Immune checkpoint inhibitor–induced central diabetes insipidus in the course of panhypophysitis

 CC BY 4.0
CC BY 4.0
Immune checkpoint inhibitor–induced central diabetes insipidus in the course of panhypophysitis
Hypophysitis is a common immune‑related adverse effect of treatment with immune checkpoint inhibitors (ICIs; anticytotoxic T‑lymphocyte–associated protein 4 and antiprogrammed cell death protein 1) that occurs in up to 10% of patients with cancer, especially those receiving combination treatment.1 The diagnosis is based on the clinical picture and hormonal test results indicating anterior pituitary deficiency, and is supported by magnetic resonance imaging (MRI) findings.2 Arginine vasopressin deficiency (AVP‑D, also known as central diabetes insipidus) due to ICI‑induced hypophysitis is extremely rare3; it occurs more often as a result of pituitary metastases, particularly when the stalk is involved. AVP‑D in a patient with a coexistence of hypophysitis and pituitary metastasis has also been described recently.4
We present a case of a 46‑year‑old man with AVP‑D in the course of ICI‑induced panhypophysitis. The patient’s medical history included BRAF mutation–positive cutaneous melanoma involving the chest wall at the stage of dissemination to the lungs. Chest computed tomography (CT) scans revealed progressive disease with multiple metastases in both lungs. Combined immunotherapy with nivolumab (1 mg/kg intravenously [IV]) and ipilimumab (3 mg/kg IV) was initiated. After the second course of the treatment, the patient reported severe headache, fatigue, nausea, and vomiting, but without any visual disturbances. The symptoms resolved following prednisone treatment at a dose of 1 mg/kg body weight, gradually downtitrated afterwards. Hormonal evaluation revealed panhypopituitarism requiring hydrocortisone, L‑thyroxine, and testosterone replacement therapy (Supplementary material, Table S1). Approximately 2 weeks since the onset of the first symptoms, the patient reported severe polyuria (12 l/24 h) and polydipsia with nycturia. Laboratory test results showed low urine osmolality (192 mOsm/kg H2O; reference range, 270–295 mOsm/kg H2O), specific gravity of 1.005, and plasma osmolality in the upper limit of normal (294 mOsm/kg). The diagnosis of AVP‑D was confirmed, and treatment with sublingual desmopressin resulted in a decrease in diuresis, resolution of nycturia, and an increase in urine osmolality. Pituitary MRI showed an enlarged pituitary gland with stalk thickening and strong contrast enhancement suggesting hypophysitis (Figure 1A–1C). No typical hyperintense signal of the posterior pituitary was visualized on T1‑weighted images (Figure 1A).
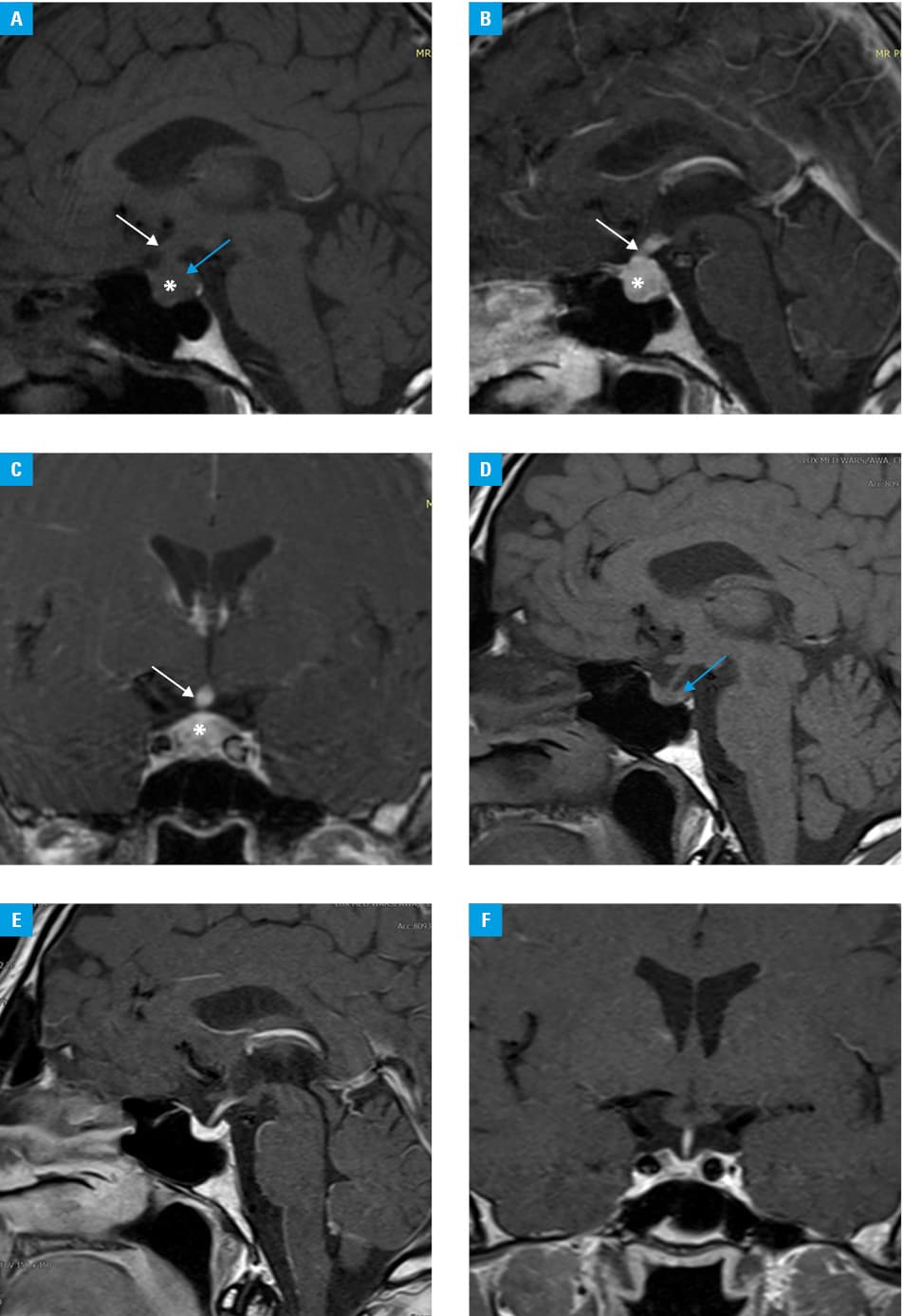
At 4- and 15‑month follow‑up visits, persistent hypopituitarism with AVP‑D was confirmed (Supplementary material, Table S1). The patient denied any headaches, visual disturbances, nausea, or vomiting. Polydipsia and polyuria were well controlled while taking desmopressin. Pituitary MRI showed regression of the inflammatory process resulting in a partially empty sella, persistent lack of the posterior pituitary bright spot; also, no metastatic lesions were visible (Figure 1D–1F). Chest CT showed a complete regression of pulmonary metastases following the ICI therapy. The patient continues the treatment with nivolumab (480 mg IV) along with the hormonal replacement therapy.
We presented a case of panhypophysitis induced by cancer immunotherapy with ICIs, as indicated by the clinical course, pituitary MRI findings, hypopituitarism, and good response to high‑dose prednisone. Although AVP‑D is an extremely rare toxicity of immunotherapy, it may be observed in an increasing number of patients as indications for ICIs expand. Apart from hypophysitis, a differential diagnosis in the case of AVP‑D should always include a pituitary metastasis; therefore, active surveillance is recommended in such cases.5
- Castillero F, Castillo‑Fernandez O, Jimenez‑Jimenez G, et al. Cancer immunotherapy‑associated hypophysitis. Future Oncol. 2019; 15: 3159‑3169. | Crossref
- Catford S, Wang YY, Wong R. Pituitary stalk lesions: systematic review and clinical guidance. Clin Endocrinol (Oxf). 2016; 85: 507‑521. | Crossref
- Stelmachowska‑Banaś M, Czajka‑Oraniec I. Management of endocrine immune‑related adverse events of immune checkpoint inhibitors: an updated review. Endocr Connect. 2020; 9: R207‑R228. | Crossref
- Fosci M, Pigliaru F, Salcuni AS, et al. Diabetes insipidus secondary to nivolumab‑induced neurohypophysitis and pituitary metastasis. Endocrinol Diabetes Metab Case Rep. 2021; 2021: 20‑0123. | Crossref
- Caturegli P, Di Dalmazi G, Lombardi M, et al. Hypophysitis secondary to cytotoxic T‑lymphocyte‑associated protein 4 blockade: insights into pathogenesis from an autopsy series. Am J Pathol. 2016; 186: 3225‑3235. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION