Liver cysts are among the most frequent focal lesions found on hepatic ultrasonography, with a high prevalence of 15% to 18% reported in the United States. They are most commonly simple cysts, but parasitic or malignant etiology should be considered in some cases.1
A 75‑year‑old woman with metabolic syndrome and unusual abdominal complaints, with previously diagnosed irritable bowel syndrome and gastroesophageal reflux disease, underwent abdominal ultrasonography that revealed focal liver lesions. The main tumor, localized in the right lobe, consisted of a large, mostly fluid, thick‑walled cyst with a diameter of 96 mm × 89 mm and a solid 14‑mm layer comprising small cysts. Additionally, a conglomerate of thin‑walled cysts with a total diameter of 35 mm × 21 mm was found in the left lobe. On the first computed tomography (CT) scan, the entire right lobe tumor was described as a polycystic area (Figure 1A). Serologic tests excluded parasitic nature of the cyst. A consulting surgeon suggested a watch‑and‑wait approach involving observation of the liver lesions.
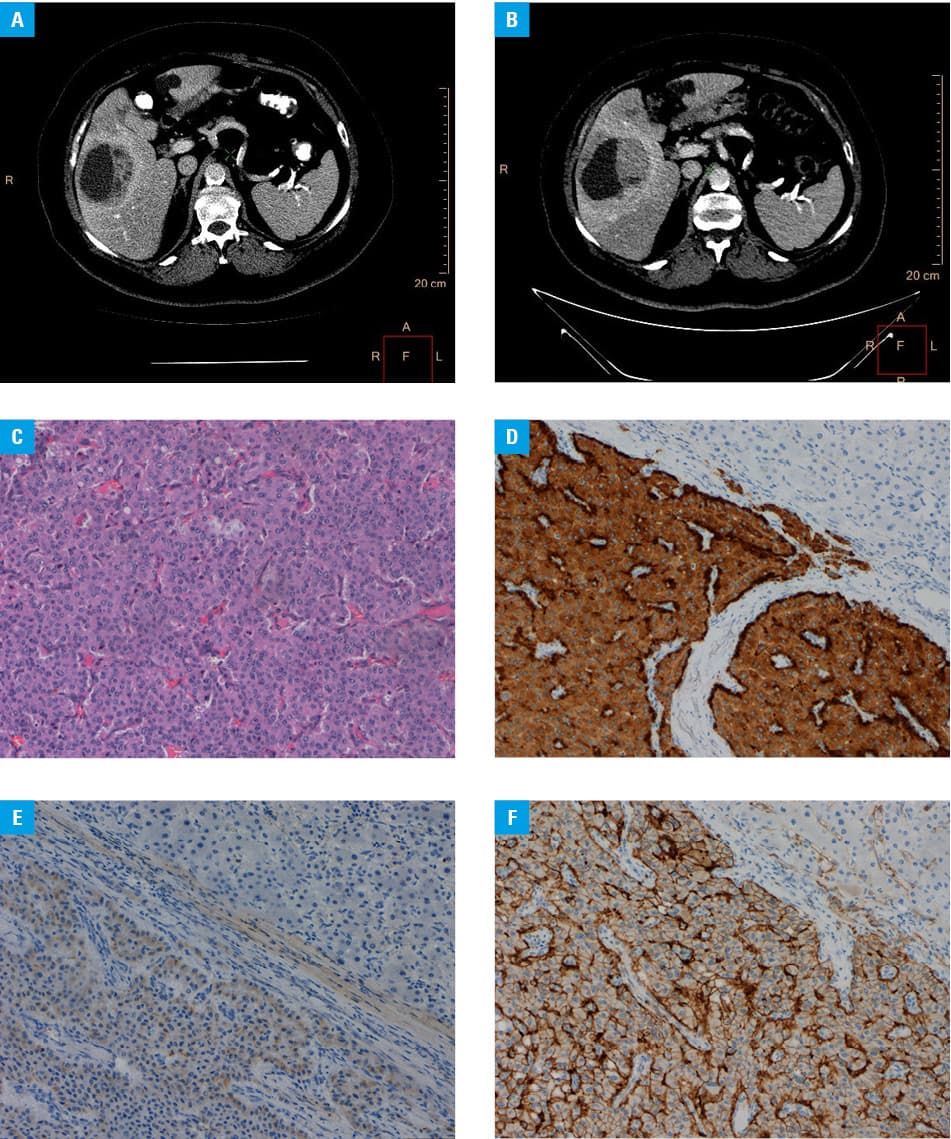
A year later, on a follow‑up CT scan, the diameter of the large tumor did not change, but the solid part of the tumor was found to be larger than before and showed enhancement after contrast administration (Figure 1B). Liver function tests and neoplastic markers were within normal ranges. Based on the significant changes observed on the second CT scan, the patient was referred to a surgery department with a suspected cystadenoma / carcinoma of the liver. Resection of the 3 liver segments (15.5 cm × 10 cm × 9 cm) was performed, with mainly solid tumor showing an expanding type of growth. Histopathologic examination confirmed that it was a neuroendocrine tumor (NET; Figure 1C–1F), and additional therapy with lanreotide was introduced. Further diagnostics using positron emission tomography with [68Ga]Ga‑DOTA‑0‑Tyr3‑Octreotate did not reveal other focal lesions and showed enhanced expression of somatostatin receptors. During over 2 years of follow‑up, no focal changes were found on imaging.
Primary hepatic NETs (PHNETs) are extremely rare, comprising only approximately 0.3% of all gastrointestinal NETs, and only 200 cases have been described in the medical literature to date.2 Establishing a diagnosis of PHNET is particularly difficult, because NETs most commonly occur in the small intestine, pancreas, or large intestine, and metastasize to the liver in over 40% of cases.3 PHNETs are more frequent in middle‑aged and older women, typically with minimal symptoms (over 60% of patients experience nonspecific abdominal pain). Less than 7% of patients present clinical symptoms of carcinoid syndrome. PHNETs grow slowly and are commonly localized in the right lobe. On imaging, PHNETs appear as a cystic or solid‑cystic structure. The final diagnosis is based on histopathologic examination. The treatment of choice is surgical resection or liver transplant for incidental cases, and pharmacotherapy with somatostatin analogues for chronic cases.2,4,5
In conclusion, despite its rarity, and in light of the increasing prevalence of gastrointestinal NETs, PHNET should be considered in a differential diagnosis, especially in older women with nonspecific abdominal pain and a large, atypical cystic mass in the liver.
- Rawla P, Sunkara T, Muralidharan P, Raj JP. An updated review of cystic hepatic lesions. Clin Exp Hepatol. 2019; 5: 22‑29. | Crossref
- Wong PC, She WH, Khoo US, Cheung TT. A case of primary hepatic neuroendocrine tumor and literature review. Case Rep Oncol. 2021; 14: 90‑97. | Crossref
- Frilling A, Modlin IM, Kidd M, et al; Working Group on Neuroendocrine Liver Metastases. Recommendations for management of patients with neuroendocrine liver metastases. Lancet Oncol. 2014; 15: e8‑e21. | Crossref
- Li YF, Zhang QQ, Wang WL. Clinicopathological characteristics and survival outcomes of primary hepatic neuroendocrine tumor: a Surveillance, Epidemiology, and End Results (SEER) population‑based study. Med Sci Monit. 2020; 26: e923375. | Crossref
- Song JE, Kim BS, Lee CH. Primary hepatic neuroendocrine tumor: a case report and literature review. World J Clin Cases. 2016; 4: 243‑247. | Crossref
ARTICLE INFORMATION