Role of glucagon-like peptide-1 receptor agonists in the treatment of obesity, cardiovascular disease, and cerebrovascular disease
Key words: cardiovascular diseases, glucagon-like peptide-1 receptor agonists, obesity



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Role of glucagon-like peptide-1 receptor agonists in the treatment of obesity, cardiovascular disease, and cerebrovascular disease
Worldwide prevalence of obesity is increasing dramatically, imposing a significant economic burden on our society. Treatment of obesity is challenging, potentially due to different disease phenotypes. Taking into consideration “obesities” rather than “obesity,” and thus aiming to understand different pathophysiologic mechanisms of individual phenotypes, might help identify more tailored treatment strategies. Glucagon‑like peptide‑1 receptor agonists (GLP‑1RAs), for example, dulaglutide and semaglutide, are routinely prescribed for the treatment of type 2 diabetes mellitus (T2DM) in patients with obesity or those at a high cardiovascular (CV) risk. Indeed, despite having been developed for T2DM, GLP‑1RAs are being increasingly often recognized as antiobesity medications due to their weight loss effects. Furthermore, recent evidence has shown that the extent of CV prevention offered by these drugs goes beyond that associated with their weight loss and pleiotropic effects. For instance, they exert anti‑inflammatory effects on vessels, enhance atherosclerotic plaque stability, reduce local advanced glycation end product receptor expression, lower monocyte‑macrophage adhesion, and antagonize the effect of angiotensin II. In the heart, GLP‑1RAs ameliorate cardiomyocyte survival and myocardial contractility, reduce cardiac hypertrophy, and are one of few drugs that can reduce epicardial fat thickness. In this review, we summarize recent evidence concerning the effects of GLP‑1RAs on obesity / dysmetabolism and on cardio- / cerebrovascular health. We further highlight the possible role of GLP‑1RAs in the treatment of obesity‑related CV diseases by describing the principal molecular mechanisms reported in the current literature.
Introduction
Despite the efforts of health care systems worldwide to promote healthy lifestyle as a prevention of cardiovascular (CV) and cerebrovascular (CBV) diseases, the global prevalence of obesity has increased over the last few decades,1 and is forecasted to rise even more in the coming years.2 As a result, obesity represents an important social and economic burden, especially due to obesity‑related diseases.3 Therefore, deep understanding of its pathophysiology and identification of the most appropriate treatment are crucial to improve patients’ quality of life and health care sustainability.
Inflammation has emerged as the core of obesity‑related diseases.4 Considering obesity as a condition related to persistent low‑grade inflammation of the whole body can explain the increased predisposition of individuals with obesity to development of various CV diseases (CVDs), such as hypertension,5 left ventricular hypertrophy,6 heart failure,7 arrhythmias,8 atherosclerotic plaque formation,9 epicardial fat deposits,10 and myocardial infarction.11 Intertwined with inflammation, other mechanisms linking metabolic alterations with CV conditions are insulin resistance12 and disturbed adipokine balance.13 In obesity, proinflammatory immune cells infiltrate the dysfunctional adipose tissue and promote the release of proinflammatory adipokines (such as leptin), while reducing the release of anti‑inflammatory ones (such as adiponectin).14
The quest for novel treatment strategies to reduce the social and health burden of obesity is continuing faster than ever. A recent therapeutic option is represented by glucagon‑like peptide‑1 receptor agonists (GLP‑1RAs), also known as GLP‑1 agonists or incretin mimetics. These molecules were initially developed for the treatment of type 2 diabetes mellitus (T2DM). Apart from lowering glucose levels, GLP‑1RAs also lead to significant weight loss; therefore, they are currently the gold standard in the treatment of overweight patients with T2DM. Of interest, these drugs have shown beneficial effects concerning CVD prevention in T2DM in recent clinical trials (Table 1). In the 2023 European Society of Cardiology (ESC) guidelines for the management of CVDs in patients with diabetes,15 GLP‑1RAs are indicated as the first‑choice treatment for T2DM patients at a high / very high CV risk or those with proven atherosclerotic CVD.
