Mortality and major postoperative complications within 1 year after vascular surgery: a prospective cohort study
Key words: myocardial injury after noncardiac surgery, postoperative complications, vascular surgery



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Mortality and major postoperative complications within 1 year after vascular surgery: a prospective cohort study
Introduction: Patients undergoing vascular procedures are prone to developing postoperative complications affecting their short‑term mortality. Prospective reports describing the incidence of long‑term complications after vascular surgery are lacking.
Objectives: We aimed to describe the incidence of complications 1 year after vascular surgery and to evaluate an association between myocardial injury after noncardiac surgery (MINS) and 1‑year mortality.
Patients and methods: This is a substudy of a large prospective cohort study Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION). Recruitment took place in 28 centers across 14 countries from August 2007 to November 2013. We enrolled patients aged 45 years or older undergoing vascular surgery, receiving general or regional anesthesia, and hospitalized for at least 1 night postoperatively. Plasma cardiac troponin T concentration was measured before the surgery and on the first, second, and third postoperative day. The patients or their relatives were contacted 1 year after the procedure to assess the incidence of major postoperative complications.
Results: We enrolled 2641 patients who underwent vascular surgery, 2534 (95.9%) of whom completed 1‑year follow‑up. Their mean (SD) age was 68.2 (9.8) years, and the cohort was predominantly male (77.5%). The most frequent 1‑year complications were myocardial infarction (224/2534, 8.8%), amputation (187/2534, 7.4%), and congestive heart failure (67/2534, 2.6%). The 1‑year mortality rate was 8.8% (223/2534). MINS occurred in 633 patients (24%) and was associated with an increased 1‑year mortality (hazard ratio, 2.82; 95% CI, 2.14–3.72; P <0.001).
Conclusions: The incidence of major postoperative complications after vascular surgery is high. The occurrence of MINS is associated with a nearly 3‑fold increase in 1‑year mortality.
What's new?
This substudy of a large international prospective study (Vascular Events in Noncardiac Surgery Patients Cohort Evaluation [VISION]) included more than 2600 patients who underwent noncardiac vascular surgery. It proved that major postoperative complications are common within a year after these procedures, and that the profile of the postoperative complications varies across different types of noncardiac vascular surgeries. We revealed that 1 in 12 patients dies within a year after a major noncardiac vascular procedure. Finally, our analyses showed that myocardial injury after noncardiac surgery is associated with an almost 3‑fold increase in 1‑year mortality.
Introduction
Vascular procedures are associated with the highest risk of postoperative complications among all noncardiac surgeries.1 Severe systemic atherosclerosis combined with blood loss, aortic cross‑clamping, and direct atherosclerotic plaque damage contribute to a high risk of myocardial and cerebral ischemia in vascular surgery patients.2-4
Recent observational studies have shown that myocardial injury after noncardiac surgery (MINS) is a common and prognostically important adverse event with the highest incidence among patients undergoing vascular surgery.5-9 The Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) (ClinicalTrials.gov ID: NCT00512109), the largest prospective study in this field, aimed to establish the causal relationship between MINS and 30‑day mortality. It found an association between MINS and every sixth death 30 days after noncardiac surgery.1 The majority of patients who suffer from MINS do not present with classic ischemic features, which may be masked by sedation and analgesia in the perioperative period. Indeed, the VISION study indicated that 9 out of 10 MINS diagnoses go undetected without systematic troponin screening.5 Even though the relationship between MINS and short‑term complications is well established, the data on its association with long‑term complications remain scarce.
Based on the VISION study, we aimed to analyze the incidence of short- and long‑term complications after different types of noncardiac vascular surgery and to investigate the relationship between MINS and mortality within 1 year after surgery.
Patients and methods
Study design
Details of the study design and methods were described previously.5,10 Briefly, the VISION study included patients aged at least 45 years undergoing noncardiac surgery (under general or regional anesthesia) who required hospitalization for at least 24 hours after the surgery. The study protocol complied with the Declaration of Helsinki and its further amendments. Each center had obtained an approval of their respective Bioethical Committee before the patient recruitment began. The first and the last authors’ center received an approval number KBET/74/B/2010. Eligible patients or their representatives provided written informed consent.
Study setting
The study was performed in 28 centers from 14 countries in Asia, Africa, Australia, and Europe, as well as North and South America, from August 2007 to November 2013. Screening of eligible patients was performed every day from the list of patients from preoperative assessment clinics, surgical lists (same day or the day before), and the list of patients hospitalized in surgical wards and intensive care units. The screening also included patients in the preoperative holding areas to identify those undergoing elective, urgent, or emergent surgery day and night, weekdays, and weekends. The countries and centers participating in the study are listed in Supplementary material, Table S1.
Patients, data collection, and follow‑up
The group of patients eligible for this substudy included all individuals exposed to noncardiac vascular surgery from the VISION study. The types of vascular surgery included in this study were: thoracic aorta reconstruction (n = 79; thoracic aortic aneurysm repair, repair of supra‑aortic trunks not requiring total cardiopulmonary bypass, thoracoabdominal aortic aneurism repair with or without aortofemoral bypass), aortoiliac reconstruction (n = 645; open abdominal aortic aneurysm repair, aortofemoral bypass, iliofemoral bypass, renal artery revascularization, celiac artery revascularization, superior mesenteric artery revascularization), peripheral vascular reconstruction (n = 1206; axillofemoral bypass, femoral‑femoral bypass, femoroinfragenicular bypass, profundoplasty, or other angioplasties of the infrainguinal arteries), extracranial cerebrovascular surgery (n = 434; carotid endarterectomy, carotid‑subclavian bypass), and endovascular aortic repair (n = 302). Each patient was interviewed and examined by a member of the study personnel prior to the surgery to prospectively gather baseline demographic data and clinical characteristics. Blood samples were obtained 6 to 12 hours before the surgery and on the first, second, and third postoperative day in order to measure the plasma concentration of cardiac troponin T. A majority of the participating centers (12/28) assessed high‑sensitivity troponin T (hs‑TnT), followed by centers assessing both hsTnT and non–hs‑TnT (8/28), and non‑hsTnT (8/28). The study personnel observed the patients during their hospital stay for the occurrence of the study outcomes and recorded laboratory results as well as anesthesia and discharge data. The patients or their relatives were contacted by phone 30 days and 1 year after the surgery in order to gather data on the study outcomes. The patients who did not complete 1‑year follow‑up were censored on the last day their status was confirmed.
Study outcomes
We prospectively assessed the incidence of MINS and the following outcomes at 1‑year follow‑up: mortality, myocardial infarction (MI), nonfatal cardiac arrest, stroke, venous thromboembolism, congestive heart failure, cardiac revascularization, and amputation. Additionally, we calculated the 30‑day rate of the abovementioned complications, as well as sepsis, infection without sepsis, acute kidney injury requiring dialysis, bleeding independently associated with mortality (BIMS),11 and new clinically important atrial fibrillation. MINS was defined as an elevated postoperative plasma troponin concentration adjudicated at each site according to predefined criteria as due to myocardial ischemia. Troponin elevations judged as resulting from nonischemic etiology (eg, sepsis, pulmonary embolism, atrial fibrillation, cardioversion, chronic elevation) were not recorded as MINS. The incidence of MINS was described in the entire cohort. The frequency of 30‑day complications was described in the patients with available 30‑day follow‑up (n = 2630), while the 1‑year complication rate was described in the patients with available 1‑year follow‑up (n = 2534). Detailed definitions of other outcomes are provided in Supplementary material, Appendix S1. All outcomes were adjudicated by a blinded clinical events classification committee using standardized definitions.
Statistical analysis
We used data from a large cohort study (VISION), where sample size calculations were based on the expected incidence of major cardiac complications after noncardiac surgery.5 Categorical variables were presented as numbers (percentage) and compared using the χ2 test, while continuous variables were presented as mean (SD) or median (interquartile range [IQR]) and compared using the t test or the Mann–Whitney test, depending on their distribution. Survival probability between the groups (types of surgery, occurrence of MINS) was compared using the Kaplan–Meier curves and the log‑rank test. The relationship between 1‑year mortality and MINS was evaluated using the Cox proportional hazard model. Death during 1‑year follow‑up was a dependent variable, while independent variables included MINS and clinical characteristics that are known to be associated with postoperative mortality (age, sex, diabetes, recent history of high‑risk coronary artery disease [CAD], history of congestive heart failure, active cancer, chronic obstructive pulmonary disease, and type of vascular surgery).5,10 This was a complete‑case analysis. A P value below 0.05 was considered significant. Statistical analyses were performed with R Studio packages: survival, survminer, ggplot2, amd dplyr (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
The VISION study included 40 004 patients undergoing noncardiac surgeries, and out of them 2641 (6.6%) had a vascular procedure. The patients having vascular surgeries were predominantly men (2047/2641; 77.5%) of a mean (SD) age of 68.2 (9.8) years. The most common comorbidities were hypertension (1992/2641; 75.5%), peripheral vascular disease (1782/2641; 67.5%), and CAD (1002/2641; 38.0%). Detailed demographic and clinical characteristics of the study group, along with the type of vascular surgery and anesthesia, are presented in Table 1. The follow‑ups of 30 days and 1 year were completed by 2630 (99.6%) and 2534 (95.9%) patients, respectively (Supplementary material, Figure S1). Baseline characteristics of the patients with available 30‑day and 1‑year follow‑up are provided in Supplementary material, Table S2.
Characteristics | Value (n = 2641) |
Data are presented as number (percentage) or median (interquartile range) unless otherwise indicated.
a The number of patients with 2 types of vascular procedures was 23, and the number of patients with 3 types of vascular procedures was 1.
Abbreviations: ACE, angiotensin‑converting enzyme; DVT, deep vein thrombosis; PE, pulmonary embolism | |
Age, y, mean (SD) | 68.2 (9.8) |
45–54, y | 238 (9) |
55–64, y | 721 (27.3) |
65–74, y | 931 (35.3) |
75–84, y | 650 (24.6) |
≥85, y | 101 (3.8) |
Male sex | 2047 (77.5) |
Body mass index, kg/m2 (n = 2475) | 25.8 (23.2–29) |
Frailty (n = 2619) | 222 (8.5) |
Comorbidities | |
Coronary artery disease (n = 2638) | 1002 (38) |
Recent high‑risk coronary artery disease | 54 (2) |
Congestive heart failure (n = 2639) | 215 (8.1) |
Previous DVT/PE (n = 2636) | 111 (4.2) |
Previous cerebrovascular event | 524 (19.8) |
Atrial fibrillation (n = 2631) | 179 (6.8) |
Hypertension (n = 2640) | 1992 (75.5) |
Peripheral vascular disease | 1782 (67.5) |
Chronic obstructive pulmonary disease | 700 (26.5) |
Diabetes (n = 2639) | 675 (25.6) |
Preoperative estimated glomerular filtration rate, ml/min/1.73 m2 (n = 2567) | |
>60 | 1712 (69.7) |
45–60 | 377 (15.3) |
30–44 | 253 (10.3) |
<30 | 116 (4.7) |
Medications <24 hours prior to surgery | |
Acetylsalicylic acid (n = 2631) | 754 (28.7) |
ACE inhibitors (n = 2633) | 1089 (41.4) |
β-Blockers (n = 2633) | 982 (37.3) |
Statins (n = 2632) | 1687 (64.1) |
Medications <7 days prior to surgery | |
Acetylsalicylic acid (n = 2637) | 1682 (63.8) |
ACE inhibitors (n = 2639) | 1464 (55.5) |
β-Blockers (n = 2639) | 1074 (40.7) |
Statins (n = 2639) | 1951 (73.9) |
Type of anesthesia (n = 2636) | |
General | 1357 (51.5) |
Neuraxial | 996 (37.8) |
Other | |
Type of surgerya | 283 (10.7) |
Thoracic aorta reconstruction | 79 (3) |
Aortoiliac reconstruction | 645 (24.4) |
Peripheral vascular reconstruction | 1206 (45.7) |
Extracranial cerebrovascular surgery | 434 (16.4) |
Endovascular aortic repair | 302 (11.4) |
Urgent / emergent surgery | 134 (5.1) |
Incidence of major postoperative complications
The most common complications after vascular surgery at 30 days were BIMS (662/2630; 25.2%), followed by MINS (633/2641; 24%), and MI (223/2630; 8.5%). The 30‑day mortality was 2.8% (73/2630). The incidence of 30‑day complications stratified by the type of vascular surgery is summarized in Supplementary material, Table S3.
