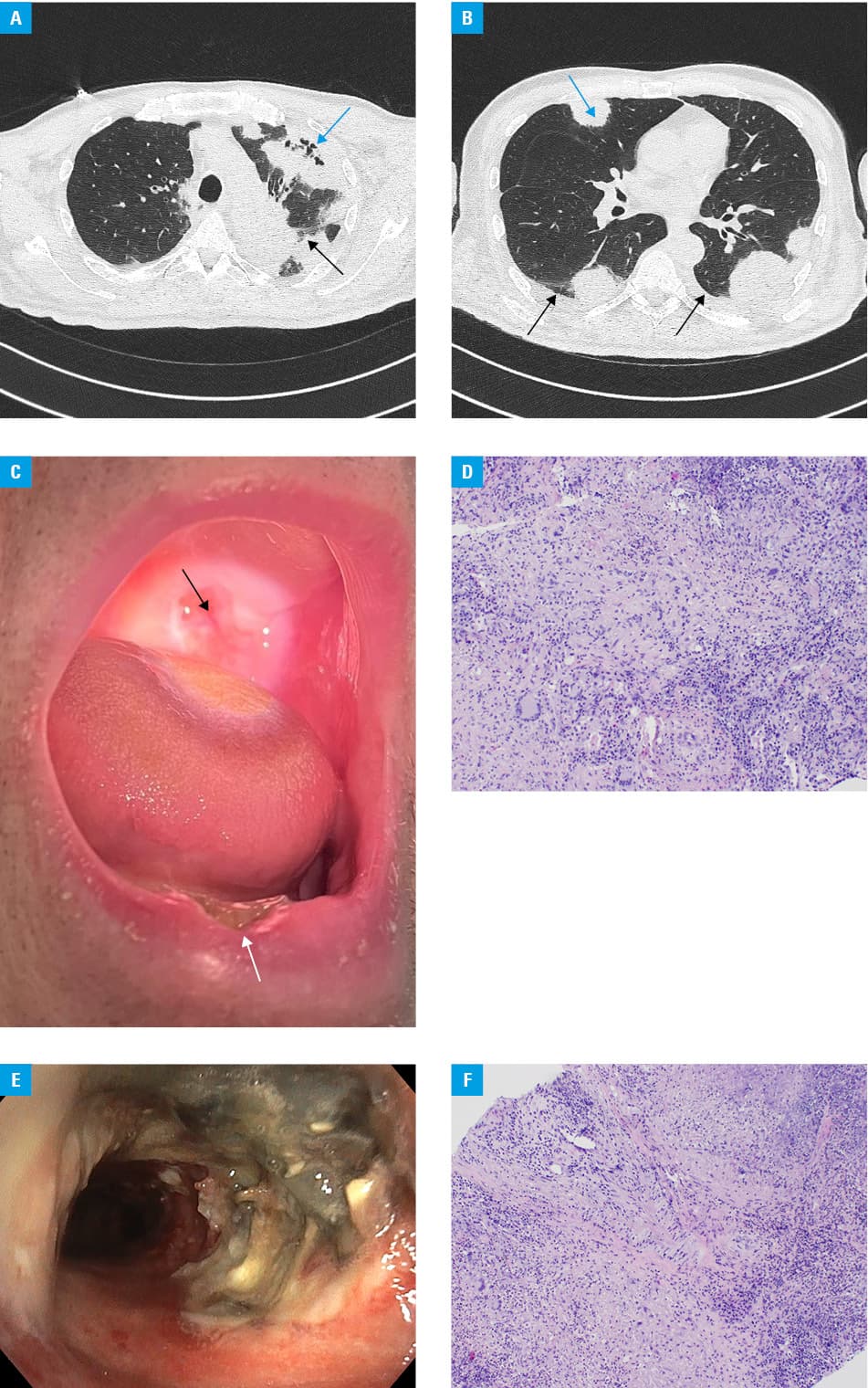
A 57‑year‑old man with a 40‑pack‑year smoking history was admitted to a hospital due to a brief loss of consciousness and right‑sided paresis that occurred more than 24 hours ago. Over the past 4 months, he experienced progressive health deterioration, cough, and 15 kg weight loss. Due to bilateral inflammatory changes on chest X‑ray examination, he received 2 empiric antibiotic therapies in an outpatient setting, which resulted in only slight improvement. Three months earlier, he experienced perforation of the left eardrum with subsequent persistent hearing loss. On admission, cerebral magnetic resonance showed ischemic stroke in both thalami. The National Institutes of Health Stroke Scale score was 4, and the Eastern Cooperative Oncology Group performance status was 3–4. Chest computed tomography showed bilateral pulmonary infiltrates involving the pleura, suggesting advanced malignancy (Figure 1A and 1B). Ultrasound‑guided transthoracic biopsy was performed. After completing conservative stroke treatment, while awaiting results, the patient was transferred to a hospice, where he continued symptomatic and oral antifungal therapy. After thrush subsided, lip, tongue, and palate ulcers appeared (Figure 1C). Histopathologic examination of the lung sample revealed chronic granulomatous inflammation with extensive necrosis (Figure 1D). Additional staining suggested a fungal infection. The patient was admitted to a pneumonology department for further diagnostics. Bronchoscopy showed tracheal ulceration and bilateral retention of bloody‑purulent secretions (Figure 1E). Bronchoalveolar lavage cultures revealed growth of multiple pathogens, including Pseudomonas aeruginosa and Staphylococcus aureus. Histopathologic examination of mouth ulceration samples revealed Actinomyces infection. Urinalysis revealed urinary casts, hematuria, and mild proteinuria. Both antiproteinase‑3 antineutrophil cytoplasmic antibody titer (1:1280; reference range [RR], <1:40) and level (>200 RU/ml; RR, <20 RU/ml) were highly elevated. The new clinical findings prompted histopathologic re‑examination of the lung sample, which revealed features of small vessel vasculitis (Figure 1F). European Alliance of Associations for Rheumatology classification criteria score for granulomatosis with polyangiitis (GPA) equaled 16, which justified the diagnosis.1 The disease activity was assessed as severe on the Birmingham Vasculitis Activity Score for Wegener granulomatosis.2 The patient received 3 pulse doses of methylprednisolone followed by weight‑based oral prednisone tapered according to the PEXIVAS regimen,1 repeated pulse doses of cyclophosphamide,1 a course of antibiogram‑guided intravenous antibiotics (ceftazidime, metronidazole, levofloxacin), voriconazole, and Pneumocystis jiroveci prophylaxis (cotrimoxazole thrice a week). Rituximab was considered but was unavailable for the first‑line treatment. Within 2 weeks, the patient improved dramatically and, on day 21, was discharged home to continue remission induction treatment.
GPA is a systemic disease caused by necrotizing granulomatous inflammation of the small vessels. Its rarity, various symptoms, and management by multiple specialists frequently delay diagnosis. Hearing impairment, cavitating pulmonary infiltrates, and upper and lower airway ulcers are common GPA manifestations. However, in our case, the first clinical symptom was ischemic stroke, which is rare in this entity.3,4
This case illustrates that patients with multiorgan symptoms might benefit from a multidisciplinary team consultation. It also shows that, even in a suggestive context, radiologic suspicion of malignancy should be verified with an appropriately conducted histopathologic examination whenever feasible.
- Hellmich B, Sanchez‑Alamo B, Schirmer JH, et al. EULAR recommendations for the management of ANCA‑associated vasculitis: 2022 update. Ann Rheum Dis. 2024; 83: 30‑47. | Crossref
- Mukhtyar C, Lee R, Brown D, et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann Rheum Dis. 2009; 68: 1827‑1832. | Crossref
- Wójcik K, Masiak A, Jeleniewicz R, et al. Association of antineutrophil cytoplasmic antibody (ANCA) specificity with demographic and clinical characteristics of patients with ANCA‑associated vasculitides. Pol Arch Intern Med. 2022; 132: 16187. | Crossref
- Tarte NN, Ceruti R, Tati V. An unusual neurological manifestation of granulomatosis with polyangiitis: a case report and literature review. Clin Case Reports. 2020; 8: 862‑866. | Crossref
ARTICLE INFORMATION