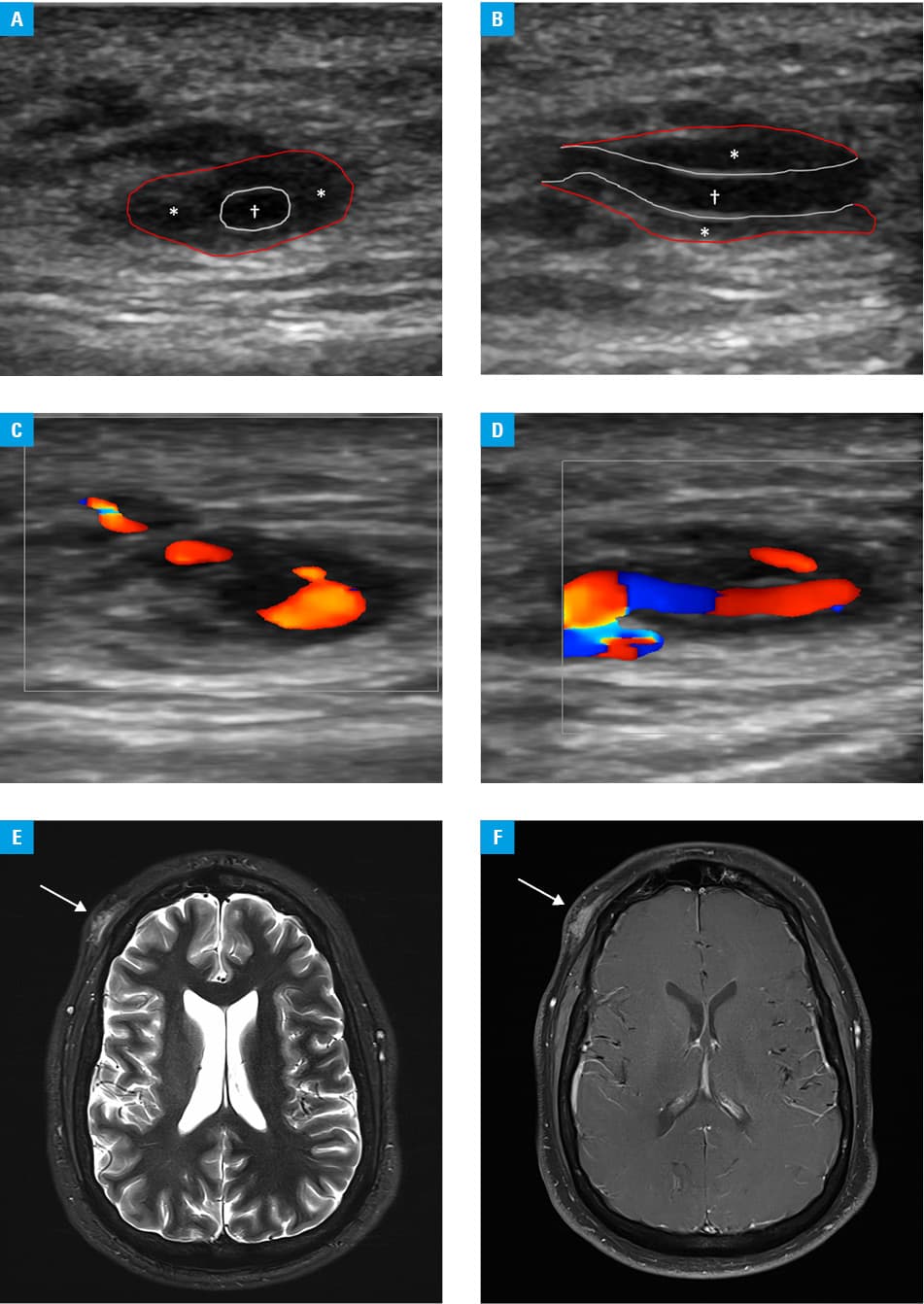
A 40‑year‑old man presented with tenderness and swelling of the right frontotemporal region lasting for about 3 years. The symptoms started after the patient had bumped his right temple against a Table’s edge, but their severity increased in the last few weeks. No further signs of potential giant cell arteritis were found, with unremarkable inflammation parameters. Ultrasonography (US) of the affected temporal region in transversal and longitudinal views revealed a hypoechoic, perivascular area with visible central arterial lumen of the right temporal artery (Figure 1A and 1B). Duplex US of the right temporal artery revealed a hypoechoic, perivascular area with central perfusion suggesting a halo sign. However, on closer examination, additional perfusion of subcutaneous hypoechoic areas and perfusion within the presumed halo sign were detected (Figure 1C and 1D). A pseudohalo sign caused by perivascular hematoma formation without lumen stenosis was suggested instead of a halo sign due to inflammatory vascular wall thickening with lumen stenosis. Temporal pseudoaneurysm was suspected; therefore, magnetic resonance imaging of the cranial arteries was performed, confirming pseudoaneurysm of the right temporal artery without potential inflammatory changes (Figure 1E and 1F). The patient underwent successful and uneventful surgical removal of the post‑traumatic temporal pseudoaneurysm, without any histologic abnormalities indicating potential vasculitis on subsequent biopsy.
Duplex US is the first‑line examination to confirm temporal pseudoaneurysm. During the examination, different US signs may be detected, including a yin‑yang sign, to‑and‑fro pattern, or the abovementioned pseudohalo sign.1,2 Misdiagnosis of the latter with a halo sign, which is a classic US finding in cranial giant cell arteritis, should be avoided, especially in the cases with mismatching clinical signs and symptoms.3
- Balligand A, Mulquin N. Pseudoaneurysm of the superficial temporal artery after blunt trauma. Mayo Clin Proc. 2020; 95: 226‑227. | Crossref
- Park DH, Lee JK, Baik BS, et al. Traumatic hematoma‑based pseudoaneurysm of the superficial temporal artery in a 7‑year‑old boy: a case report. Arch Craniofac Surg. 2023; 24: 32‑36. | Crossref
- Dejaco C, Ramiro S, Bond M, et al. EULAR Recommendations for the use of imaging in large vessel vasculitis in clinical practice: 2023 update. Ann Rheum Dis. 2023 Aug 7. [Epub ahead of print]
ARTICLE INFORMATION