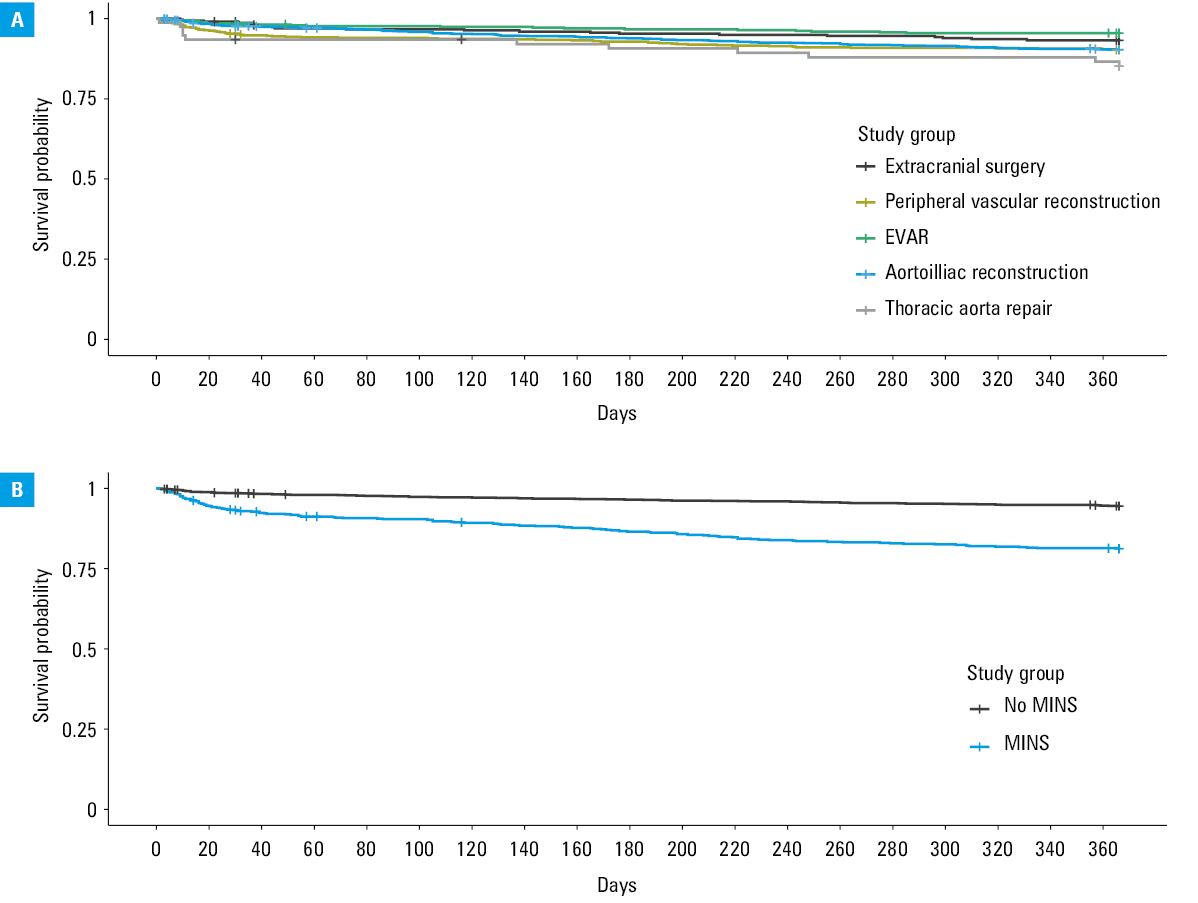
The incidence of 1‑year complications varied depending on the type of vascular surgery (Table 2). In the entire cohort, the most frequent 1‑year complications were MI (224/2534; 8.8%), amputation (187/2534; 7.4%), and congestive heart failure (67/2534; 2.6%). The mortality rate at 1‑year was 8.8% (223/2534). The lowest mortality rate was observed in the patients exposed to extracranial cerebrovascular surgery (4.9%), and the highest in those undergoing thoracic aorta repair (14.5%) (Figure 1). The incidence and median time to event for all postoperative complications, stratified by the type of vascular surgery, are presented in Table 2.
Complication | Thoracic aorta repair (n = 76) | Aortoiliac reconstruction (n = 629) | Peripheral vascular reconstruction without aortic cross‑clamping (n = 1149) | Extracranial cerebrovascular surgery (n = 412) | EVAR (n = 293) | All patients (n = 2534) | Median time to event in the entire cohort, d |
Frequency is presented as number (percentage) and time to event as median (interquartile range). The 1‑year complication rate is provided in patients with available 1‑year follow‑up data (n = 2534). The number of patients with 2 types of vascular procedures was 23, and the number of patients with 3 types of vascular procedures was 1.
Abbreviations: EVAR, endovascular aortic repair | |||||||
Death | 11 (14.5) | 63 (10) | 112 (9.3) | 20 (4.9) | 20 (6.8) | 223 (8.8) | 96 (18.5–212) |
Myocardial infarction | 7 (9.2) | 77 (12.2) | 91 (7.9) | 25 (6.1) | 26 (8.9) | 224 (8.8) | 1 (1–2) |
Nonfatal cardiac arrest | 2 (2.6) | 7 (1.1) | 6 (0.5) | 2 (0.5) | 0 | 17 (0.7) | 4.5 (2.25–50.25) |
Stroke | 2 (2.6) | 9 (1.4) | 11 (1) | 10 (2.4) | 1 (0.3) | 33 (1.3) | 6 (1.5–28.5) |
Congestive heart failure | 4 (5.3) | 26 (4.1) | 18 (1.6) | 10 (2.4) | 9 (3.1) | 67 (2.6) | 5.5 (3–64) |
Venous thromboembolism | 1 (1.3) | 7 (1.1) | 12 (1) | 3 (0.7) | 2 (0.7) | 25 (1) | 18 (7–57) |
Cardiac revascularization | 1 (1.3) | 13 (2.1) | 25 (2.2) | 13 (3.2) | 8 (2.7) | 60 (2.4) | 59 (16–190) |
Amputation | 2 (2.8) | 14 (2.2) | 171 (14.9) | 1 (0.2) | 0 | 187 (7.4) | 50 (13–135.25) |
Abbreviations: see Table 2
Association between myocardial injury after noncardiac surgery and 1‑year complications
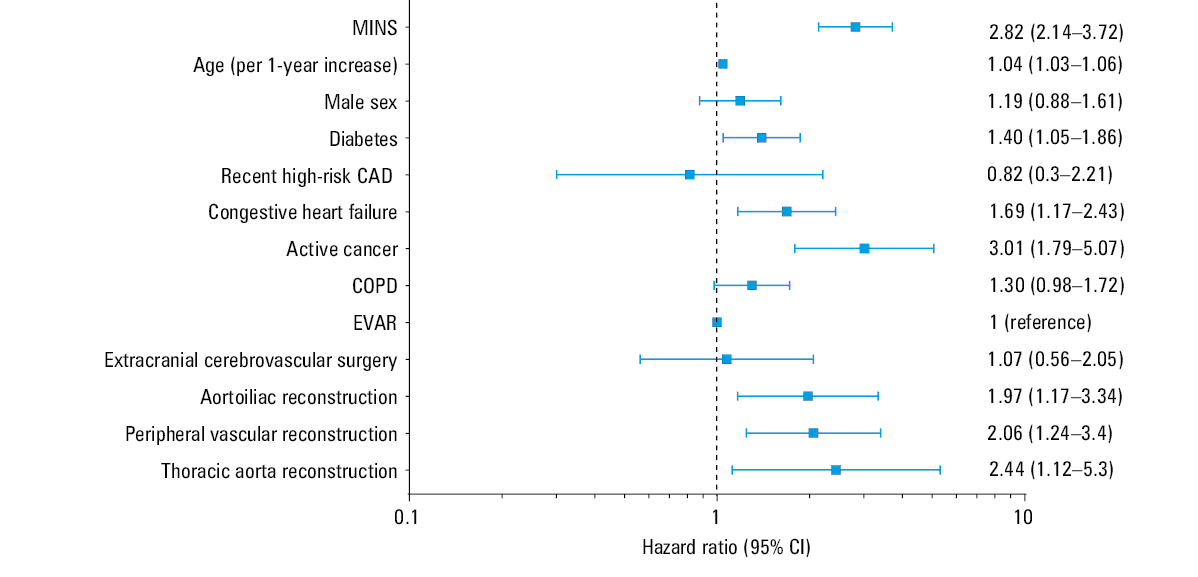
MINS occurred in 633 patients (24%) following major vascular surgery. Its incidence varied from 15.4% after extracranial cerebrovascular surgery to 31.6% after aortoiliac reconstruction. The median (IQR) time to MINS occurrence was 2 (1–3) days. Preoperative serum troponin was measured in 1303 patients (49.3%). MINS incidence did not differ depending on availability of preoperative troponin measurements (24.7% vs 23.2%; P = 0.4). There was also no difference in MINS incidence between the centers using only hs‑TnT, both hs‑TnT and non–hs‑TnT, and only non–hs‑TnT measurements (22.6% vs 24.9% vs 26.9%, respectively; P = 0.14). Details on troponin assays and their association with MINS incidence are summarized in Supplementary material, Table S4. One‑year mortality was significantly higher among the patients who developed MINS than in those who did not (19.2% vs 5.6%; log‑rank test with P <0.001). The Kaplan–Meier curve