Trial | Primary end points | Drug regimen | Sample size | Follow‑up | Primary end point occurrence |
Abbreviations: CV, cardiovascular; ELIXA, Evaluation of Lixisenatide in Acute Coronary Syndrome; EXSCEL, Exenatide Study of Cardiovascular Event Lowering; HR, hazard ratio; LEADER, the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results; MI, myocardial infarction; PIONEER‑6, Peptide Innovation for Early Diabetes Treatment; qd, once a day; qwk, once a week; REWIND, Researching Cardiovascular Events With a Weekly Incretin in Diabetes; SC, subcutaneous; SELECT, Semaglutide Effects on Heart Disease and Stroke in Patients with Overweight or Obesity; UA, unstable angina | |||||
ELIXA, 201571 | MI, stroke, CV death, or hospitalization for UA | Lixisenatide up to 20 µg SC qd | 6068 | 1.1 y | Lixisenatide, 13.4% vs controls, 13.2% (HR, 1.02; 95% CI, 0.89–1.17; P <0.001 for noninferiority; P = 0.81 for superiority) |
LEADER, 201686 | Nonfatal MI or stroke, CV death | Liraglutide 1.8 mg SC qd | 9340 | 3.8 y | Liraglutide, 13% vs controls, 14.9% (HR, 0.87; 95% CI, 0.78–0.97; P <0.001 for noninferiority; P = 0.01 for superiority) |
SUSTAIN‑6, 201687 | Nonfatal MI or stroke, CV death | Semaglutide 0.5 or 1 mg SC qwk | 3297 | 2.1 y | Semaglutide, 6.6% vs controls, 8.9% (HR, 0.74; 95% CI, 0.58–0.95; P <0.001 for noninferiority) |
EXSCEL, 201774 | Nonfatal MI or stroke, CV death | Exenatide 2 mg SC qwk | 14 752 | 3.2 y | Exenatide, 11.4% vs controls, 12.2% (HR, 0.91; 95% CI, 0.83–1; P <0.001 for noninferiority; P = 0.06 for superiority) |
Harmony Outcomes, 201872 | MI, stroke, or CV death | Albiglutide 30 mg SC qwk for 5 weeks, then possible dose increase to 50 mg qwk | 9463 | 1.6 y | Albiglutide, 7% vs controls, 9% (HR, 0.78; 95% CI, 0.68–0.9; P <0.0001 for noninferiority; P = 0.0006 for superiority) |
PIONEER‑6, 201976 | Nonfatal MI or stroke, CV death | Semaglutide up to 14 mg qd orally | 3183 | 1.3 y | Semaglutide, 3.8% vs controls, 4.8% (HR, 0.79; 95% CI, 0.57–1.11; P <0.001 for noninferiority) |
REWIND, 201975 | Nonfatal MI or stroke, CV death | Dulaglutide 1.5 mg SC qwk | 9901 | 5.4 y | Dulaglutide, 12% vs controls, 13.4% (HR, 0.88; 95% CI, 0.79–0.99; P = 0.026) |
AMPLITUDE‑O, 202173 | Nonfatal MI or stroke, CV or all‑cause death | Efpeglenatide 4 or 6 mg SC qwk | 4076 | 1.8 y | Efpeglenatide, 7% vs controls, 9.2% (HR, 0.73; 95% CI, 0.58–0.92; P <0.001 for noninferiority; P = 0.007 for superiority) |
SELECT, 202385 | Nonfatal MI or stroke, CV death | Semaglutide 2.4 mg SC qwk | 17 604 | 3.3 y | Semaglutide, 6.5% vs controls, 8% (HR, 0.8; 95% CI, 0.72–0.90; P <0.001) |
In this review, we summarize recent evidence concerning obesity and dysmetabolism, and their implications on CV health. We highlight the role of GLP‑1RAs as a treatment for obesity and obesity‑related CVDs by describing the principal molecular mechanisms known from current literature.
Different phenotypes of obesity
The most common clinical method for assessing obesity is the use of body mass index (BMI), which is calculated by dividing an individual’s weight (in kilograms) by the square of their height (in meters). Obesity is still defined as BMI equal to or above 30 kg/m2.16 However, this method has several limitations. For instance, BMI does not account for the difference between muscle and fat mass, which means that very fit athletes might be inaccurately considered overweight or even obese. Conversely, cachectic patients might have normal or low BMI but show clinically relevant metabolic alterations and obesity‑related diseases. Such a condition is known as sarcopenic obesity.17 Other anthropometric measurements have been shown to increase the diagnostic value of BMI in obesity. One of such measurements is waist circumference18; probably due to the fact that the greatest amount of visceral fat is found in the abdomen. Increased and dysfunctional visceral fat has emerged as the hallmark of obesity and its related to dysmetabolic conditions. Indeed, obesity should be considered a complex metabolic disease rather than a mere phenotypic expression of fat mass. On this basis, assessment of body fat distribution, together with appropriate depiction of the metabolic profile (including glucose and lipids), allow for distinction of 4 different phenotypes: 1) metabolically unhealthy normal weight, 2) metabolically healthy overweight / obesity, 3) metabolically unhealthy overweight / obesity, and 4) sarcopenic obesity.4 Understanding the different pathophysiologic mechanisms of obesity phenotypes can be useful to improve the prediction of their impact on the CV system.
Impact of obesity on cardiovascular diseases
Inflammation is considered a central process in development of CVDs in obesity, and insulin has been identified as one of the main factors stimulating adipose tissue and systemic inflammation in this condition.4,19,20 Indeed, insulin has a strong impact on the lipid profile—it stimulates overmetabolization of free fatty acids or triglycerides in the adipose tissue, which results in production of a high number of fatty acid metabolism intermediates. These molecules may in turn trigger intracellular pathways, such as c‑Jun N‑terminal kinase, IκB kinase, and protein kinase C, leading to insulin receptor phosphorylation and signaling inhibition.13 On the other hand, hypertrophic adipocytes and macrophages in the adipose tissue of obese individuals tend to produce and release tumor necrosis factor (TNF)-α, which causes serine phosphorylation and tyrosine dephosphorylation of insulin receptor substrates, leading to their inactivation and degradation. Furthermore, concomitant presence of hyperglycemia21 and inflammation22 creates a detrimental loop that leads to proatherosclerotic conditions and cardiovascular dysfunction. Atherosclerosis is accelerated by hyperinsulinemia, dyslipidemia, and hyperglycemia, which are known to induce endothelial oxidative stress via several pathways, including advanced glycation end product (AGE) formation, protein kinase C and polyol / hexosamine pathway activation, and endoplasmic reticulum and mitochondrial dysfunction.23 Moreover, reactive oxygen species (ROS) are at the center of both vascular smooth‑muscle cell proliferation and apoptosis, which are mechanisms involved in plaque instability and its potential rupture.
Of note, recent studies have shown that patients with very high BMI, that is, those with morbid obesity, demonstrate lower rates of CV outcomes, including stroke24 and myocardial infarction,25 in comparison with normal‑weight or underweight individuals. Such an unexpected finding is known as the obesity paradox, and should be interpreted with caution.26 Indeed, most of these studies did not differentiate between metabolically healthy and unhealthy participants, and showed that markers of fat distribution, such as waist‑to‑hip ratio, seem to have better prognostic ability than BMI alone.27,28 Even though no universal definition of metabolically healthy obesity is available at the moment, such a term would describe individuals with high BMI and a healthy metabolic profile, that is, preserved insulin sensitivity, a favorable lipid profile, and low plasma levels of proinflammatory cytokines (typically young and physically active individuals with low percentage of visceral or ectopic fat).29 On the opposite end of the spectrum, the unhealthy obesity phenotype is characterized by insulin resistance and increased prevalence of CV risk factors other than high body weight and elevated percentage of visceral fat.29 Focusing on the incidence of CVDs and their outcomes in different phenotypes of obesity would still highlight that metabolically unhealthy obesity is related to more detrimental effects rather than benefits.
Treating obesity with glucagon‑like peptide‑1 receptor agonists
GLP‑1 is a 30‑amino acid‑long peptide that is cleaved from proglucagon. It is synthesized and secreted from intestinal enterocytes known as L cells.30 Together with gastric inhibitory peptide (GIP), GLP‑1 belongs to the group of incretin hormones, which perform several metabolic functions. Pancreatic β cells express the GLP‑1 receptor and respond to stimulation by increasing intracellular calcium level, eventually leading to greater exocytosis of insulin‑containing granules.31 GLP‑1 also improves insulin resistance of adipocytes by upregulating expression of insulin receptor β, insulin receptor substrate 1, and glucose transporter type 4.32 In muscles, GLP‑1 activates sirtuin 1 via the protein kinase A / cyclic adenosine monophosphate pathway, resulting in higher glucose transporter type 4 activity.33 Furthermore, GLP‑1 reduces gastric emptying by blunting vagal activity through GLP‑1 receptors expressed by myenteric neurons.34 Delayed gastric emptying further reduces postprandial glycemia.34 GLP‑1 is then degraded by a proteolytic enzyme dipeptidyl peptidase‑4, which is found in several tissues in the human body. The plasma half‑life of GLP‑1 after secretion is about 1.5 to 5 minutes.35 Two classes of drugs are available to increase GLP‑1 signaling: dipeptidyl peptidase‑4 inhibitors and GLP‑1RAs.
GLP‑1RAs are commonly used in clinical practice for the treatment of T2DM. This class of drugs includes semaglutide, liraglutide, dulaglutide, albiglutide, exenatide, lixisenatide, and tirzepatide. GLP‑1 secreted after meals controls glucose metabolism through different mechanisms: 1) by increasing β-cell insulin secretion; 2) by reducing glucagon secretion; 3) by blunting gastric motility and emptying, and decreasing appetite; and 4) by improving insulin sensitivity. Accordingly, treatment with GLP‑1RAs results in reducing the levels of glucose.36 Of interest, these drugs have shown a better safety profile with a lower risk of hypoglycemia, as compared with other antidiabetics, such as sulfonylureas or glinides.37 Other side effects include nausea, vomiting, and diarrhea due to their binding to the GLP‑1 receptor expressed in the central nervous system. The same mechanism is also responsible for the main “favorable” side effect, that is, weight loss (up to 20%) due to reduction of appetite and delayed gastric emptying with slower glucose absorption.36,38 As a result, these drugs have shown promise as a possible antiobesity treatment.39,40
Beneficial effects of glucagon‑like peptide‑1 receptor agonists on the cardiovascular system
The effects of GLP‑1RAs on the CV system seem to go beyond the mere prevention of CVDs by means of weight reduction. The main effects of GLP‑1RAs on the CV system are summarized in Figure 1.
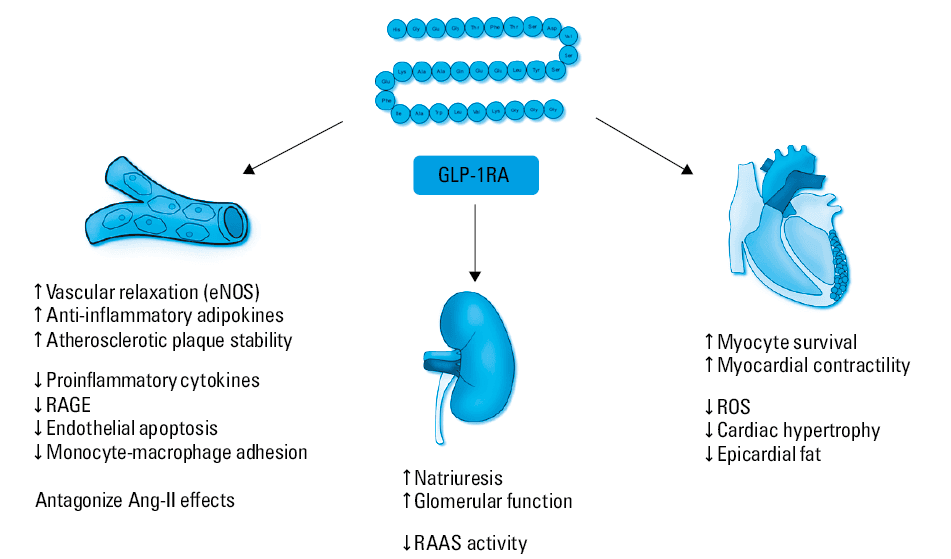
Abbreviations: Ang‑II, angiotensin II; eNOS, endothelial nitric oxide synthase; RAAS, renin‑angiotensin‑aldosterone system; RAGE, receptor for advanced glycation end products; ROS, reactive oxygen species
In the heart, GLP‑1 receptor is expressed in cardiomyocytes, especially near the sinoatrial node.41 Treatment with GLP‑1RAs protects these cells against interleukin (IL)-1β–induced ROS production.42 Indeed, GLP‑1RA use was associated with reduced mitochondrial ROS production in animal models treated with oxidized low‑density lipoproteins.43 Among mediators of such effects, studies identified a deleterious scavenger receptor, lectin‑type oxidized low‑density lipoprotein receptor 1.44 Furthermore, GLP‑1RAs attenuate cardiac hypertrophy via the 5'-monophosphate‑activated protein kinase (AMPK) / mammalian target of rapamycin signaling pathway.45 Consequently, GLP‑1RAs favor cardiomyocyte survival and ameliorate cardiac contractility.46
A potential beneficial effect of GLP‑1RAs on visceral / ectopic fat deposit formation has been recently hypothesized. In particular, the use of GLP‑1RAs might be promising for reducing epicardial fat thickness. Epicardial fat expresses GLP‑1 receptor in both diabetic and nondiabetic individuals.47 Recent studies have shown that treatment with GLP‑1RAs reduces epicardial fat thickness by up to 20%–30%,48,49 confirming the beneficial effect of these drugs in CVD prevention.
Regarding the effects on vessels, GLP‑1 receptor is expressed in endothelial cells,50 and GLP‑1RAs favor vascular relaxation via the AMPK / protein kinase B pathway51 and via endothelial nitric oxide synthase activation.52-54 Also, GLP‑1RAs prevent dysfunctional activation of endothelial cells by inhibiting phosphorylation of nuclear factor κ-light‑chain‑enhancer of activated B cells55 and blunting the expression of proinflammatory mediators, such as edothelin‑1 and ILs.56 Furthermore, GLP‑1RAs reduce the production and activation of angiotensin II,57,58 with beneficial effects on both endothelial and vascular smooth muscle cells.54,59 Through their antidiabetic effects, they reduce the levels of AGEs as well as their receptor, thus preventing endothelial cell apoptosis.60,61
As previously mentioned, GLP‑1RA treatment is associated with direct anti‑inflammatory effects.62 In an atherosclerosis model, these drugs showed potential for preventing immune cell accumulation in the arterial wall by blunting the levels of TNF-α, monocyte chemoattractant protein‑1,63 intercellular adhesion molecule‑1,53 vascular cell adhesion protein,55,64 and metalloproteinases.65 GLP‑1RAs also reduce systemic levels of proinflammatory cytokines (TNF-α, IL‑1β, IL‑6),66,67 while increasing the levels of anti‑inflammatory mediators, such as adiponectin.66 As a consequence, GLP‑1RA treatment reduces atherosclerotic inflammation and foam cell formation, and improves plaque stability by blunting matrix metallopeptidase‑9 and facilitating the formation of plaque collagen and fibrous cap.61,68-70
Impact of treatment with glucagon‑like peptide‑1 receptor agonists on reduction of cardiovascular outcomes: recent evidence from clinical trials
Over the last decade, several randomized controlled trials (RCTs) have demonstrated the beneficial role of GLP‑1RAs in preventing CVDs in patients with T2DM (Table 1). The main primary end points of these studies were myocardial infarction, CV death, or stroke. A majority of these trials showed a reduction in primary end points in the group treated with GLP‑1RAs, with the exception of the ELIXA (Evaluation of Lixisenatide in Acute Coronary Syndrome) trial,71 which reported almost no difference in the rate of CV events between the treated and untreated patients (lixisenatide group, 13.4% vs controls, 13.2%). This might be due to several factors, including a short follow‑up (up to 1.1 years) and inclusion of patients with previous coronary events within 180 days, which increased the risk of recurrent events. The most promising results were reported in the Harmony Outcomes72 (albiglutide group, 7% vs controls, 9%) and AMPLITUDE‑O73 (efpeglenatide group, 7% vs controls, 9.2%) studies. The EXSCEL (Exenatide Study of Cardiovascular Event Lowering)74 had the largest sample size (14 752 patients), and the REWIND (Researching Cardiovascular Events With a Weekly Incretin in Diabetes) study75 had the longest follow‑up (5.4 years). The reduced rate of clinical events showed in the REWIND study75 (dulaglutide group, 12% vs controls, 13.4%) highlights the importance of continuing the treatment for an extended period. To date, the PIONEER‑6 (Peptide Innovation for Early Diabetes Treatment) study76 was the only one specifically evaluating CV effects of an oral GLP‑1RA formulation (semaglutide 14 mg/day), and showed a lower rate of CV events in the treated group (semaglutide group, 3.8% vs controls, 4.8%). These findings are particularly important, since oral drug intake is generally preferred due to simplicity and better patient adherence.
