T-cell prolymphocytic leukemia with lung involvement presenting as crazy paving on high-resolution computed tomography

 CC BY 4.0
CC BY 4.0
T-cell prolymphocytic leukemia with lung involvement presenting as crazy paving on high-resolution computed tomography
T‑cell prolymphocytic leukemia (T‑PLL) is a rare mature T‑cell lymphoma1 with poor prognosis. The unified criteria for a diagnosis of T‑PLL2 include, among others, involvement of disease‑specific sites, for example, splenomegaly or effusions. T‑PLL is known for its predilection for infiltration of extramedullary sites, which are most frequently the pleura or the peritoneum, the skin, or the central nervous system. Periorbital, conjunctival edema is also frequently observed in patients with T‑PLL. While it is generally agreed that pleural effusion is a typical presentation of T‑PLL, involvement of the pulmonary alveolar septa and spaces is not. Here, we report a case of a patient with T‑PLL who presented with lung involvement mimicking proteinosis.
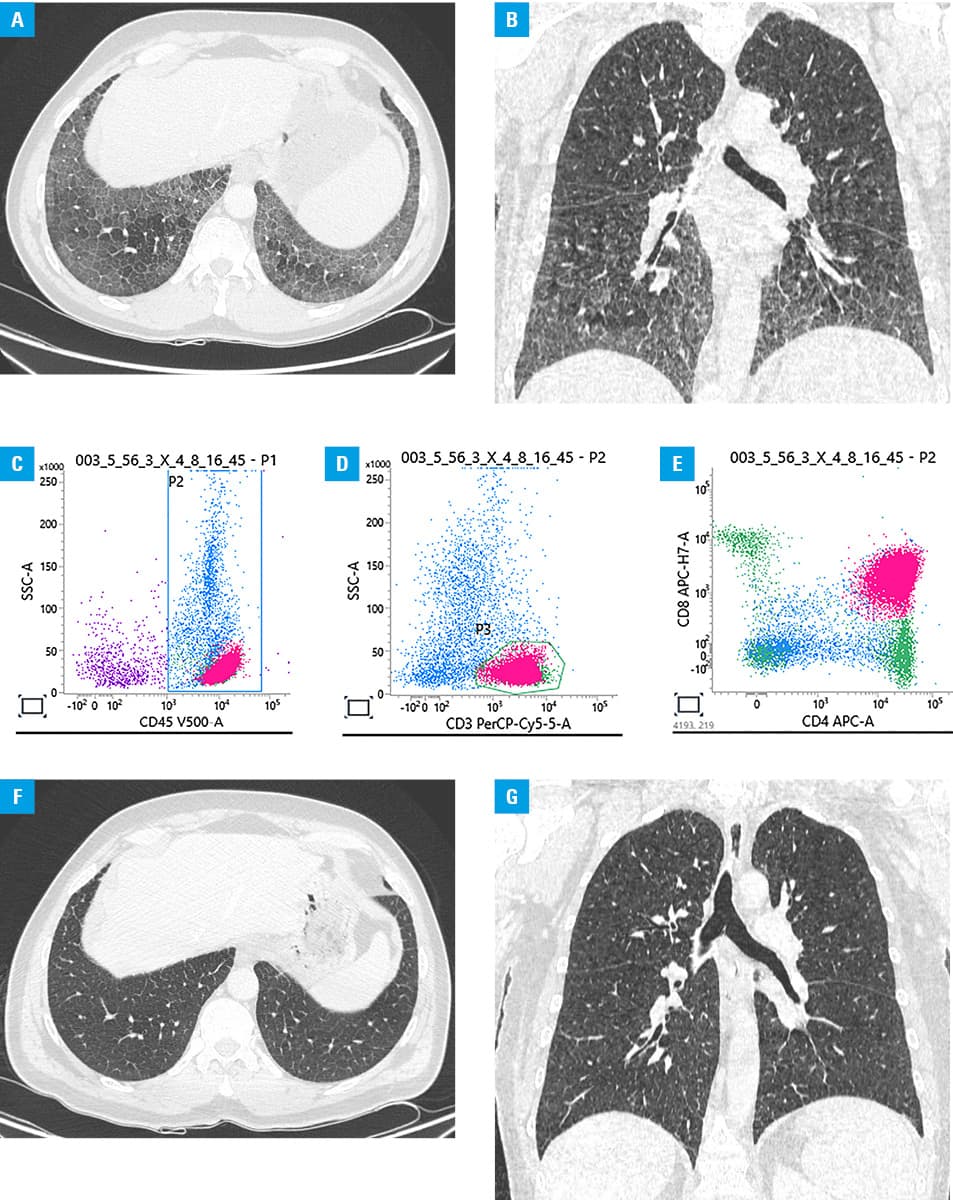
The 49‑year‑old man was diagnosed with T‑PLL in 2020 based on an analysis of complete blood count with differential flow cytometry (CD45+, CD3+, CD4+, CD8+, CD5+, CD2+, CD7+, TCRαβ+, TCRχδ–, CD45RO–, CD45RA–/dim CD1a–, TdT–, CD34–, CD117–, and CD10–), and chromosomal abnormality inv(14)(q11q32). Due to a stable course of the disease,3 the second wave of the COVID‑19 pandemic, and unavailability of anti–SARS‑CoV‑2 vaccines, a decision to postpone treatment was made despite modest thrombocytopenia. Seven months later, the patient experienced recurrent bilateral edema of the lacrimal caruncle with an obstruction of lacrimal canaliculi. Another 4 months later, before commencing treatment, computed tomography (CT) was performed, revealing on chest high‑resolution CT (HRCT) bilateral ground‑glass opacities with intralobular septal thickening within the lower lobes, that is, a crazy paving pattern, suggesting a diagnosis of pulmonary proteinosis (Figure 1A and 1B). The bronchoalveolar lavage fluid (BALF) analysis did not confirm the diagnosis of proteinosis, on the contrary, the BALF culture was positive for Mycobacterium kansasii. Therapy with rifampin, isoniazid, and ethambutol was initiated. Despite negative cultures obtained after 3 and 6 months of treatment, there was a progression of the crazy paving pattern on chest HRCT scans. At that time a decision was made to perform a flow cytometry analysis of the BALF, which yielded a positive result for the presence of T‑PLL cells (Figure 1C–1E). The patient was started on intravenous alemtuzumab,4 which was associated with radiologic remission of the crazy paving pattern on chest HRCT performed after completion of treatment (Figure 1F and 1G). Based on the persistence of the T‑PLL cells in the BALF, and subsiding of T‑PLL at all other locations, the response to the first‑line treatment was assessed as a partial remission. As per available evidence,5 the response was consolidated with allogeneic hematopoietic stem cell transplantation. At the time of writing this report, the patient is in complete remission as assessed by routine procedures, with no signs of the crazy paving on chest HRCT scans and with full donor chimerism.
To summarize, the described patient presented with an unusual extramedullary involvement of the alveolar spaces in the course of T‑PLL. To the best of our knowledge, this is the first description of lung involvement, presenting as a diffuse infiltration of the alveolar spaces, and not a tumorous infiltration, typical of lymphomas.
- Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Lymphoid Neoplasms. Leukemia. 2022; 36: 1720‑1748.
- Staber PB, Herling M, Bellido M, et al. Consensus criteria for diagnosis, staging, and treatment response assessment of T‑cell prolymphocytic leukemia. Blood. 2019; 134: 1132‑1143. | Crossref
- Garand R, Goasguen J, Brizard A, et al. Indolent course as a relatively frequent presentation in T‑prolymphocytic leukaemia. Groupe Français d’Hématologie Cellulaire. Br J Haematol. 1998; 103: 488‑494. | Crossref
- Dearden CE, Khot A, Else M, et al. Alemtuzumab therapy in T‑cell prolymphocytic leukemia: comparing efficacy in a series treated intravenously and a study piloting the subcutaneous route. Blood. 2011; 118: 5799‑5802. | Crossref
- Wiktor‑Jedrzejczak W, Drozd‑Sokolowska J, Eikema DJ, et al. EBMT prospective observational study on allogeneic hematopoietic stem cell transplantation in T‑prolymphocytic leukemia (T‑PLL). Bone Marrow Transplant. 2019; 54: 1391‑1398. | Crossref
ARTICLE INFORMATION