presenting crude survival probability stratified by the incidence of MINS is presented in Figure 1. A multivariable analysis (Figure 2) showed that after adjustment for prognostically important clinical variables and the type of vascular surgery, MINS was associated with an increase in 1‑year mortality (hazard ratio, 2.82; 95% CI, 2.14–3.72; P <0.001). The incidence of other major complications stratified by MINS is reported in Table 3.
Abbreviations: see Table 2
Complication | Follow‑upa | MINS | Non‑MINS | P value |
Data are presented as number (percentage).
a Frequency of 30‑day complications is provided for patients with available 30‑day follow‑up data (n = 2630, including 630 patients with MINS and 2000 patients without MINS), while the 1‑year complication rate is provided for patients with available 1‑year follow‑up data (n = 2534, including 600 patients with MINS and 1934 patients without MINS).
Abbreviations: AKI, acute kidney injury; BIMS, bleeding independently associated with mortality after noncardiac surgery; MINS, myocardial injury after noncardiac surgery | ||||
Sepsis | 30‑day | 70 (11.1) | 70 (3.5) | <0.001 |
Infection without sepsis | 30‑day | 61 (9.7) | 91 (4.6) | <0.001 |
AKI with dialysis | 30‑day | 17 (2.7) | 8 (0.4) | <0.001 |
BIMS | 30‑day | 282 (44.8) | 380 (19) | <0.001 |
New, clinically important atrial fibrillation | 30‑day | 29 (4.6) | 18 (0.9) | <0.001 |
Death | 30‑day | 43 (6.8) | 30 (1.5) | <0.001 |
1‑year | 115 (19.2) | 108 (5.6) | <0.001 | |
Myocardial infarction | 30‑day | 196 (31.2) | 27 (1.4) | <0.001 |
1‑year | 191 (31.9) | 33 (1.7) | <0.001 | |
Nonfatal cardiac arrest | 30‑day | 9 (1.4) | 3 (0.1) | <0.001 |
1‑year | 13 (2.2) | 4 (0.2) | <0.001 | |
Stroke | 30‑day | 12 (1.9) | 13 (0.7) | 0.01 |
1‑year | 15 (2.5) | 18 (0.9) | 0.01 | |
Congestive heart failure | 30‑day | 35 (5.6) | 12 (0.6) | <0.001 |
1‑year | 44 (7.3) | 23 (1.2) | <0.001 | |
Venous thromboembolism | 30‑day | 5 (0.8) | 11 (0.5) | 0.69 |
1‑year | 10 (1.7) | 15 (0.8) | 0.09 | |
Cardiac revascularization | 30‑day | 16 (2.5) | 6 (0.3) | <0.001 |
1‑year | 31 (5.2) | 29 (1.5) | <0.001 | |
Amputation | 30‑day | 25 (4) | 56 (2.8) | 0.18 |
1‑year | 53 (8.8) | 134 (6.9) | 0.14 | |
Discussion
In this large, prospective, international study that included more than 2600 patients who underwent noncardiac vascular surgery, the incidence of postoperative complications was high and varied considerably depending on the type of procedure. Furthermore, 1‑year mortality was independently associated with MINS in this population.
