Use of individual antihypertensive drug classes and combination therapies during the COVID-19 pandemic in Poland: a cross-sectional, nationwide study in the years 2019–2021
Key words: antihypertensive drugs, COVID-19 pandemic, guidelines, hypertension, single-pill combination

 CC BY 4.0
CC BY 4.0
Use of individual antihypertensive drug classes and combination therapies during the COVID-19 pandemic in Poland: a cross-sectional, nationwide study in the years 2019–2021
Introduction: The 2018 European Society of Cardiology / European Society of Hypertension guidelines recommended the use of combination therapy, especially in the form of single‑pill combinations (SPCs), for treatment of hypertension.
Objectives: We assessed adherence to these recommendations after their publication and during the COVID‑19 pandemic in Poland.
Patients and methods: The frequencies of using individual antihypertensive drug classes and their combinations were analyzed for the years 2019, 2020, and 2021 in all patients who filled at least 1 prescription for an antihypertensive drug, using information from a database covering all prescriptions filled in Poland.
Results: In the years 2019, 2020, and 2021, a total of 10 328 341, 9 478 949, and 9 637 595 patients, respectively, fulfilled the inclusion criteria. There was a continuous decrease in the rate of patients meeting the criteria for coprescribing 2 or more antihypertensive drugs in the consecutive years (59.3%, 49%, 45.6%, respectively, in 2019, 2020, and 2021; P <0.001). In 2019, 2020, and 2021, a combination of renin‑angiotensin system blockers, calcium channel blockers and / or diuretics was respectively used by 41.7%, 40.9%, and 42% of the patients taking 2 antihypertensive drugs (P <0.001), and by 15.2%, 17.2%, and 18.5% of the patients taking 3 antihypertensive drugs (P <0.001). There was an increase in the use of β-blockers over the study period (62%, 62.8%, and 63.7%, respectively, in 2019, 2020, and 2021; P <0.001). Double SPCs were used by 28%, 28.7%, and 29.8% of the patients (P <0.001), and triple SPCs by 2.6%, 2.9%, and 3.4% of the patients (P <0.001), respectively, in 2019, 2020, and 2021.
Conclusions: During the COVID‑19 pandemic, a decrease in the frequency of combination treatments and an increase in the frequency of dual and triple SPC use were observed. Despite the slow increase in the frequency of prescribing the guideline‑recommended drug combinations, their use remains suboptimal.
What's new?
Hypertension guidelines recommend frequent use of combination therapy, especially in the form of a single pill. We obtained the frequencies of using individual antihypertensive drug classes and their combinations for the years 2019–2021 from a database covering all prescriptions filled in Poland. The results of our analysis showed a reduction in the use of combination treatments during the COVID‑19 pandemic. They also indicated a limited impact of the recommendations on the pattern of hypertension treatment over several years. This is especially reflected by excessive frequency of β-blocker use and failure to take advantage of single‑pill combinations.
Introduction
Hypertension remains a major risk factor for cardiovascular morbidity and mortality, not only due to its widespread prevalence in the population but also because it is insufficiently diagnosed and inadequately treated.1 The European Society of Cardiology / European Society of Hypertension (ESC/ESH) guidelines published in 2018 introduced a simple antihypertensive treatment strategy as one of the solutions to improve the management of hypertension. This strategy is based on the use of a combination of 2 antihypertensive drugs from the onset of therapy in most patients, and intensification of treatment by adding on antihypertensive drugs one by one, if necessary, to attain target blood pressure (BP) values. It was also recommended to use single‑pill combinations (SPCs) at each step of the therapy, in order to reduce the pill burden and support adherence.2 These recommendations were subsequently implemented in the 2019 Polish Society of Hypertension guidelines.3
Shortly after publication of the 2018 ESC/ESH guidelines, the world was confronted with another threat: the COVID‑19 pandemic. Restrictions on access to health care, social isolation, changes in lifestyle and work patterns are among the many factors that have affected the way antihypertensive therapy has been administered, as well as its effectiveness, during the pandemic.4-7
Analyses of large medical databases enable assessment of changes in drug prescription patterns, and evaluation of the structure of treatment for many diseases, including hypertension, which would have been impossible in classic clinical and epidemiologic cross‑sectional studies.8-11 A limitation of such analyses is often a lack of detailed clinical patient data. In 2019, an electronic database covering all filled prescriptions was established in Poland. Thus, analysis of this database makes it possible to assess the structure of therapy and its long‑term changes in subsequent years in the Polish population.
