Atrial myxoma is the most prevalent benign primary heart tumor of mesenchymal origin, with a prevalence of 0.0017% to 0.19%. Approximately 75% of myxomas originate in the left atrium (LA), 20% arise from the right atrium, and 5% can be found in both atria or the ventricles.1,2
Cardiac myxomas, though biologically benign, can have serious consequences due to their potential for embolization, and are often referred to as “functionally malignant.” Atrial myxomas are typified by a triad that consists of intracardiac obstruction, embolic manifestations, and constitutional symptoms.3
Clinical manifestation of myxoma varies significantly and is primarily determined by the tumor size, its surface, location, and mobility. Atrial myxoma poses a unique diagnostic challenge due to its potential to remain entirely asymptomatic (10% of cases). It can also cause life‑threatening systemic embolization (neurologic complications, 30%–50% of cases) or sudden cardiac death.4
A 67‑year‑old man was urgently referred from outpatient care to the Department of Cardiology at the Medical University in Lublin, Poland due to the presence of LA myxoma that was diagnosed on routine echocardiography. The patient experienced minor, occasional shortness of breath episodes that started a month ago, having been completely asymptomatic prior to that time. In‑depth echocardiography confirmed an exceptionally large myxoma in the LA, associated with a substantial massive thrombus adhering to the inferior wall of the myxoma on the side of the LA. The myxoma was floating from the LA to the left ventricle (Figure 1A–1C). The mitral valve function was undisturbed.
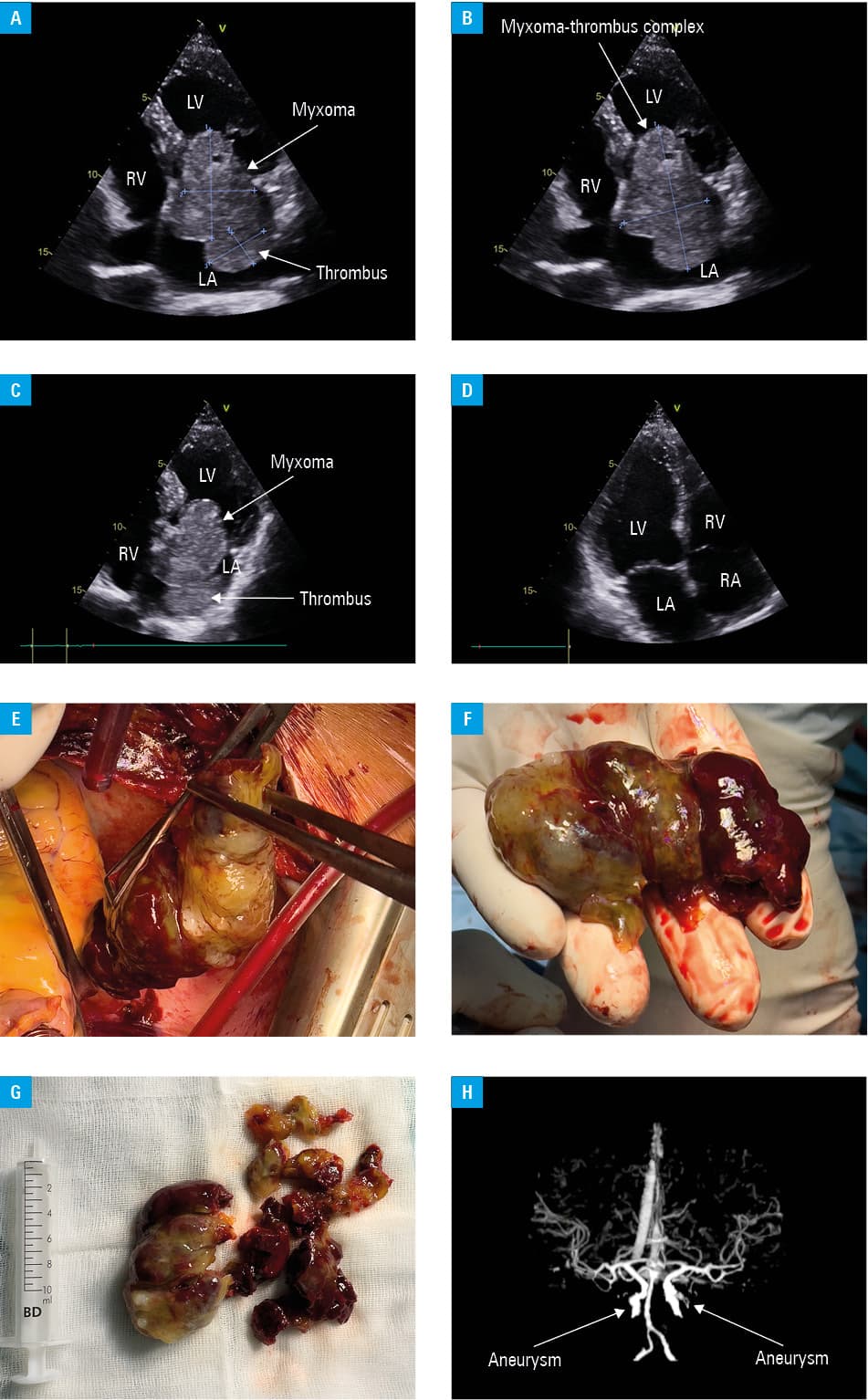
Abbreviations: LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle
After a heart team consultation, the patient was immediately referred for urgent surgical treatment to avoid embolic complications. The LA was accessed via median sternotomy and during cardiopulmonary bypass (standard ascending aortic and bicaval venous cannulation). During the first step of the procedure, the thrombus was carefully removed; it was extremely fragile, and during its extraction from the LA, massive thrombus fragmentation started. That was a crucial part of the procedure due to a high risk of small thrombus parts being transferred into the bloodstream if unremoved. In the next step, after surgeons confirmed that all thrombotic masses had been removed, a narrow pedicle attached to the atrial septum was localized, and the gigantic tumor was subsequently extracted from the LA (Figure 1D–1G). The tumor dimensions were 8 cm × 5 cm, and its surface was irregular. Aortic cross‑clamp time was 29 minutes, and cardiopulmonary bypass time was 42 minutes. Throughout the procedure, the bispectral index was monitored; the value of 60 was constant, confirming a low risk of periprocedural ischemic events. The time from the myxoma diagnosis to its complete surgical extraction was less than 24 hours. Follow‑up brain computed tomography revealed a small ischemic lesion and confirmed left internal carotid artery and right anterior cerebral artery aneurysms with associated vascular malformations (Figure 1H). The patient was discharged in good condition. Histopathologic examination confirmed the myxoma diagnosis.
With early diagnosis and timely surgical intervention, patients with atrial myxomas can undergo successful treatment with low complication rates. Cerebral aneurysm is a condition rarely associated with myxoma.5
- Lee S, Park JS, Park J, et al. Comparison of clinical and echocardiographic characteristics between cardiac myxomas and masses mimicking myxoma. Korean Circ J. 2020; 50: 822‑832. | Crossref
- Ezzeddine F, Haq IU, Pessanha BS, et al. Point‑of‑care ultrasound diagnosis of a giant left atrial mass. CASE. 2022; 6: 243‑246. | Crossref
- Islam A. Cardiac myxomas: a narrative review. World J Cardiol. 2022; 14: 206‑219. | Crossref
- Wen X, Chen Y, Yu L, et al. Neurological manifestations of atrial myxoma: a retrospective analysis. Oncol Lett. 2018; 16: 4635‑4639. | Crossref
- Chojdak-Łukasiewicz J, Budrewicz S, Waliszewska‐Prosół M. Cerebral aneurysms caused by atrial myxoma – a systematic review of the literature. J Pers Med. 2022; 13: 8. | Crossref
ARTICLE INFORMATION