Postoperative complications after noncardiac surgery are associated with increased short‑term mortality, and their incidence is particularly high among patients undergoing vascular procedures.1,12 In this cohort, the most common postoperative complications were BIMS and MINS, each of which occurred in a quarter of patients. MINS was common following all forms of surgery, but it was most prevalent in the patients who underwent thoracic aortic repair or aortoiliac reconstruction, where the rate was approximately 30%. MINS was associated with the occurrence of all 30‑day and 1‑year complications except for venous thromboembolism and amputation. Our 1‑year data demonstrated that nearly 9% of the vascular surgical patients developed MI, and more than 7% underwent amputation within this time. The postoperative complication rates were the highest following the procedures involving the aorta. These procedures carry an intrinsically high risk because of the invasive nature of the surgery. Manipulations involving the aorta and aortic cross‑clamping increase the risk of arterial thromboembolism. Additional risk comes from frequent presence of comorbidities, such as CAD, cerebrovascular disease, chronic kidney disease, diabetes mellitus, and chronic obstructive pulmonary disease, all of which were prevalent in this study cohort. The advent of endovascular aortic repair (EVAR) has reduced the rate of procedural complications, as compared with open surgery in the subgroup of patients who required intervention for abdominal aortic aneurysm. However, not all patients are technically suitable for the procedure. It involves administration of X‑ray contrast with the associated risk of contrast‑induced nephropathy, and bleeding, which occurred in 17.8% of our EVAR patients, remains a potential problem. The requirement for amputation was infrequent (0%–2.8%) following most types of the surgery, but its rate was appreciable (6.2% at 30 days and 14.9% at 1 year) after peripheral vascular surgery. The incidence of stroke was generally low. It occurred most commonly after extracranial cerebrovascular surgery, following which the 30‑day and 1‑year stroke rates were nearly 3%. There are several potential etiologies for the requirement for postoperative amputation and the occurrence of postoperative stroke, but there is an obvious direct link between surgery on the arteries supplying the extremities and the brain and ischemic complications in the subtended arterial territory. The variation in complication rates following different types of vascular surgery was noticeable and suggests that postoperative monitoring for complications should be tailored according to the type of procedure.
Based on the currently available evidence, predominantly from retrospective and registry‑based studies, long‑term mortality after vascular surgery ranges from 4.2% to 11%.13-16 Our study revealed that approximately 1 in 12 patients die within a year of vascular surgery. Similarly to the nonfatal complication rates, the mortality rate depended on the type of vascular procedure and ranged from 4.9% after extracranial cerebrovascular procedures to 14.5% in the patients who underwent repair of thoracic aorta, although the number of events per surgical procedure is too low to stratify the risk accurately. Postoperative complications, particularly those involving the cardiovascular system, are important predictors of long‑term mortality after vascular procedures.17-19 A recently published large retrospective cohort study showed that perioperative MI (PMI) was associated with a more than 5‑fold increase in 1‑year mortality after vascular surgery. This is particularly alarming in light of virtually constant incidence of PMI in this population in the last decade.19,20 Higher incidence of PMI in the current study than in the previous reports is most probably associated with a routine perioperative troponin monitoring, thus showing the extent of underdiagnosis of this crucial outcome.21
The observed high incidence of postoperative cardiac complications suggests that this population requires a meticulous and accurate preoperative cardiovascular risk assessment. This phenomenon has already been taken into account in the currently used risk stratification tools. The Revised Cardiac Risk Index (RCRI) categorizes patients undergoing suprainguinal vascular procedures as high‑risk, while the National Surgical Quality Improvement Program Myocardial Infarction and Cardiac Arrest (NSQIP MICA) assigns the highest risk coefficient to aortic surgeries (1.6 points) and increased risk to peripheral vascular surgeries (0.86 points).22,23 The recently proposed American University of Beirut HAS2 Cardiovascular Risk Index simplified this issue and considered all vascular surgeries high‑risk procedures.24 However, there is still room for improvement in this area, as both RCRI and NSQIP MICA are known to significantly underestimate the postoperative cardiac risk in vascular surgery.25
In recent years it has been shown that MINS, that is, postoperative troponin elevation irrespective of symptoms or electrocardiographic changes, is associated with increased short- and long‑term mortality after noncardiac surgery.26-28 Further analyses revealed that MINS occurs most commonly after vascular procedures, and is one of the most critical factors contributing to short‑term mortality in the noncardiac surgery population.1,29
We have confirmed that MINS is an important predictor of 1‑year mortality in the patients undergoing vascular surgery. Perioperative troponin monitoring should be considered in the patients undergoing vascular surgery, particularly in light of limited accuracy of risk prediction tools in individual patients.30,31 Not only does MINS predict risk, but it also identifies the patients who may benefit from novel interventions aimed at modifying their adverse prognosis.32,33
To our knowledge, this is the largest prospective study describing the incidence of major postoperative complications and long‑term mortality in the patients undergoing a wide range of vascular procedures. Another strength of this study is its very high 1‑year follow‑up completion rate. Moreover, routine troponin monitoring enabled reliable assessment of PMI and MINS incidence. In summary, this manuscript offers a comprehensive insight into the profile of long‑term complications in the population of patients undergoing vascular procedures.
We are aware of several limitations of this study. Firstly, the rate of 1‑year follow‑up complications was determined by telephone calls with patients or their relatives, which could potentially lead to underestimation (or possibly overestimation) of the incidence of some complications. However, the risk of underestimating 1‑year mortality was low in view of the high rate of follow‑up achieved and a clear binary nature of this outcome. Secondly, although this was a large cohort of patients undergoing vascular surgery, the number of individuals who underwent thoracic aorta repair was low. This limited the precision with which risk estimates could be made for this procedure. Thirdly, the study was performed between 2007 and 2013, and surgical practices and techniques may have changed (eg, the number of available endovascular techniques increased). Moreover, there were some important developments in our knowledge about perioperative troponin release in noncardiac surgery as well as perioperative practices concerning medications. For this reason, the study results may not represent the most current clinical practice, and may possibly overestimate the rate of complications. Nevertheless, we suspect that the profile of complications associated with each type of surgery would not change. Finally, preoperative troponin measurement was missing in a significant proportion of the study participants (50.7%). This could potentially impact the frequency of MINS and MI because the dynamics of troponin levels are taken into account in the diagnosis of these complications. Moreover, a lack of preoperative troponin results hinders differentiating acute and chronic troponin elevation. Importantly, we did not find any association between preoperative troponin level availability and MINS rate.
Conclusions
This large prospective cohort study showed that patients undergoing noncardiac vascular surgery commonly develop postoperative complications within 1 year from the procedure. The distribution of postoperative adverse events varied across different types of procedures. MINS occurred in 24% of the patients and was independently associated with 1‑year mortality.
- Spence J, LeManach Y, Chan MTV, et al. Association between complications and death within 30 days after noncardiac surgery. CMAJ. 2019; 191: E830‑E837. | Crossref
- McGinigle KL, Spangler EL, Pichel AC, et al. Perioperative care in open aortic vascular surgery: a consensus statement by the Enhanced Recovery After Surgery (ERAS) Society and Society for Vascular Surgery. J Vasc Surg. 2022; 75: 1796‑1820. | Crossref
- Lasek‑Bal A, Urbanek T, Puz P, et al. Cerebral embolism in the perioperative period in patients post interventional treatment of carotid artery stenosis: a preliminary report. Kardiol Pol. 2014; 72: 783‑789. | Crossref
- Latacz P, Simka M, Bryll A, et al. Cerebral ischemic lesions on diffusion‑weighted magnetic resonance imaging after carotid eversion endarterectomy vs carotid stenting with a proximal protection device: results of a randomized prospective trial. Pol Arch Intern Med. 2019; 129: 562‑566. | Crossref
- Devereaux PJ, Biccard BM, Sigamani A, et al. Association of postoperative high‑sensitivity troponin levels with myocardial injury and 30‑day mortality among patients undergoing noncardiac surgery. JAMA. 2017; 317: 1642‑1651.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION