Although a vast majority of patients with congenital heart disease (CHD) die from cardiovascular causes, between 6% and 13% of them die from cancer.1,2 Given the increased risk of complications during noncardiac surgery, these patients may occasionally be denied definitive cancer therapy.
A 44‑year‑old woman with Eisenmenger syndrome (uncorrected complete atrioventricular canal defect) was referred to our center by her CHD specialist for re‑evaluation of breast cancer in April 2022. The cancer diagnosis was established in December 2021; however, the patient was denied definite treatment at the regional center due to an unacceptable cardiovascular risk.
She had a pacemaker (transvenous dual‑chamber system) implanted due to sick sinus syndrome, and was on long‑term anticoagulation with a vitamin K antagonist (VKA). She was also treated with macitentan and sildenafil for pulmonary hypertension. On examination, she had clubbing, central cyanosis, and a loud ejection systolic murmur over the precordium, with a split‑second heart sound. She was in a stable clinical condition, with a World Health Organization functional class of II/III.
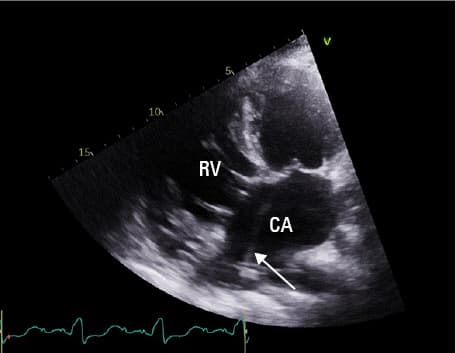
The patient had normal blood pressure of 106/74 mm Hg, pulse of 80 bpm, and oxygen saturation of 84% on room air. Evaluation of hematology parameters showed secondary erythrocytosis with a hemoglobin level of 18.1 g/dl (reference range [RR], 12–16 g/dl) and a hematocrit fraction of 54% (RR, 36%–48%). In addition, the N‑terminal pro–B‑type natriuretic peptide level was significantly elevated (3533 pg/ml; RR <125 pg/ml). Transthoracic echocardiography (Figure 1) revealed a significant atrioventricular defect with a bidirectional shunt. The right ventricle (RV) was hypertrophied and enlarged, with good systolic function (tricuspid annular plane systolic excursion of 21 mm, RV lateral tricuspid annulus peak systolic velocity of 9 cm/s). Electrocardiography showed sinus rhythm and right axis deviation with RV hypertrophy. The patient achieved 356 m in the 6‑minute walk test.
Multifocal left breast cancer (cT2mN0M0, luminal B subtype, HER‑2 negative) was confirmed. A multidisciplinary team (involving a CHD and pulmonary hypertension specialist, a senior cardiac anesthetist, and an oncology surgeon) qualified the patient for surgery. VKA was interrupted 48 hours before the procedure, and a therapeutic dose (1 mg/kg twice daily) of low‑molecular‑weight heparin (LMWH) was administered. The patient was operated on under local (LA) and general anesthesia (GA). The combined mode was chosen to decrease the risk of hemodynamic instability caused by GA, and to provide good operating conditions for the surgeon, which are impossible to obtain under LA alone. Total intravenous anesthesia was chosen as more stable and more controllable than the endotracheal technique. Continuous infusion of propofol and remifentanil was administered. With respect to LA, regional blocks within the chest wall were performed. During the entire operation, direct monitoring of the mean arterial pressure (MAP) was carried out, and MAP values of 68 to 70 mm Hg (the average for the patient) were maintained by continuous infusion of norepinephrine. A simple removal of the left breast and excision of the left axillary sentinel node were performed. After the surgery, the patient was transferred to the intensive care unit (ICU) for monitoring. Anticoagulation with VKA was reimplemented in the ICU following LMWH bridging therapy. The postoperative course was uncomplicated. The patient was discharged home on the 7th day after the operation.
Patients with Eisenmenger syndrome should not be denied definitive cancer treatment. Every case should be discussed in a multidisciplinary team, and a detailed management plan should be made a priori. Local / regional anesthesia alternatives should be pursued, if possible, as the mortality in patients receiving LA is lower than in those receiving GA (5% vs 18%).3,4
- Diller GP, Kempny A, Alonso‑Gonzalez R, et al. Survival prospects and circumstances of death in contemporary adult congenital heart disease patients under follow‑up at a large tertiary centre. Circulation. 2015; 132: 2118‑2125. | Crossref
- Yu C, Moore BM, Kotchetkova I, et al. Causes of death in a contemporary adult congenital heart disease cohort. Heart. 2018; 104: 1678‑1682. | Crossref
- Price LC, Martinez G, Brame A, et al. Perioperative management of patients with pulmonary hypertension undergoing non‑cardiothoracic, non‑obstetric surgery: a systematic review and expert consensus statement. Br J Anaesth. 2021; 126: 774‑790.
- Martin JT, Tautz TJ, Antognini JF. Safety of regional anesthesia in Eisenmenger’s syndrome. Reg Anesth Pain Med. 2002; 27: 509‑513. | Crossref
ARTICLE INFORMATION