The aim of the present study was to assess variations in the structure of hypertension therapy in the years 2019–2021 in Poland considering the impact of the COVID‑19 pandemic. We focused on the use of the guideline‑recommended drug combinations, including renin‑angiotensin system (RAS) blockers, calcium channel blockers (CCBs), and diuretics, as well as on the rate of using combination treatments, either as free‑dose combinations or as SPCs.
Patients and methods
Data of all adult patients who filled at least 1 prescription from the Anatomical Therapeutic Chemical Classification System groups C02 (antihypertensives), C03 (diuretics), C07 (β-blocking agents), C08 (CCBs), C09 (agents acting on the RAS), and C10BX (lipid‑modifying agents in combination with other drugs) in each of the analyzed years (2019, 2020, and 2021) were extracted from the e‑Health Center on filled prescriptions for drugs. Both the drugs reimbursed by the National Health Fund and those requiring full payment by the patient were considered. The patients with a principal or comorbid diagnosis of I50 (heart failure) according to the International Statistical Classification of Diseases, 10th Revision were excluded from the analysis. This exclusion criterion was met by 906 853 patients in 2019, 832 710 patients in 2020, and 857 087 patients in 2021. The individuals who filled a prescription only for captopril (a drug used ad hoc for acute increases in BP) were also excluded from the analysis. This exclusion criterion was fulfilled by 89 961 patients in 2019, 78 375 patients in 2020, and 90 488 patients in 2021.
In order to analyze the rate of use and type of combination therapies, we evaluated coprescription of antihypertensive drugs. We calculated duration of the therapy with a given drug as the number of days for which a patient had enough pills in the purchased packages (assuming 1 pill per 1 day). Treatment overlap (coprescription) was considered to occur when a patient had a supply of 2 drugs allowing them to take 1 pill a day of each drug concurrently for at least 40 days.12 If a patient purchased another package, duration of the treatment was considered to increase accordingly. In the case of SPC use, coprescription of individual substances included in the SPC was automatically recognized (based on brand names of antihypertensive drugs).
To assess the number and type of antihypertensive drugs used as a combination therapy each year by particular patients, we analyzed the drugs taken that met the coprescribing critera described above. In the cases where a patient took different combinations during a single year, the one that was used the longest was selected.
Frequencies of using individual antihypertensive drug classes were analyzed for the years 2019, 2020, and 2021. The following drug classes were considered: β-blockers (BBs); RAS inhibitors: angiotensin‑converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs); CCBs: dihydropyridine CCBs (dhpCCBs) or nondihydropyridine CCBs (ndhpCCBs); diuretics: thiazide diuretics (TDs), thiazide‑like diuretics (TLDs), or loop diuretics (LDs); mineralocorticoid receptor antagonists (MRAs); and others (centrally‑acting drugs and α-blockers). Separate analyses of the structure of antihypertensive therapy in patients using 1, 2, 3, or 4 antihypertensive drugs were also carried out.
Statistical analysis
Data are expressed as absolute values and percentages. The frequency of using each type of antihypertensive therapy in the consecutive years was compared using the χ2 test. All calculations, including statistical calculations, were made using Microsoft Excel version 16 (Microsoft, Redmond, Washington, United States) and the free Social Science Statistics application (socscistatistics.com; copyright 2023 Jeremy Stangroom).
Results
Use of combination therapy
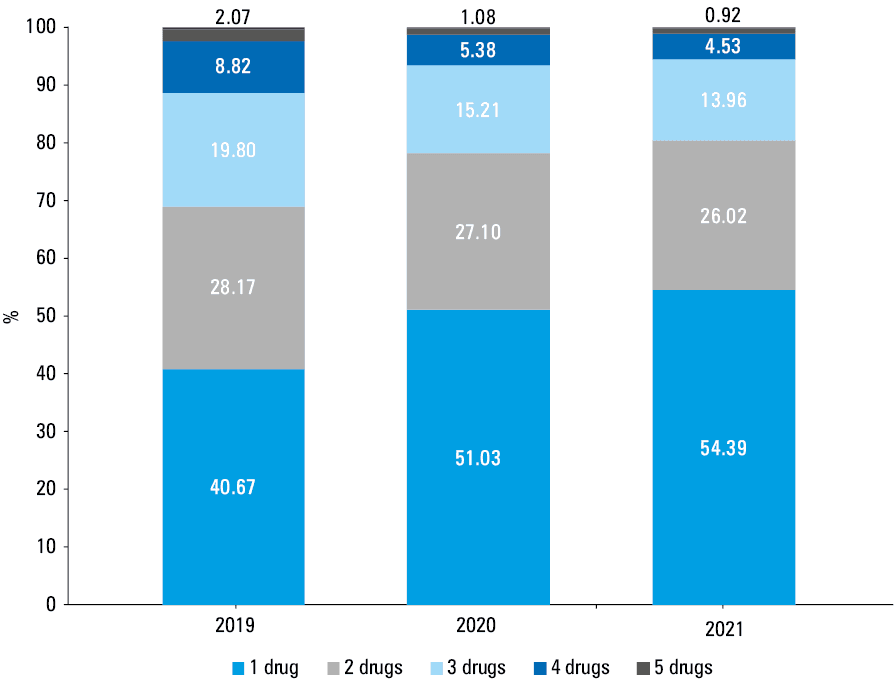
In the years 2019 (prepandemic period), 2020, and 2021 (pandemic), the inclusion criteria were fulfilled by 10 328 341, 9 478 949, and 9 637 595 patients, respectively. There was a decrease in the rate of patients who met the criteria for coprescription of 2, 3, 4, 5, and 6 or more antihypertensive drugs during the pandemic (2020–2021), as compared with the prepandemic period (2019) (Figure 1). The criteria for coprescribing of 2 or more and 3 or more antihypertensive drugs were met by 59.3%, 49%, 45.6% and 31.2%, 21.9%, 19.6% of the patients in the years 2019, 2022, and 2021, respectively (P <0.001; and P <0.001 for the difference between the consecutive years).
Use of individual antihypertensive drug classes
Among the main groups of antihypertensive drugs, the most often prescribed drug classes were RAS inhibitors (to 73.4%, 74.2%, and 72% of the patients in the years 2019, 2020, and 2021 respectively; P <0.001) and BBs (Supplementary material, Figure S1). Almost half of the patients used a diuretic (47.9%, 47.5%, and 47.4% in the years 2019, 2020, and 2021, respectively; P <0.001), and 1 in 3 patients used a CCB (35.7%, 36.3%, and 36.9% in the years 2019, 2020, and 2021, respectively; P <0.001). Within the class of RAS inhibitors, a decrease in the frequency of ACEI use was observed in 2021 (from 52.7% in 2020 to 46.8%, P <0.001), and an increase in the use of ARBs was noted (Supplementary material, Figure S1). An increase in the use of dhpCCBs was also observed. Within the class of diuretics, there were no major changes in the frequency of using particular drug types, except for a decrease in the use of TLDs (Figure 2). By converting the frequency of using each drug group to the total number of filled antihypertensive drug prescriptions, we found a comparable frequency of using each group—BBs were used the most often, followed by ACEIs, dhpCCBs, ARBs, TLDs, and others (Supplementary material, Table S1). The 5 most often used agents within each drug group are shown in Supplementary material, Figure S2.
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BB, β-blocker; dhpCCB, dihydropyridine calcium channel blocker; LD, loop diuretic; MRA, mineralocorticoid receptor antagonist; ndhpCCB, nondihydropyridine calcium channel blocker; TD, thiazide diuretic; TLD, thiazide‑like diuretic
Structure of therapy according to the number of antihypertensive drugs used
Among the classes of drugs taken in monotherapy, BBs were used the most often (Table 1). The second most common group were ACEIs, followed by ARBs and dhpCCBs (Table 1). During the pandemic, there was an increase in the prescription rate of BB, MRA, and LD monotherapy, and a decrease in the use of ACEIs and ndhpCCBs as single antihypertensive drugs.
Antihypertensive drug group | 2019 | 2020 | 2021 | P value |
Data are presented as percentages. | ||||
β-Blockers | 38.6 | 40.1 | 40.4 | <0.001 |
Angiotensin‑converting enzyme inhibitors | 24.3 | 22.2 | 21.3 | <0.001 |
Angiotensin II receptor blockers | 10.6 | 10.6 | 10.8 | <0.001 |
Dihydropyridine calcium channel blockers | 9.2 | 9.9 | 10 | <0.001 |
Thiazide‑like diuretics | 5.7 | 5.5 | 5.5 | <0.001 |
Loop diuretics | 2.2 | 4.9 | 5.2 | <0.001 |
Mineralocorticoid receptor antagonists | 1.9 | 2.2 | 2.4 | <0.001 |
Thiazide diuretics | 4.3 | 1.5 | 1.6 | <0.001 |
α-Blockers | 1.7 | 1.7 | 1.6 | <0.001 |
Centrally‑acting drugs | 0.7 | 0.7 | 0.7 | <0.001 |
Nondihydropyridine calcium channel blockers | 0.8 | 0.6 | 0.5 | <0.001 |
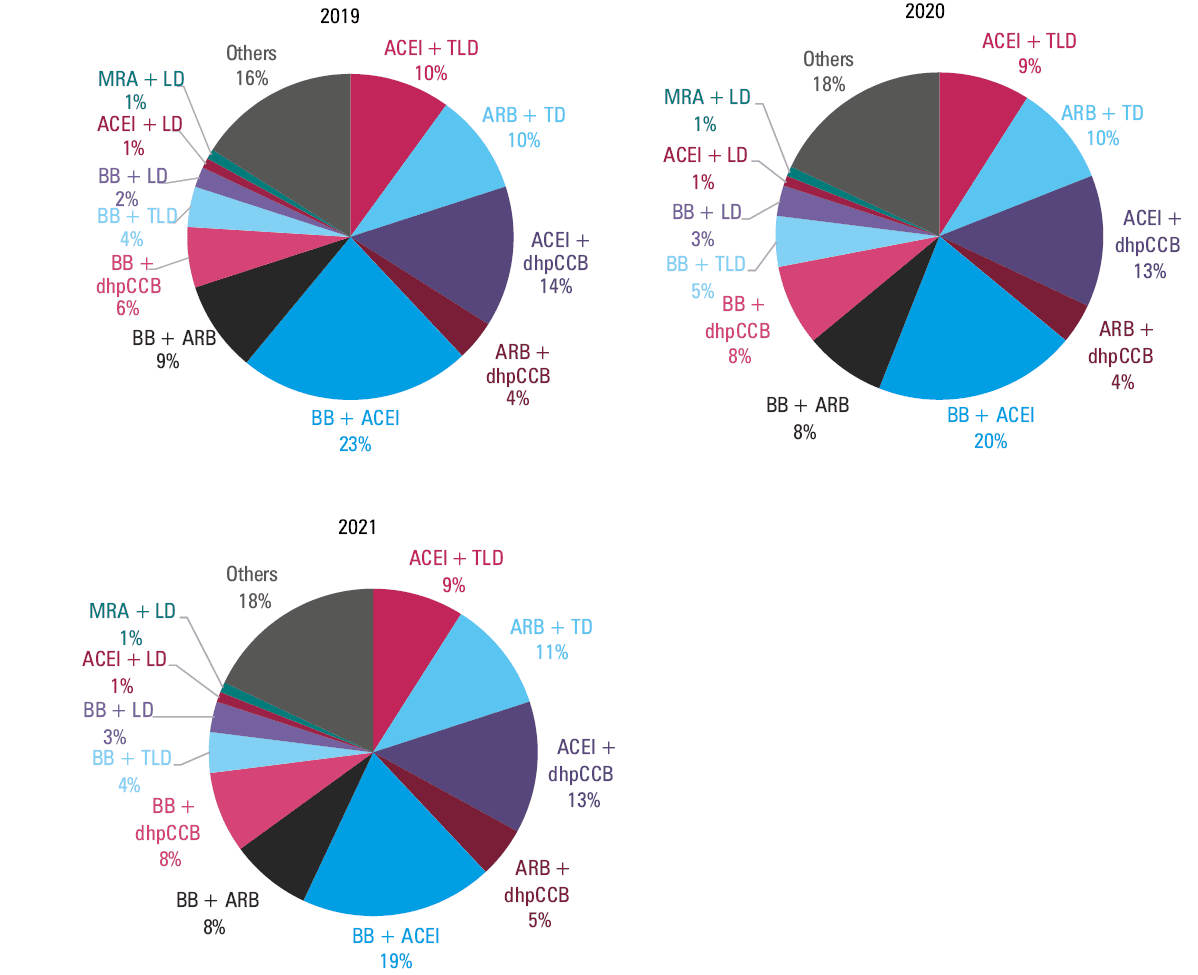
Among the patients taking 2 antihypertensive drugs (meeting the criteria of coprescription), the most common combination was a BB + an ACEI (Figure 2). The frequency of using this combination showed a downward trend during the pandemic. BBs in combination with other antihypertensive drugs were used by 48.6%, 46.9%, and 45.7% of the patients, respectively, in the years 2019, 2020, and 2021 (P <0.001). Combinations of an ACEI/ARB + a TD/TLD and an ACEI/ARB + a dhpCCB were used by 24.3%, 23.4%, and 23.6% (P <0.001) and 17.4%, 17.6%, and 18.4% (P <0.001) of the patients, respectively, in 2019, 2020, and 2021 (Figure 2). Together, the abovementioned combinations accounted for 41.7%, 40.9% and 42% of the 2‑drug combinations used in 2019, 2020, and 2021, respectively (P <0.001). Within those combinations, the most pronounced increase in the years 2020–2021 was observed for the ARB + dhpCCB combination. During the pandemic, there was a decrease in the frequency of ACEI use (51.9%, 46.8%, and 45.8% of the patients in 2019, 2020, and 2021, respectively; P <0.001) and an increase in the frequency of dhpCCB use (26.6%, 29.7%, 30.6% of the patients in 2019, 2020, and 2021, respectively; P <0.001) in 2‑drug combinations.
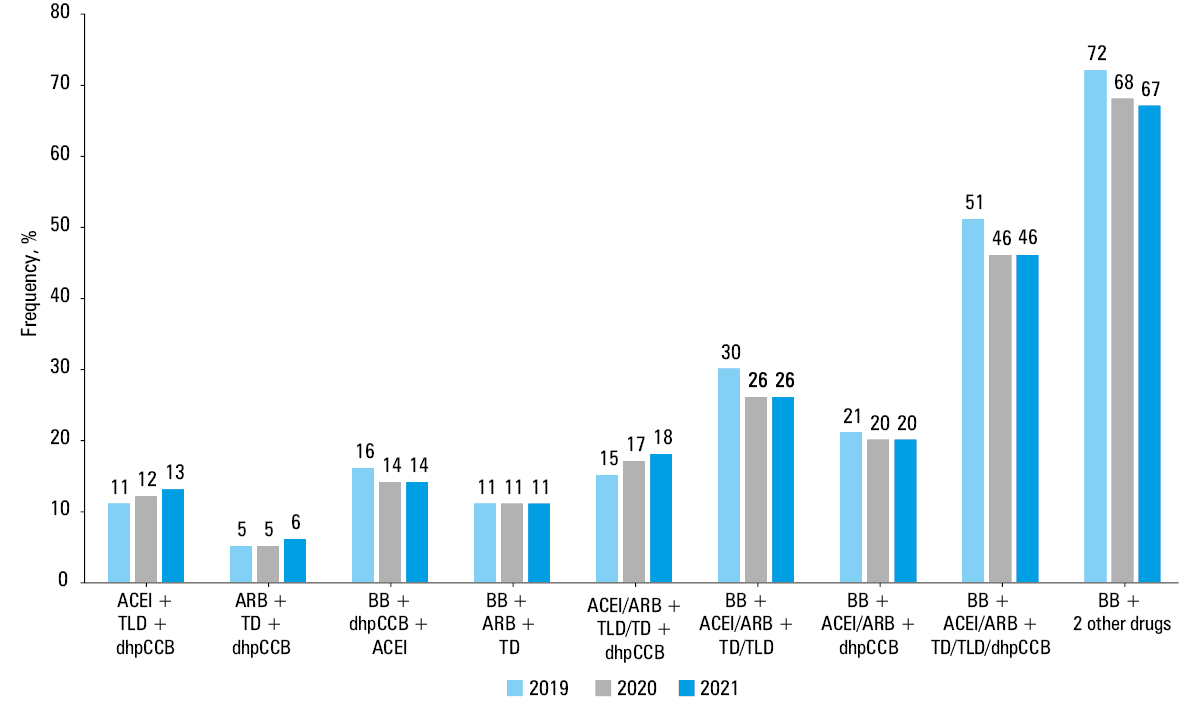
Among the patients taking 3 antihypertensive drugs (meeting the criteria of coprescription), the most common combination was that of a BB + an ACEI + a dhpCCB (Figure 3). The frequency of using this combination showed a downward trend during the pandemic. BBs were also used the most often in 3‑drug combinations (71.8%, 68.1%, 66.6% of the patients in 2019, 2020, and 2021, respectively), with a downward trend during the pandemic (P <0.001).
Abbreviations: see Figure 2
The recommended 3‑drug combination (ACEI/ARB + TD/TLD + dhpCCB) was used by 15.2%, 17.2%, and 18.5% of the patients, respectively, in the years 2019, 2020, and 2021, with an upward trend (P <0.001). This approach resulted in more frequent use of the ACEI + TLD + dhpCCB and ARB + TD + dhpCCB combinations.
Among the patients taking 4 antihypertensive drugs (meeting the criteria of coprescription), the most common combination was a BB + an ACEI + a TLD + a dhpCCB, used respectively by 27%, 27.2%, and 28.6% of the patients in 2019, 2020, and 2021 (P <0.001). An LD was used in every fourth combination of the 4‑drug regimens (23.6%, 26.4%, 26.6% of the patients in 2019, 2020, and 2021, respectively; P <0.001).
Use of single‑pill combinations
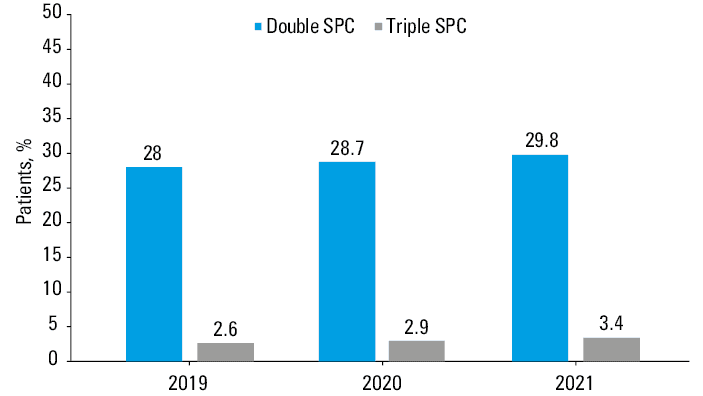
The last analysis focused on the prevalence of SPC use in the treatment of hypertension. We found a steady increase in the frequency of using double SPCs (Figure 4). Triple SPCs were used rather infrequently, although a substantial relative increase in the frequency of their use was observed (Figure 4). In total, any SPC (double or triple) was used by 32.3% of the patients in 2021.
Discussion
To our best knowledge, this is the first large population‑based study from a major European country assessing the impact of the 2018 ESC/ESH and Polish guidelines on the structure of hypertension therapy before and during the COVID‑19 pandemic, based on all prescriptions for antihypertensive drugs filled in the country in 3 years (2019–2021). Our results indicate 1) an increase in the use of guideline‑recommended combinations among the patients receiving 3 antihypertensive drugs, but not among those receiving 2 antihypertensive drugs; 2) a relatively high rate of BB use, and frequent use of combinations based on these agents, not corresponding to their place in the guidelines; 3) a significant decline in the use of combination therapies during the COVID‑19 pandemic; 4) a steady increase in the use of SPCs.
Use of guideline‑recommended antihypertensive drug combinations
The existing guidelines highlight the importance of using drug combinations with proven beneficial effects on cardiovascular risk in the treatment of hypertension. Emphasis is placed on the combinations including a RAS inhibitor and a CCB and / or a diuretic. It has been conclusively proven in randomized controlled trials and meta‑analyses that not only are such combinations effective in lowering BP and have a favorable tolerability profile, but also, most importantly, they reduce the risk of cardiovascular events.2,13,14 This justifies indicating them as preferable in the treatment of hypertension in the guidelines.2,3
In our analysis, among the patients receiving 2 antihypertensive agents, only 41%–42% used the recommended combinations. During the 3‑year study period, there was no increase in the rate of using the recommended combinations. Among the patients on 3 antihypertensive drugs, a gradual increase was observed each year; although the rate of the ACEI/ARB + CCB + TD/TLD combination use was only 15%–19%.
There are limited data on the use of the recommended combinations in contemporary cohorts. In an analysis of the NHANES study,15 the most common dual therapy was an ACEI/ARB + a diuretic. The recommended ACEI/ARB + CCB / diuretic combinations accounted for 60% of the 2‑drug combinations used in the years 2013–2016. The recommended triple combination (an ACEI/ARB + a CCB + a diuretic) was used by 26% of the patients receiving 3 antihypertensive drugs.
An interesting analysis from the United Kingdom (UK) evaluated changes in BP‑lowering treatment over 31 years. It showed a gradual increase in the use of ACEIs and CCBs, especially after 2004, when these groups were indicated as first‑line therapy in the UK guidelines.16
It is also worth noting that when certain preparations are unavailable or recalled, an increase in the frequency of use of other preparations from the same group is usually noted, rather than a switch to another group. This could be observed, for example, after withdrawal of valsartan preparations, which were replaced mainly with telmisartan in Poland, losartan in the United States, and candesartan in Canada and Germany.17
Use of β-blockers
The 2018 and 2019 guidelines2,3have excluded BBs from the primary treatment strategy for patients with hypertension without any cardiovascular diseases. It has been recommended to limit their prescription to situations in which there is a specific indication for the use of this group of drugs. Nevertheless, BBs remain the most widely used group of antihypertensive drugs in Poland. Moreover, a steady increase in their use has been observed. Only the frequency of using ACEIs and ARBs (assessed together) was higher than that of BBs.
Recently, 2 important reviews have questioned the validity of downgrading BBs in hypertension therapy.18,19 It has been argued that hypertension is characterized by activation of the sympathetic nervous system, which makes BBs an appropriate treatment from a pathophysiological viewpoint. In addition, BBs are a diverse group of drugs, in which no class effect is found. It is presumed that BBs with high β-blocking selectivity and / or vasodilating properties should be preferred because they lack disadvantages typical of other BBs. Moreover, it has been shown that nonatenolol BBs are effective in lowering BP when used as an add‑on to monotherapy or as a component of combination therapy.20 The recently published ESH guidelines shared this view, and pointed to a greater role of BBs in the treatment of hypertension.21
The available studies indicate differences between countries in both the frequency of BB use and the types of specific preparations prescribed. In a study from the United States (Florida), BBs were the second most common antihypertensive group in patients initiating hypertension therapy, with a decreasing frequency between 2013 and 2021.22 In the NHANES analysis, BBs were the third most common antihypertensive group in treated hypertensive patients, with a decreasing frequency of use (from 39.4% in 2005–2008 to 35.1% in 2013–2016).15 Moreover, in the same analysis, the authors observed a sharp decrease (by 53%) in the proportion of hypertensive patients taking BBs in monotherapy without compelling indications (from 12% in 2005–2008 to 6% in 2013–2016; corresponding to 24% and 13% of patients on monotherapy in each period, respectively). In a population‑based cohort study from the UK, BBs were the third most often prescribed antihypertensive drug group after ACEIs and CCBs, constituting 22.5% of all drug prescriptions (analysis per prescription).16 In our study, in the per prescription analysis, BBs represented 27.3%–27.5% of all drug prescriptions filled. A study by Rouette et al16 also showed that although BBs were no longer recommended as the first‑line antihypertensive treatment in the UK after 2010, there was no reduction in their use. Conversely, they were the most frequently prescribed drug group at treatment initiation (40% of patients starting therapy).16 Similar results were reported from Sweden, even during the COVID‑19 pandemic.23,24 Not in all countries are BBs so frequently prescribed.25-28 According to studies from Australia, Japan, and Saudi Arabia, only 27.6%, 25%, and 10.1% of patients, respectively, were treated with BBs.26-28 An analysis of 2‑drug regimens used at the initiation of hypertension therapy in 8 countries found wide variations in the use of BB‑based therapy, ranging from 0.7% in China to 32.3% in South Korea.9
Not only are BBs used due to their BP‑lowering and antiarrhythmic effects. They are also widely applied for the treatment of diseases coexisting with hypertension, including anxiety and migraines. A recent study from the UK has shown that incident prescription rate of BBs rose almost 2‑fold between 2003 and 2018.29
Use of combination therapies
In 2019, the prevalence of antihypertensive monotherapy use in Poland was comparable to that observed in 2013–2016 in the NHANES study analysis (40.7% vs 40.1%).15 However, it increased significantly to 54.4% in 2021, mainly due to a decrease in the percentage of patients meeting the criteria for coprescribing of 3, 4, 5, and 6 or more antihypertensive drugs in 2020 and 2021, during the COVID‑19 pandemic. Data from the UK concerning primary care patients showed that in 2018, 51% of the patients were prescribed 2 or more antihypertensive drugs.16 A study from Australia, which used the same definition of coprescription as the one adopted in our study, found that in 2018, 52.5% of the patients were treated with a single antihypertensive drug.27
Even though the European and Polish guidelines placed a strong emphasis on the use of combination treatment, the impact of these recommendations on clinical practice has remained relatively low in most European countries. Thus, no impact of the 2018 ESC/ESH guideline recommendation on the use of combination therapy (both free‑dose combinations and SPCs) was shown in a work by Savare et al.30 The study included residents of the Lombardy region (Italy) aged 40 years or older, in whom antihypertensive treatment was initiated in 2012, 2015, and 2018 (the last cohort should have been influenced by the 2018 guidelines). After 2 years of treatment, 58.9%, 58.9%, and 61% of the patients, respectively, were still receiving monotherapy. Similar results were reported from Germany, France, and Italy.9,31
Our study shows that the use of combination treatment (both free‑dose combinations and SPCs) for hypertension decreased in the years 2020 and 2021, as compared with 2019, indicating that the COVID‑19 pandemic has only exacerbated the already suboptimal use of combination therapy observed in earlier studies. The reduction in the frequency of combination therapy use observed in our study during the COVID‑19 pandemic may translate to other populations and indicate that, in general, more than half of individuals with hypertension worldwide are currently receiving monotherapy.
Slow but steady increase in the use of single‑pill combinations
The existing guidelines emphasize that SPCs should be used whenever possible. Thanks to simplification of the therapeutic regimen, their use is associated with increased adherence and persistence.13,32,33 Recently, Schmieder and al34 compared the effects of using 4 SPCs vs identical multiple pills on the rate of cardiovascular events, mortality, and adherence. The authors found that the use of SPCs was associated with a reduction in all‑cause mortality, as well as with reduced rates of coronary events, heart failure, and stroke. They also observed higher adherence rates at 1‑year follow‑up in the patients receiving SPCs.
Another important benefit of SPCs is their potential to reduce patient and reimbursement costs, as well as the costs of managing the consequences of poorly treated hypertension, thus improving the cost‑effectiveness of antihypertensive therapy, as suggested recently.35 In Poland, the factor limiting wider use of SPCs were regulations regarding their reimbursement—SPCs could be reimbursed only when used in accordance with the characteristics of the medicinal product (most often replacing the already used drugs with SPCs), which was not in line with guideline recommendations on their use (ie, treatment initiation and therapy intensification).36 Yet, our study shows a slow, steady increase in the use of SPCs. However, it should be noted that less than 30% of the patients used 2‑drug–based SPCs. Our findings are in accordance with the previously published rates. In Japan, SPCs were taken by less than 20% of patients on 2 antihypertensive drugs,37 and in Australia, any SPC was taken by 33.1% of patients prescribed with antihypertensive medications in 2018.27 Actually, 2 recent studies have shown a decrease in the use of SPCs with time. In an analysis of the prepandemic NHANES cycles (2009–2012, 2013–2016, and 2017–2020), a decrease in the use of SPCs by hypertensive patients taking at least 2 different classes of antihypertensives was observed (35.8% in 2009–2012, 32.4% in 2013–2016, and 27.8% in 2017–2020).38 Of interest, among the individuals treated with SPCs, there were more patients with controlled hypertension than among those not taking SPCs. In our study, we assessed the frequency of SPC use in the entire population of patients taking antihypertensive drugs. If we had limited our estimates to the patients taking 2 or more drugs, the Polish population would have been characterized by a higher use of SPCs than the United States population in the prepandemic period.
Limitations
The analyzed database did not include demographic data, such as age or sex, which have been shown to influence drug prescription patterns. However, conducting more detailed analyses would have made it difficult to interpret the results regarding the main objectives of the study. In addition, no detailed clinical data, such as BP values, duration of hypertension, and comorbidities, were available. We were also unable to assess regional differences (eg, between provinces) or the differences between prescriptions issued by primary care physicians and specialists. This is due to the fact that at the current stage of electronic system implementation in Poland, these data would have been incomplete, which could have led to biased conclusions. Thus, for example, it could not be concluded whether maintaining patients on monotherapy was adequate or not. On the other hand, in comparison with other studies, we analyzed the entire population of a single large country, regardless of whether the drug was prescribed by a family doctor or a specialist, during a reimbursed or private visit, and whether the drug was reimbursed or full‑price. In addition, we assessed the use of drugs in terms of individual patients rather than in terms of the number of drug packages filled. Just before the COVID‑19 pandemic, a mandatory electronic prescription system was introduced in Poland, which greatly facilitated access to treatment during the pandemic (especially follow‑up). Therefore, the results of our study may not be comparable with those from the countries where conventional prescriptions were used during the pandemic.
The effectiveness of hypertension therapy is affected by several factors, among which the importance of comorbidities, such as depression or anxiety disorders, as well as side effects of drugs are emphasized.39,40 It can be postulated that these factors may have played a greater role during the COVID‑19 pandemic.
Conclusions
Over the last decade, the percentage of patients with well‑controlled hypertension has not increased substantially, and has even decreased in some countries. The COVID‑19 pandemic has further negatively affected BP control.6,41,42 We observed a reduction in the use of combination treatments in Poland in the years 2020–2021, as compared with 2019, which implies that the negative trends regarding BP control may have been further exacerbated during the pandemic. The results of our analysis also indicate a limited impact of the guideline recommendations on the structure of antihypertensive treatment over several years. This is especially true with respect to the use of BBs and SPCs.
- Carey RM, Moran AE, Whelton PK. Treatment of hypertension: a review. JAMA. 2022; 328: 1849‑1861. | Crossref
- Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018; 36: 1953‑2041.
- Tykarski A, Filipiak KJ, Januszewicz A, et al. 2019 Guidelines for the management of hypertension — Part 1‑7. Arterial Hypertension. 2019; 23: 41‑87. | Crossref
- Weber T, Amar J, de Backer T, et al. COVID‑19 associated reduction in hypertension‑related diagnostic and therapeutic procedures in Excellence Centers of the European Society of Hypertension. Blood Press. 2022; 31: 71‑79. | Crossref
- Januszewicz A, Wojciechowska W, Prejbisz A, et al. Impact of the COVID‑19 pandemic on blood pressure control and cardiovascular risk profile in patients with hypertension. Pol Arch Intern Med. 2021; 131: 16129. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION