A rare case of primary diffuse large B-cell lymphoma of the parotid gland misinterpreted as Warthin tumor



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
A rare case of primary diffuse large B-cell lymphoma of the parotid gland misinterpreted as Warthin tumor
Primary diffuse large B‑cell lymphoma (DLBCL) of the salivary gland is a rare infiltrative neoplasm associated with destruction of the salivary gland. This high‑grade lymphoma constitutes 2%–5% of salivary gland tumors and 5% of extranodal lymphomas. Considering that most patients do not present systemic manifestations of the disease, surgery with histologic confirmation remains a critical element of diagnosis. The features of DLBCL of the parotid gland include a unilateral mass, in some cases accompanied by cervical lymphadenopathy, pain, or facial nerve paresis.1,2
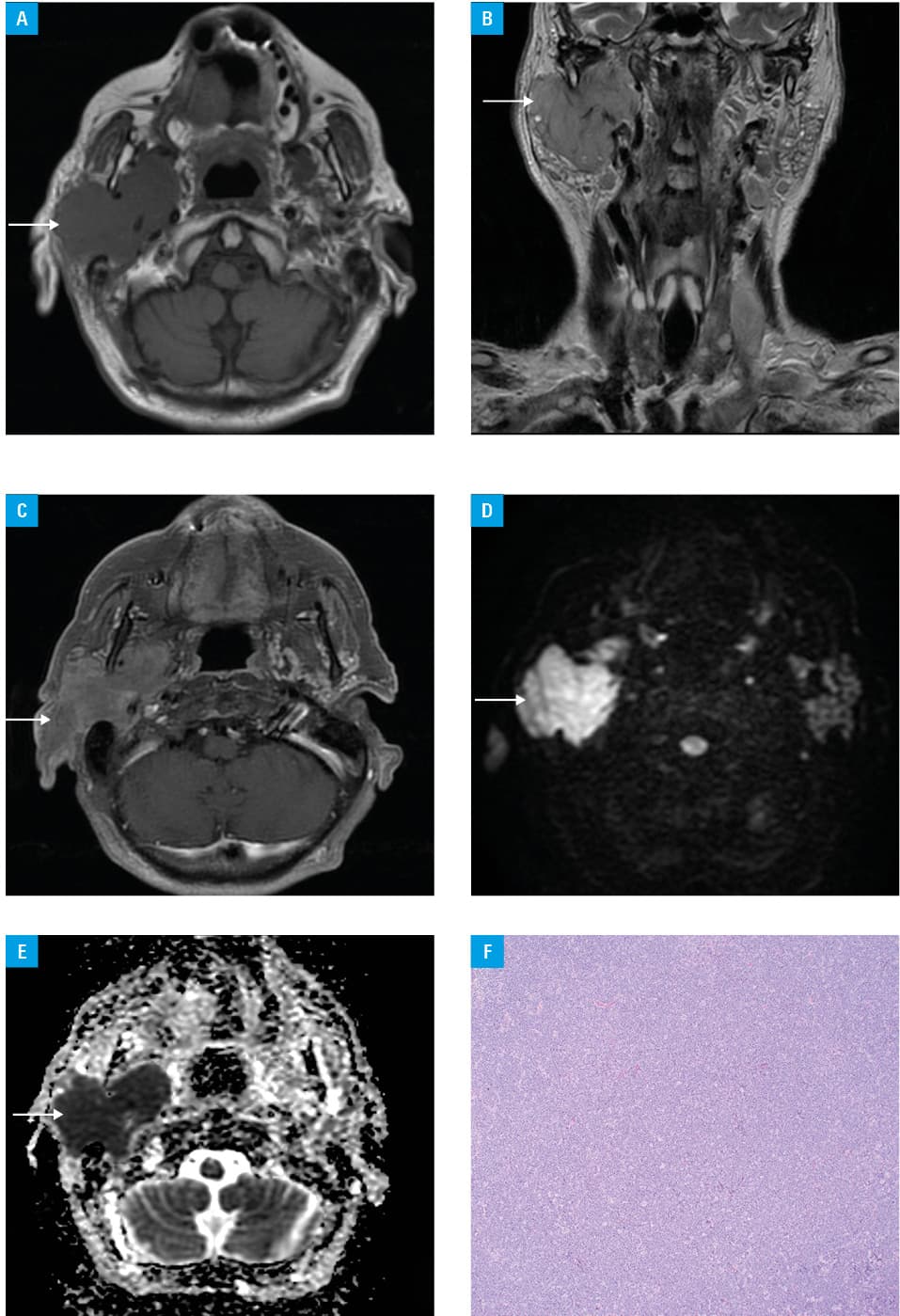
We present a case of an 85‑year‑old woman with a right parotid gland tumor, which was palpable for 6 months and growing slowly. Preoperative magnetic resonance imaging (MRI) revealed an extensive, well‑circumscribed and rather homogeneous mass, hypointense on T1‑weighted images, with an intermediate signal on T2‑weighted images, showing high signal intensity on diffusion‑weighted imaging (DWI) and low signal intensity on apparent diffusion coefficient (ADC) maps, which indicted features of restricted diffusion (Figure 1A–1E). The lesion was located within the superficial and deep part of the right parotid gland; it measured 51 mm × 34 mm × 52 mm. The MRI report suggested only Warthin tumor (WT; lymphomatous papillary cystadenoma). The patient was qualified for surgery. Parotidectomy was performed with total tumor resection. The pathologic findings were consistent with a diagnosis of DLBCL (Figure 1F).
We present this case of large parotid gland DLBCL in order to discuss the reasons for misdiagnosis on MRI and to underline the nonspecific clinical symptoms reported by the patient that delayed a correct diagnosis. The patient presented with DLBCL located exclusively in an extremely rare, extranodal location with no systemic manifestations that would indicate the presence of lymphoma (fever, night sweats, weight loss), and no history of infections or autoimmune diseases. Moreover, the presence of a slow‑growing, painless mass and intact facial nerve function indicated a benign neoplasm. Lymphomas usually present low signal intensity on T1‑weighted images, a low or isointense signal on T2‑weighted images, and variable contrast enhancement. Lymphomas, as highly cellular tumors, appear hyperintense on DWI and hypointense on ADC maps due to their restricted diffusion.3,4 The preoperative MRI report suggested WT because it is the most common tumor of the parotid gland, and it shows features of restricted diffusion. It should be highlighted that WT is usually a heterogeneous mass presenting faint enhancement, and that large WTs tend to have a higher proportion of cystic content. On the contrary, the parotid lesion in our case had a generally homogeneous appearance. WT usually shows cellular components with accumulated microscopic cysts containing proteinous fluid with foamy cells, red cells, and neutrophils recognized as high‑signal‑intensity foci on T1‑weighted images and as hypointense areas on T2‑weighted images.5
We would like to emphasize that rare entities, such as DLBCLs, can occur in everyday clinical practice and that they should be considered and included in a differential diagnosis when there are unusual features of what appears to be a typical disease. The presented case is extremely rare and could pose a diagnostic challenge.
- Gupta A, Lee JA, Nguyen SA, Lentsch EJ. Primary diffuse large B‑cell lymphoma of the major salivary glands: increasing incidence and survival. Am J Otolaryngol. 2021; 42: 102938. | Crossref
- Gutierrez‑Alvarez M, Martinez C, Campollo Lopez AP, et al. Warthin’s tumor of the parotid gland with degeneration to diffuse large B‑cell lymphoma: a case report and review of literature. Cureus. 2023; 15: e36802. | Crossref
- Gökçe E, Beyhan M. Advanced magnetic resonance imaging findings in salivary gland tumors. World J Radiol. 2022; 14: 256‑271. | Crossref
- Chang YJ, Huang TY, Liu YJ, et al. Classification of parotid gland tumors by using multimodal MRI and deep learning. NMR Biomed. 2021; 34: e4408. | Crossref
- Jia CH, Wang SY, Li Q, et al. Conventional, diffusion, and dynamic contrast‑enhanced MRI findings for differentiating metaplastic Warthin’s tumor of the parotid gland. Sci Prog. 2021; 104: 368504211018583. | Crossref
ARTICLE INFORMATION