Tirzepatide acts as an agonist for both GLP‑1 receptors and GIP receptors. Data from RCTs showed that this drug outperformed other GLP1‑RAs in terms of glucose control, and its use was associated with weight reduction by up to 20.9% in the SURMOUNT‑1 trial.77 Although to date there is no available trial directly comparing this agent with other GLP1‑RAs, tirzepatide seems to induce greater weight loss than any other available medication, based on post hoc analyses.78,79 For this reason, the American Diabetes Association (ADA) now consider tirzepatide, along with semaglutide, as an agent with very high efficacy for weight loss.80 With regard to its impact on CV outcomes, tirzepatide is not currently considered an incretin mimetic with proven CV benefits. The available trials only explored safety end points, and showed favorable results.81 The ongoing SURPASS‑CVOT trial,82 enrolling patients with T2DM and BMI greater than or equal to 25 kg/m2, will compare tirzepatide and dulaglutide for noninferiority and superiority with respect to the composite end point of death from CV causes, nonfatal myocardial infarction, or nonfatal stroke over a period of 54 months. At the moment, evidence on the potential beneficial effect of GLP‑1RAs in patients with heart failure with preserved ejection fraction is limited to the STEP‑HFpEF trial (Semaglutide in Patients with Heart Failure with Preserved Ejection Fraction and Obesity).83 A total of 529 nondiabetic patients were enrolled and randomly assigned to receive 2.4 mg of semaglutide subcutaneously or placebo once a week for 13 months. Of interest, semaglutide met both primary end points, that is, body weight loss and reduction of HF symptoms assessed by the Kansas City Cardiomyopathy Questionnaire. Furthermore, the treated group showed greater improvement in the 6‑minute walking test. The mean percentage reduction of circulating C‑reactive protein levels was also greater in the treated group than in controls (–43.5% vs –7.3%, respectively), indicating that GLP‑1RAs can effectively reduce inflammation, and confirming their potential applicability in the management of dysmetabolism, beyond T2DM treatment.
In the 2023 ADA guidelines,84 GLP‑1RAs were indicated as first‑line therapy for T2DM patients with obesity or those at a high risk of CVDs. Later that year, such recommendations were also implemented in the ESC guidelines.15
In November 2023, results of the SELECT (Semaglutide Effects on Heart Disease and Stroke in Patients with Overweight or Obesity) trial84 were published. It was the first study specifically designed to assess the role of GLP‑1RAs in preventing CV and CBV outcomes in patients with pre‑existing CVDs and overweight or obesity. The primary end point was the composite of CV death, nonfatal myocardial infarction, or stroke. A total of 17 604 patients aged 45 or older (mean age, 62 years), with pre‑existing CVD and BMI of 27 kg/m2 or higher were included. The participants were randomized to receive either semaglutide 2.4 mg subcutaneously once a week or placebo. The mean follow‑up was 39.8 months. There was a higher prevalence of men in both groups (72.2% vs 72.5% in semaglutide and placebo groups, respectively). A majority of the enrolled patients were obese according to the BMI categories (mean BMI, 33.3 vs 33.4 kg/m2, respectively, in semaglutide and placebo groups). The treatment met the primary end point, showing 20% less CV and CBV events, as compared with placebo (6.5% vs 8%; hazard ratio, 0.8; 95% CI, 0.72–0.9; P <0.001).85 However, adverse effects that caused treatment discontinuation were more frequent in the semaglutide group (16.6% vs 8.2%), mostly due to gastrointestinal disorders. Collaterally, the trial reported a reduction of 3.3 mm Hg in systolic blood pressure and a 37.8‑percentage‑point decrease in high‑sensitivity C‑reactive protein levels in the patients treated with semaglutide.85 These data support the use of GLP‑1RAs for CV and CBV prevention in obese patients, even those without diabetes.
Conclusions
GLP‑1RAs are established drugs for the treatment of T2DM. Given their striking effects on body weight, GLP1‑RAs are being increasingly often regarded as a possible antiobesity treatment, with additional beneficial effects on CV and CBV complications. While the Food and Drug Administration has already approved GLP1‑RAs for the treatment of obesity (with or without diabetes) in the United States, this class of drugs is not approved to be prescribed in the absence of diabetes in Europe. Recent data from the SELECT trial85 confirmed the beneficial CV and CBV effects of semaglutide in nondiabetic patients, and will hopefully pave the way for its broader use.
- Inoue Y, Qin B, Poti J, et al. Epidemiology of obesity in adults: latest trends. Curr Obes Rep. 2018; 7: 276‑288. | Crossref
- Dobbs R, Sawers C, Thompson F, et al. Overcoming Obesity: an Initial Economic Analysis. McKinsey Global Institute; 2014.
- Tremmel M, Gerdtham UG, Nilsson PM, et al. Economic burden of obesity: a systematic literature review. Int J Environ Res Public Health. 2017; 14: 435. | Crossref
- Preda A, Carbone F, Tirandi A, et al. Obesity phenotypes and cardiovascular risk: from pathophysiology to clinical management. Rev Endocr Metab Disord. 2023; 24: 901‑919. | Crossref
- Dorresteijn JA, Visseren FL, Spiering W. Mechanisms linking obesity to hypertension. Obes Rev. 2012; 13: 17‑26. | Crossref
ARTICLE INFORMATION