A novel microRNA differentially expressed in patients with persistent and paroxysmal atrial fibrillation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A novel microRNA differentially expressed in patients with persistent and paroxysmal atrial fibrillation
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia in the general population. The estimated prevalence of this arrhythmia in adults ranges from 2% to 4%.1 AF is one of the leading causes of stroke, heart failure, other thromboembolic complications, and sudden death. On the basis of the duration of an arrhythmia episode, AF is classified as first‑diagnosed, paroxysmal, persistent, long‑standing persistent, or permanent.2 In recent years, there has been a growing body of evidence that microRNAs (miRNAs) play an important role in AF development and progression.3 Advances in next‑generation sequencing technologies made it possible to identify and evaluate putative novel miRNAs associated with this arrhythmia. Hence, the main goal of this study was to identify novel circulating serum miRNAs that can differentiate between paroxysmal and persistent AF, and may serve as potential diagnostic biomarkers.
Patients and methods
Patients
A total of 94 patients undergoing first‑time ablation due to AF were included. The study population was divided into study (n = 19) and validation (n = 75) groups. Persistent and paroxysmal AF were determined according to the 2016 European Society of Cardiology recommendations.2 Characteristics of the participants are summarized in Supplementary material, Table S1. The study was conducted in accordance with the principles of the Declaration of Helsinki, and approved by the Bioethics Committee of the Military Institute of Medicine (12/WIM/2015). Written informed consent was obtained from all participants.
Blood sample collection
Venous whole blood samples were collected and centrifuged after clotting at 1500 × g for 10 minutes at room temperature. The resulting serum samples were stored at −80 °C.
Small RNA sequencing
High‑throughput small RNA sequencing experiments and data analysis were performed using Qiagen Genomic Services (Hilden, Germany), as described previously.4 To identify putative novel miRNAs, the miRPara software was used.5
MicroRNA isolation, reverse transcription, and droplet digital polymerase chain reaction
Total RNA, including miRNA, was extracted from 200 μl of the serum samples using the miRNeasy Serum / Plasma Advanced Kit (Qiagen) in accordance with the manufacturer’s instructions. Complementary DNA was synthesized from purified miRNA using the miRCURY LNA RT Kit (Qiagen) according to the manufacturer’s protocol. Quantification of miRNA levels in serum samples from the validation group was performed using the QX200 Droplet Digital polymerase chain reaction (PCR) system (Bio‑Rad, Hercules, California, United States), as previously described.4 Data were expressed as normalized units, according to the level of miR‑16‑5p, an endogenous reference widely used for circulating miRNA studies.
Bioinformatic analysis
A putative miRNA sequence identified as a factor differentiating between patients with persistent and paroxysmal AF was used for prediction of potential gene targets by means of the Homo sapiens reference transcriptome sourced from the Ensembl database (https://www.ensembl.org). An initial prediction was run using the miRanda 3.3a algorithm6 with the following settings: minimum score greater than or equal to 140, free energy lower than or equal to –20 kcal/mol, and gap opening penalty lower than or equal to –9 for X and –4 for Y. As a result, 5094 potential targets were obtained, and after duplicate removal (due to multiple transcripts per gene) and filtering out the sequences without a gene entry, 1444 targets remained. Due to the high number of potential targets, which is unlikely to reflect the real behavior of miRNA, a second prediction using the psRNAtarget web server7 was run, which resulted in the generation of 143 potential target genes. The final list of genes was created by identifying the overlapping elements between the miRanda- and psRNAtarget‑generated datasets, resulting in 23 possible targets.
Statistical analysis
Statistical analysis was performed using the R statistical software, version 4.3.1 (The R Foundation for Statistical Computing, Vienna, Austria; https://www.R‑project.org). Normality of variable distribution was first evaluated with the Shapiro–Wilk test, and group comparisons were made using the t test for the normally distributed data or the Mann–Whitney test for the variables deviating from the normal distribution. Comparisons of categorical variables were made using the Fisher exact test. In all cases, a P value below 0.05 was set as the cutoff for statistical significance. The receiver operating characteristic (ROC) curve was constructed, and the area under the curve (AUC) with 95% CI was calculated using the R ROCit package. The optimal cutoff point was determined as the point geometrically closest to the (100%, 100%) point on the ROC plot, using the following formula: [(1–Specificity)2 + (1–Sensitivity)2]1/2.
Results and discussion
High‑throughput small RNA sequencing was performed to screen circulating serum miRNA profiles in the study group. Sequencing data revealed 8 putative novel miRNAs differentiating patients with persistent (n = 8) from those with paroxysmal AF (n = 11) (Supplementary material, Table S2). The miRNA with the highest expression level, put‑miR‑25, was selected for further analysis. Put‑miR‑25 was significantly downregulated in the serum of patients with persistent AF, as compared with those with paroxysmal AF (fold change = 0.566; P = 0.005) in the study group. Validation was carried out by droplet digital PCR (ddPCR) using serum samples from the independent validation group. Consistent with the sequencing results, the patients with persistent AF (n = 24) showed a significantly lower median level of put‑miR‑25 than those with paroxysmal AF (n = 51) (Figure 1A). To estimate the ability of put‑miR‑25 to distinguish between the patients with persistent and paroxysmal AF, a ROC curve analysis was performed (Figure 1B). The AUC for put‑miR‑25 was 72.8% (95% CI, 61.3%–84.3%). The ROC curve yielded an optimal put‑miR‑25 expression cutoff value of 375, with sensitivity of 54.9% and specificity of 83.3%.
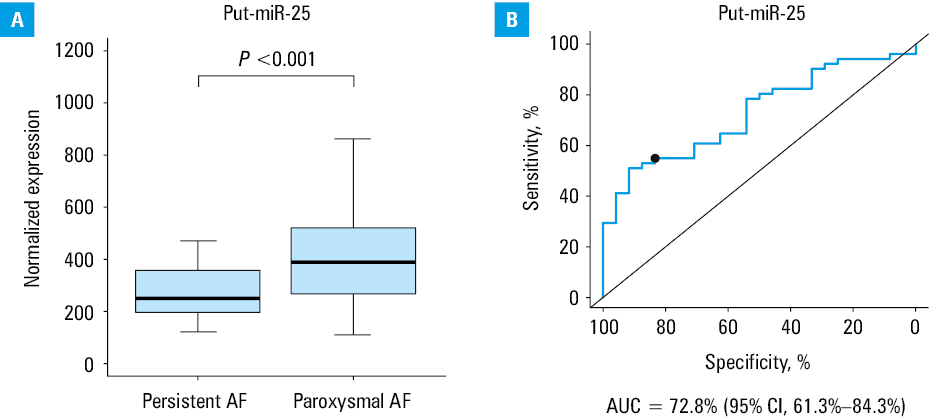
Abbreviations: AF, atrial fibrillation; AUC, area under the curve
To find potential targets of put‑miR‑25, we employed target prediction algorithms, namely, miRanda 3.3a and the psRNAtarget web server. Put‑miR‑25 was predicted to target 23 genes (Supplementary material, Table S3). Of particular note are the fms‑related receptor tyrosine kinase 1 gene (FLT1) and the inositol 1,4,5‑trisphosphate receptor type 1 gene (ITPR1), which have previously been associated with AF. Expression of both these genes was shown to be elevated in AF, which correlates with decreased levels of put‑miR‑25 found in our study. FLT1 was significantly upregulated in atrial tissues of patients with persistent AF in comparison with individuals without AF.8 This upregulation may lead to increased endothelial cell proliferation during atrial remodeling in AF. An increase in the expression of ITPR1 in atrial tissues of patients with chronic AF may be important in modulating intracellular Ca2+ homeostasis and in the initiation or perpetuation of AF.9 Based on the scores yielded by both by miRanda 3.3a and psRNAtarget, another potential target candidate for put‑miR‑25 was the cyclin L1 gene (CCNL1). Although currently there is no evidence linking this gene to AF, it was found to play a role in cardiomyocyte proliferation after myocardial infarction,10 and one of its variants was found in a genome‑wide association study to be related to coronary artery disease.11
Study limitations
This was a pilot, single‑center study, and the sample size was limited. Further evaluation of the clinical utility of put‑miR‑25 using multicenter cohorts would be necessary. In addition, interactions with target genes should be confirmed experimentally in further steps.
Conclusions
Sequencing data from the study group revealed a putative novel miRNA sequence, put‑miR‑25, to be significantly downregulated in serum of patients with persistent AF, as compared with individuals with paroxysmal AF. Validation was carried out with ddPCR using serum samples from the independent validation group, and the results matched those obtained in the sequencing data analysis. Target gene prediction indicated that put‑miR‑25 may be involved in metabolic processes relevant to pathogenesis of cardiovascular diseases.
- Staerk L, Wang B, Preis SR, et al. Lifetime risk of atrial fibrillation according to optimal, borderline, or elevated levels of risk factors: cohort study based on longitudinal data from the Framingham Heart Study. BMJ. 2018; 361: k1453. | Crossref
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016; 18: 1609‑1678. | Crossref
- Komal S, Yin JJ, Wang SH, et al. MicroRNAs: emerging biomarkers for atrial fibrillation. J Cardiol. 2019; 74: 475‑482. | Crossref
- Kiliszek M, Maciak K, Maciejak A, et al. Serum microRNA in patients undergoing atrial fibrillation ablation. Sci Rep. 2020; 10: 4424. | Crossref
- Wu Y, Wei B, Liu H, et al. MiRPara: a SVM‑based software tool for prediction of most probable microRNA coding regions in genome scale sequences. BMC Bioinformatics. 2011; 12: 107. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION