24-hour urine metanephrine excretion in patients diagnosed with adrenal incidentaloma: impact of commonly used drugs on a clinical decision
2 ,
Key words: drug interference, incidentaloma, metanephrines, pheochromocytoma
,
Key words: drug interference, incidentaloma, metanephrines, pheochromocytoma

 CC BY 4.0
CC BY 4.0
24-hour urine metanephrine excretion in patients diagnosed with adrenal incidentaloma: impact of commonly used drugs on a clinical decision
Introduction: Incidentaloma is an adrenal tumor detected during diagnostic imaging performed for extra‑adrenal causes. Evaluation of metanephrine concentrations in a 24‑hour urine collection can be a significant challenge in patients with multiple medications and comorbidities.
Objectives: The aim of this study was to evaluate the effect of commonly used groups of drugs on metanephrine levels in the 24‑hour urine collection.
Patients and methods: A total of 1051 patients with adrenal mass below 10 Hounsfield units on unenhanced computed tomography were included in the study. Patients diagnosed with Cushing or Conn syndrome, adrenal carcinoma, pheochromocytoma, active extra‑adrenal malignant neoplasms, and exacerbation of severe illnesses were excluded. Metanephrine, normetanephrine, and 3‑methoxytyramine in the 24‑hour urine collection were measured by high‑performance liquid chromatography with electrochemical detection. Information on concomitant medication (β-blockers, calcium channel blockers [CCBs], loop diuretics, thiazide diuretics, potassium‑sparing diuretics, α-blockers, angiotensin‑converting enzyme inhibitors / angiotensin II receptor blockers, metformin, nonmetformin antidiabetic drugs [NMADs], lipid‑lowering drugs, proton pump inhibitors, levothyroxine, thyreostatics, antidepressants, neuroleptics, benzodiazepines, glucocorticosteroids, inhaled B‑receptor agonists, and ipratropium) was collected from each patient.
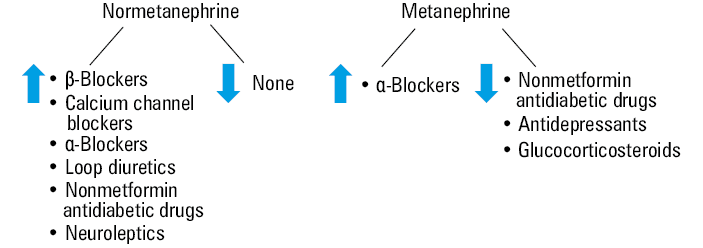
Results: The urinary excretion of normetanephrine was significantly higher in the patients on β-blockers, CCBs, loop diuretics, α-blockers, NMADs, and neuroleptics. α-Blockers increased urine metanephrine concentration, and NMADs, antidepressants, and glucocorticosteroids lowered it. There was no association between the analyzed drugs and urinary 3‑methoxytyramine level.
Conclusions: Many drug groups interfere with the measurement of urinary fractionated metanephrines. These interactions should be taken into account during interpretation of a hormonal evaluation, as they can be crucial for further management, especially for making a decision on surgical treatment.
What's new?
The number of adrenal incidentalomas detected has increased in recent years. Drug interactions with urine metanephrine concentration assessment have been known for a long time; however, data are not fully consistent. Therefore, this study, conducted in a large cohort of patients, aimed to indicate which groups of drugs should be used preferentially during urine collection to make interpretation of the results reliable and clinically useful.
Introduction
Incidentaloma is defined as an adrenal mass larger than 1 cm, detected during diagnostic imaging performed for reasons other than a suspicion of adrenal diseases.1-3 Adrenal incidentalomas (AIs) are found in 1% to 6% of adults, and the frequency of their detection has increased with the advances of imaging diagnostics and with the age of the population.4 There is no difference in incidentaloma occurrence between sexes.5 They are very rare in children, less than 1% of cases occur before 30 years of age, 4% before the age of 50 years, and the frequency increases to 7%–10% in patients over 70 years of age.6 Substantial advances in imaging techniques, such as ultrasonography, magnetic resonance, or computed tomography (CT), resulted in about 10‑fold increase in detection of adrenal lesions in the past 2 decades.1,7 Once a lesion is detected, further testing is needed to determine whether it is benign or malignant, and whether the tumor is hormonally active or not. Such diagnostics must be performed urgently in children, pregnant women, and adults under 40 years of age, because in these populations a risk of malignancy is higher.6 Hormonal evaluation includes an overnight 1‑mg dexamethasone suppression test, a 24‑hour urine collection of fractionated metanephrines, or measurement of plasma‑free metanephrines, and plasma aldosterone / renin ratio in hypertensive patients.6,8
According to the literature, the most common among AIs are adrenocortical adenomas (80%–85%), including nonfunctional lesions (40%–70%), mild autonomous cortisol‑secreting tumors (20%–50%), primary aldosteronism (2%–5%), and overt Cushing syndrome (1%–4%). Pheochromocytomas (1%–5%), metastases (3%–7%), or adrenocortical carcinomas (0.4%–4%) can also be found.9
Each year, more than 500 patients with newly‑diagnosed AIs are referred to our center for hormonal workup. The main clinical issues are hormonal activity imbalance and oncologic risk assessment. The new European Society of Endocrinology (ESE) clinical practice guideline on the management of adrenal incidentalomas developed in collaboration with the European Network for the Study of Adrenal Tumors (ENSAT) suggests measurement of plasma free metanephrines or urinary fractionated metanephrines to exclude pheochromocytoma in patients with homogenous adrenal masses with Hounsfield units (HUs) above 10 on unenhanced CT.9
Modern assays for the measurement of urinary metanephrine concentration include high‑performance liquid chromatography with electrochemical detection (HPLC‑ECD) or mass spectrometry after HPLC separation (HPLC‑MS). Electrochemical quantification is very sensitive but drug interference can occur. MS has higher sensitivity and higher specificity but its cost is higher and availability limited.10 New technologies for metanephrine measurement have made some of the previous recommendations no longer valid.
Comorbidities, such as renal failure, ischemic stroke, intracerebral hemorrhage, decompensated congestive heart failure, and obstructive sleep apnea have also been reported to affect plasma and urinary metanephrine and normetanephrine concentrations.11-15
False‑positive results due to comorbidities and drug interference often cause diagnostic dilemmas and generate additional costs. For many years, researchers have reported on the effects of different groups of drugs on plasma metanephrine concentrations and / or their urine excretion,16-18 but the exact effects of drugs on metanephrine measurement by more sensitive and specific methods have not been documented or confirmed.
The aim of this retrospective, observational study was to evaluate the effect of commonly used drugs on the 24‑hour urinary metanephrine excretion in patients with incidentalomas using HPLC‑ECD.
Patients and methods
A database search was performed for AI patients, diagnosed and treated at the Department of Endocrinology, Oncological Endocrinology and Nuclear Medicine, University Hospital in Kraków in the years 2017–2020. Out of 1344 recorded patients, 1051 were enrolled in the final analysis. Patients with diagnosed hormonal disturbances (Cushing disease, Conn disease, and pheochromocytoma), malignancy (adrenal carcinoma or other cancers), and with adrenal mass above 10 HUs were excluded (Figure 1). Only the patients in stable condition, without exacerbation of concomitant diseases and with extra‑adrenal malignant neoplasms in remission for more than 5 years were included in the analysis.
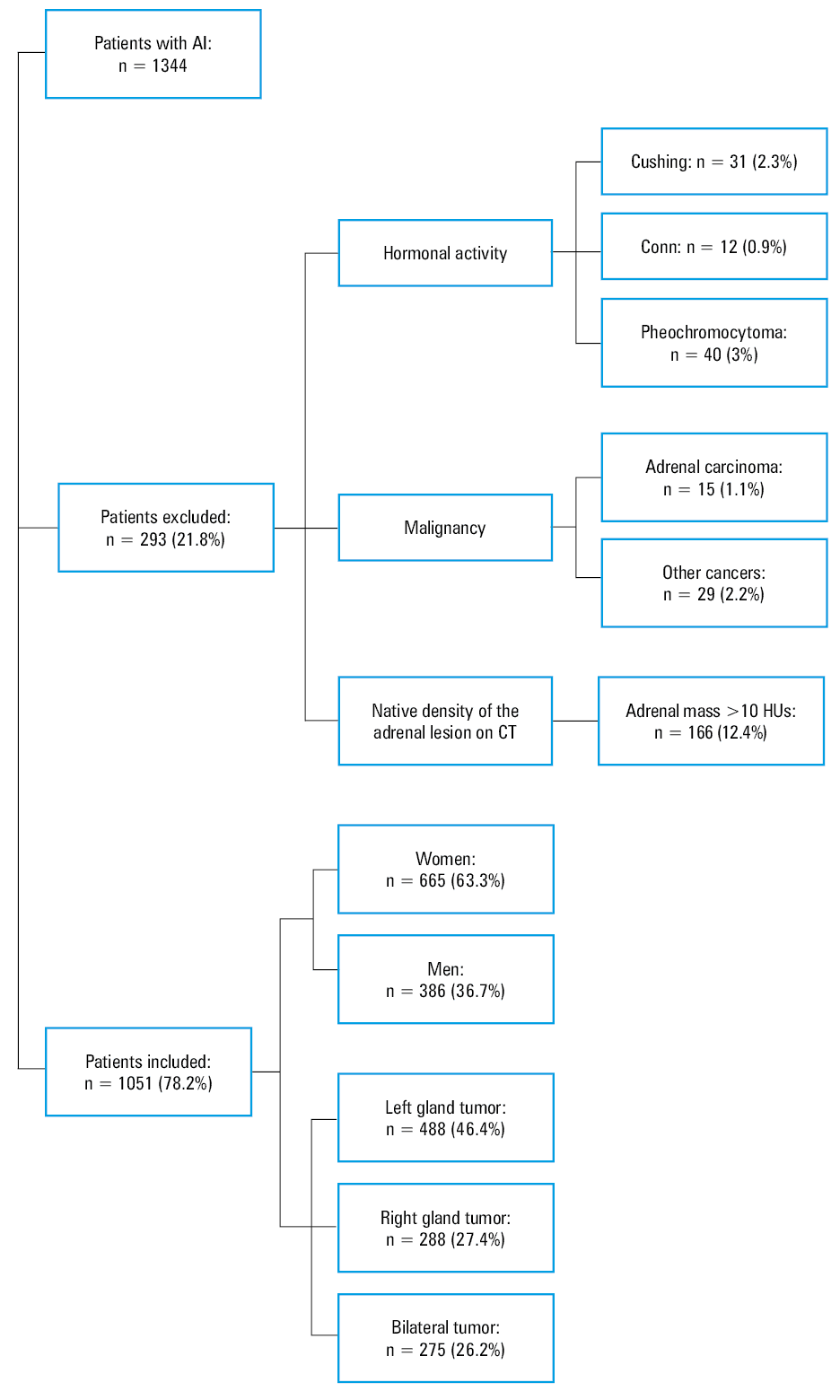
Abbreviations: AI, adrenal incidentaloma; CT, computed tomography; HU, Hounsfield unit
The analyzed group of patients included 665 women (63.3%) and 386 men (36.7%). A tumor of the left adrenal gland, right adrenal gland, and bilateral tumors were detected in 488 patients (46.4%), 288 patients (27.4%), and 275 patients (26.2%), respectively. The median age was 65 years (interquartile range [IQR], 18–88 years).
Hormonal workup involved 1‑mg overnight dexamethasone suppression test and measurement of urinary metanephrine excretion in all cases. In the patients with concomitant hypertension or hypokalemia, the aldosterone / renin ratio was used to exclude primary hyperaldosteronism.
As per our clinical routine, all patients followed a special diet low in tyramine‑containing products for 2 weeks before and during the 24‑hour urine collection. They were given precise written guidelines on the products they should avoid, so as not to interfere with the hormonal evaluation (bananas, chocolate, blue cheese, red wine).19 On admission, all the patients declared following the diet. Metanephrine, normetanephrine, and 3‑methoxytyramine were measured by HPLC‑ECD (CompleteKit, Metanephrines in Urine, Recipe, Munich, Germany) at the Clinical Biochemistry Department of Pediatric Institute, Jagiellonian University Medical College, Kraków, Poland.
The method performance was assessed in the Randox International Quality Assessment Scheme (Randox, Crumlin, United Kingdom) for urinary metanephrines. The reference ranges were 52–341 µg/24 h for metanephrine, 88–440 µg/24 h for normetanephrine, and 0–220 µg/24 h for 3‑methoxytyramine.
Information on the medications taken by the patients was collected from their detailed medical history. None of the patients used acetaminophen during hospitalization. Nineteen most common groups of drugs were selected for the analysis, and they included β-blockers (449 patients), CCBs (518 patients), loop diuretics (106 patients), thiazide diuretics (193 patients), potassium‑sparing diuretics (66 patients), α-blockers (152 patients), angiotensin‑converting enzyme inhibitors (ACEIs) / angiotensin II receptor blockers (ARBs; 352 patients), metformin (254 patients), nonmetformin antidiabetic drugs (NMADs; 96 patients), lipid‑lowering drugs (LLDs; 441 patients), proton pump inhibitors (PPIs; 213 patients), levothyroxine (LT4; 165 patients), thyreostatics (14 patients), antidepressants (84 patients), neuroleptics (18 patients), benzodiazepines (BDZs; 53 patients), glucocorticosteroids (GCSs; 89 patients), inhaled B‑receptor agonists (109 patients), and ipratropium (65 patients). As many as 132 patients denied using any drugs.
Statistical analysis
STATISTICA 13.3 software (TIBCO Software Inc., Palo Alto, California, United States) was used to calculate statistical significance. First, we checked normality of the data distribution with the Shapiro–Wilk test and homogeneity of variances with the Levene test. Taking into account that distribution of metanephrine excretion was not normal in some groups of patients, we decided to use the nonparametric Mann–Whitney test for the first stage of the statistical data analysis to compare the results in the patients taking and not taking individual drugs. To avoid false conclusions due to the use of different drugs, a multivariate analysis was performed with the ς test with constraints (multivariate general linear model: multivariate analysis of variance). A P value below 0.05 was deemed significant. Drug groups that did not show significance between the patients taking and not taking the drugs in the Mann–Whitney test were not included in the multivariate analysis.
Origin 2021 (OriginLab Corporation, Northampton, Massachusetts, United States) and Microsoft PowerPoint (Microsoft, Redmond, Washington, United States) were used to draw the graphs presented in the text.
Ethics statement
The study protocol was approved by the Local Ethics Committee of the Jagiellonian University in Kraków (1072.6120.81.2021). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Results
Twenty four‑hour normetanephrine excretion in relation to drug use
Medians and IQRs of the 24‑hour normetanephrine excretion in the patients with incidentaloma taking different drugs are presented in Figure 2. In the first stage of the analysis (the Mann–Whitney test), the difference between the patients taking and not taking the same drugs was significant for β-blockers (P <0.001), CCBs (P <0.001), loop diuretics (P <0.001), thiazide diuretics (P <0.001), α-blockers (P <0.001), metformin (P <0.001), NMADs (P = 0.002), LLDs (P <0.001), PPIs (P = 0.02), and neuroleptics (P = 0.03). Multivariate analysis showed significance for 6 of the 10 groups: β-blockers (P = 0.02), CCBs (P <0.001), loop diuretics (P = 0.007), α-blockers (P = 0.02), MNADs (P = 0.02), and neuroleptics (P = 0.04). Increased urinary excretion of normetanephrine was observed in all patients taking the abovementioned drugs (Figure 2). No difference in 24‑hour normetanephrine excretion was found between the patients taking and not taking thiazide diuretics, metformin, LLDs, and PPIs.
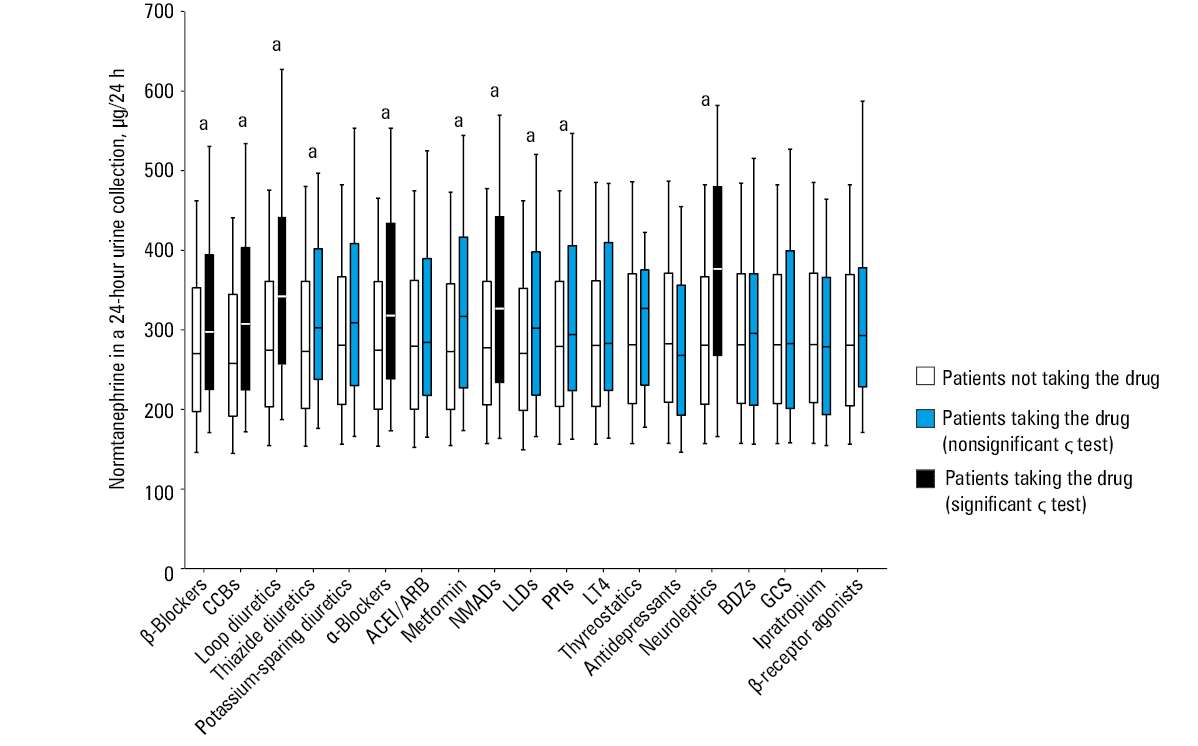
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BDZs, benzodiazepines, CCBs, calcium channnel blockers; GCS, glucocorticosteroid, LLDs, lipid‑lowering drugs; LT4, levothyroxine; NMADs, nonmetformin antidiabetic drugs; PPIs, proton pump inhibitors
Twenty four‑hour metanephrine excretion in relation to drug use
Medians and IQRs of the 24‑hour metanephrine excretion in the patients with incidentaloma using different drugs are presented in Figure 3. In the first stage of the analysis (the Mann–Whitney test), the difference between the patients taking and not taking the same drugs was significant only for α-blockers (P <0.001), NMADs (P = 0.03), antidepressants (P = 0.01), and GCSs (P = 0.03). Multivariate analysis showed significant differences for α-blockers (P <0.001), NMADs (P = 0.007), antidepressants (P = 0.02), and GCSs (P = 0.01). In the patients taking α-blockers, increased urinary metanephrine excretion was observed, while in those taking NMADs, antidepressants, or GCSs, urinary metanephrine excretion was lower than in the individuals not taking these drugs.
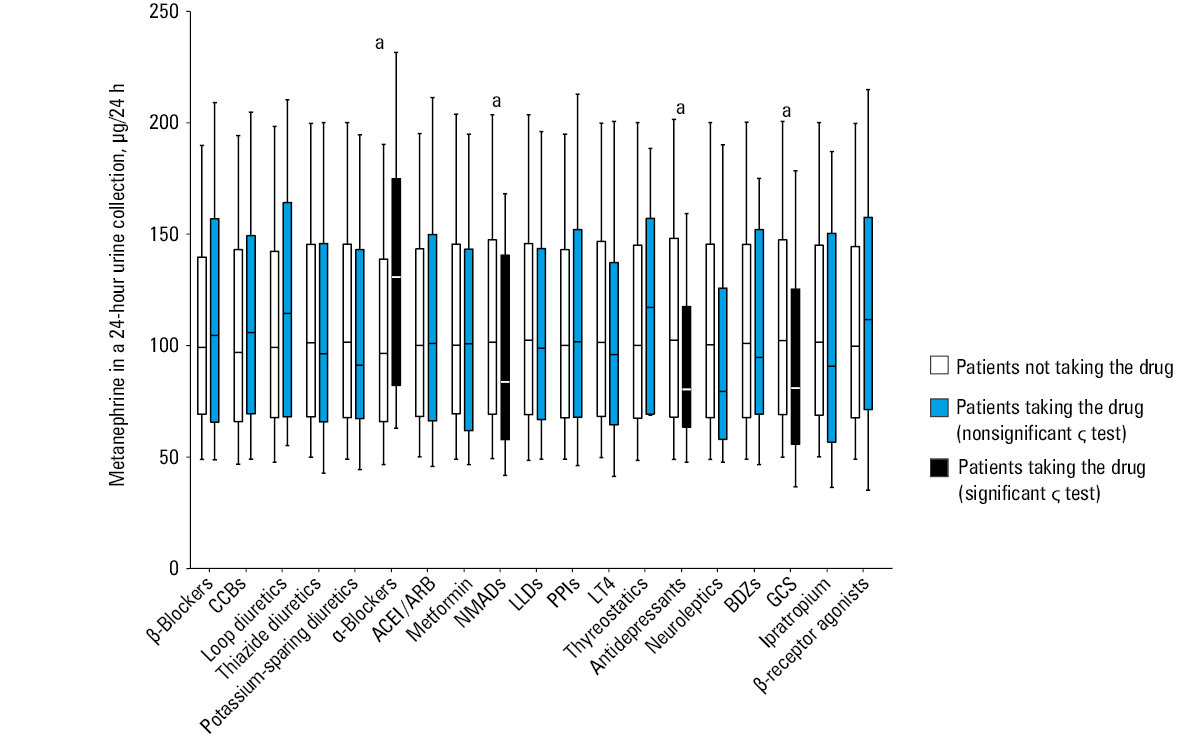
Abbreviations: see Figure 2
Twenty four‑hour 3‑metoxytyramine excretion in relation to drug use
No differences were seen in the patients taking and not taking the analyzed drugs (except LT4 in the Mann–Whitney test; P = 0.04; no significance in multivariate analysis) with reference to 3‑metoxytyramine excretion (Figure 4).
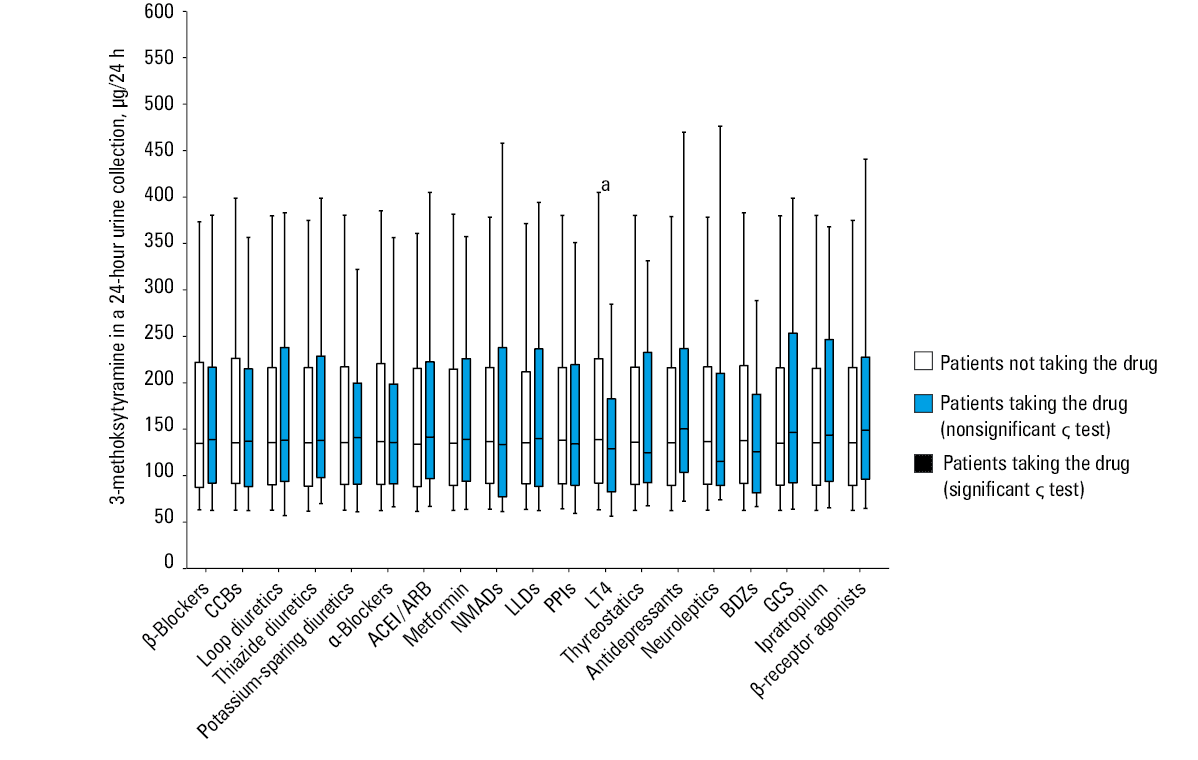
Abbreviations: see Figure 2
Discussion
Although the updated ESE/ENSAT guidelines for the management of AIs9 are likely to reduce the number of metanephrine evaluations, data on the impact of different drugs on these outcomes remain crucial in differential diagnosis in patients at a higher oncologic risk (adrenal masses >10 HUs on unenhanced CT). The effect of drugs on metanephrine excretion results should be taken into consideration, as it is essential for patient management, including decisions on surgical intervention or observation.20
In this study, of 19 the most commonly used drug groups analyzed in a large cohort, a significant impact on metanephrine concentration in the 24‑hour urine collection was found for β- and α-blockers, CCBs, loop diuretics, NMADs, neuroleptics, GCSs, and antidepressants (Figure 5).
The effect of β-blockers on metanephrine excretion can be explained biochemically. Activation of β1- and β2-adrenergic receptors can stimulate the activity of protein kinase A (PKA) through the Gs pathway, which involves adenyl cyclase and cyclic adenosine monophosphate (cAMP).21 Phenylethanolamine N‑methyltransferase (PNMT) is the final enzyme necessary to convert norepinephrine to epinephrine in the catecholamine biosynthesis pathway.22 cAMP and PKA increase the expression of early growth response protein 1.22 In this mechanism, they activate the promoter of the PNMT gene.22Thus, lowering the cAMP and PKA activity during β-blocker use probably results in a lower activity of PNMT leading to higher norepinephrine concentration. Parasiliti‑Caprino et al17 showed that patients with higher urinary normetanephrine excretion were more likely to be treated with β-blockers. It is still under debate whether this is just an effect of drug use or a sympathetic stimulation caused by comorbidities.
Literature data suggest a significantly higher impact of α1-blockers, CCBs, and loop diuretics on urine normetanephrine concentration.17,23 Another experimental study by Yoshida et al23 showed the effect of furosemide on increasing blood norepinephrine levels in rats. Reflex sympathetic stimulation is the most likely explanation for α-blocker–induced increase of metanephrine concentration in urine.18
Our study demonstrated an impact of NMADs on the urinary normetanephrine and metanephrine excretion. The mechanism is not entirely clear, but similar observations were reported previously.16,24 An explanation proposed by Hsu et al24 suggests that sulfonylureas inhibit release of catecholamines from the adrenal glands. The observed impact of antidepressants on catecholamine metabolites in our study may be partially explained based on Giatti’s et al25 observation that paroxetine, one of the antidepressants, interacts with PNMT, reduces its level, and leads to decreased epinephrine excretion. Endogenous glucocorticoids stimulate the activity of PNMT, necessary for the final step of epinephrine synthesis.22
Surprisingly, in our study the use of GCSs was associated with a reduction of urine metanephrine levels. However, no significant effect of GCSs on normetanephrine concentration has been demonstrated. The results of our study indicate the need to further understand the mechanisms of the effects of GCSs on urinary metanephrine concentrations. Reflex sympathetic activation, reported by Bokuda et al18 and resulting from a blockade of adrenergic receptors, is probably the main mechanism in which neuroleptics increase normetanephrine concentration in the urine, as also observed in our study.
As confirmed in our study in a large cohort, many drug groups affected the synthesis and metabolism of catecholamines, influencing the properly measured urinary excretion of metanephrines. Among all groups of the analyzed medications, α- and β-blockers, CCBs, loop diuretics, NMADs, neuroleptics, GCSs, and antidepressants affected the results of these measurements to a different degree, while many other, such as potassium‑sparing diuretics, ACEIs/ARBs, LT4, thyreostatics, BDZs, inhaled B‑receptor agonists, ipratropium, thiazide diuretics, metformin, LLDs, and PPIs had no significant effect on fractionated metanephrines in the 24‑hour urine collection.
Limitations
The study was based on retrospective data analysis. All variables used were objective clinical information, and the data were collected with a high degree of completeness; it is unlikely that the results would change significantly if the data were analyzed prospectively. The fractionated urinary metanephrines were collected only once, and the possible effects of physiological stress may not be completely excluded. However, it is not possible to perform such a study in healthy people by giving them unnecessary drugs. The results of our study can be helpful for physicians dealing with questionable clinical cases.
Conclusions
Based on the findings of the present study, it is recommended that in the patients with AI and the biochemical results suggesting endocrine activity of AI, the effect of medications on metanephrine excretion should be eliminated, especially if there is a discrepancy between the biochemical test results and the clinical manifestations.
- Bancos I, Prete A. Approach to the patient with adrenal incidentaloma. J Clin Endocrinol Metab. 2021; 106: 3331‑3353. | Crossref
- Corssmit EPM, Dekkers OM. Screening in adrenal tumors. Curr Opin Oncol. 2019; 31: 243‑246. | Crossref
- Cyrańska‑Chyrek E, Szczepanek‑Parulska E, Stajgis P, et al. Incidental finding of a mass in the adrenal bed following adrenalectomy due to pheochromocytoma. Pol Arch Intern Med. 2019; 129: 921‑923. | Crossref
- Kebebew E. Adrenal incidentaloma. N Engl J Med. 2021; 384: 1542‑1551. | Crossref
- Lee JM, Kim MK, Ko SH, et al. Clinical guidelines for the management of adrenal incidentaloma. Endocrinol Metab (Seoul). 2017; 32: 200‑218. | Crossref
ARTICLE INFORMATION