Analysis of complications in transfemoral transcatheter aortic valve implantation: a single-center study
Key words: learning curve, transcatheter aortic valve implantation, transfemoral access, vascular closure devices

 CC BY 4.0
CC BY 4.0
Analysis of complications in transfemoral transcatheter aortic valve implantation: a single-center study
Introduction: Transfemoral access is a prevailing approach for transcatheter aortic valve implantation (TAVI) in contemporary practice, with a shift from surgical arteriotomy to a percutaneous arterial approach.
Objectives: This study assessed long- and short‑term mortality, along with Valve Academic Research Consortium‑2–defined complications in percutaneous transfemoral approach (PTA) TAVI. Furthermore, it explored the impact of a learning curve on procedural outcomes.
Patients and methods: The study included 600 patients undergoing PTA TAVI at the National Institute of Cardiology, Warsaw, Poland, from January 2009 to September 2020. Retrospective data comparison involved 2 groups: early experience (first 200 patients) and late experience (next 400 patients).
Results: The primary end point (composite of life‑threatening bleeding, major vascular complication, or death at 30 days) occurred less often in the late experience group (28% vs 17.5%; P = 0.003). The late experience group also showed fewer cases of vascular complications (19% vs 10.7%; P = 0.005) and major bleeding (17.5% vs 8.5%; P = 0.001). Propensity matching yielded similar trends, including reduced frequency of pacemaker implantation (22.8% vs 10.9%; P = 0.03) and shorter median (interquartile range) hospitalization (11 [8–18] vs 7 [6–12] days; P <0.001) in the late experience group.
Conclusions: The late experience group rated with PTA TAVI exhibited significantly reduced periprocedural complications, indicating a positive impact of accumulated expertise.
What's new?
Transcatheter aortic valve implantation (TAVI) is an established treatment method for patients with severe symptomatic aortic stenosis. Several access routes have been proposed, including the transaortic, transapical, transcarotid, subclavian, and the currently preferred and most widely used transfemoral approach. While surgical cutdown was the preferred femoral access strategy in early clinical TAVI experience, recent trends favor percutaneous transfemoral approach (PTA) procedures using vascular closure devices. In this retrospective single‑center study we present outcomes of 600 patients who underwent PTA TAVI, and assess the impact of a learning curve on the outcomes of the procedures. Our results confirmed safety and feasibility of this method, and showed a significant reduction in the number of procedural complications with experience.
Introduction
Since its introduction in 2002, transcatheter aortic valve implantation (TAVI) has become an established treatment option for severe symptomatic aortic stenosis (AS).1 During this period, several access routes have been proposed, such as transaortic, transapical, transcarotid, subclavian, and the currently preferred and most widely used transfemoral approach.2-4 Initially, surgical arteriotomy was required for femoral artery access and closure. This technique, however, has several disadvantages, including the need for general or spinal anesthesia, prolonged procedure time, delayed recovery, and increased risk of access‑site infections.5 Introduction of a complete percutaneous transfemoral approach (PTA) using different types of sutures and / or collagen‑based vascular closure devices established this access route as the access of choice, in line with the “minimalist” approach for TAVI.4
In our retrospective analysis, we aimed to evaluate long- and short‑term mortality and Valve Academic Research Consortium‑2 (VARC‑2)–defined complications in PTA TAVI procedures performed at our center, and to assess an impact of a learning curve and technologic progress on the outcomes of the procedures.
Patients and methods
Study population
Our retrospective, single‑center study was conducted at the National Institute of Cardiology (NIKARD), Warsaw, Poland.
All the patients who qualified for TAVI following a review by the institutional multidisciplinary Heart Team had severe symptomatic AS with aortic valve orifice area equal to or below 0.9 cm2. Surgical risk was assessed using the Society of Thoracic Surgeons and the European System for Cardiac Operative Risk Evaluation (logistic EuroSCORE and, since October 2011, EuroSCORE II) calculators.6-8 In their decision‑making process, the Heart Team also assessed other risk factors, not included in the abovementioned surgical risk scales, such as significant calcification of the ascending aorta, a history of chest radiotherapy, severe chest deformities, osteoporosis, active malignancy, or persistent anemia.
Between January 2009 and September 2020, 610 (82.8%) of a total of 736 TAVI procedures at the NIKARD were performed using the transfemoral approach, of which 600 (81.5%) were percutaneous procedures. All consecutive patients who underwent PTA TAVI in this period were retrospectively included in the analysis and divided into 2 groups: initial 200 patients (early group) comprising individuals undergoing TAVI from January 2009 to the beginning of May 2014, and subsequent 400 patients (late group) comprising individuals undergoing TAVI from May 2014 to September 2020. This division was based on the time of introduction of second‑generation bioprostheses, and similar reports assessing the learning curve on TAVI procedures.11-13
Preprocedural evaluation
All patients underwent pre‑TAVI transthoracic echocardiography (TTE) to quantify the severity of AS. Routine multislice computed tomography evaluation was performed during the qualification to assess calcium distribution in the aortic root, measure the aortic annulus and sinuses, and identify possible access routes. The vessel caliber was measured, and the iliofemoral anatomy was assessed by institutional radiologists to ensure feasibility of the percutaneous transfemoral TAVI system delivery.
Procedural details
Between 2009 and 2020, our team adopted Core Valve / EvolutR self‑expandable systems (Medtronic, Minneapolis, Minnesota, United States), Sapien XT/3 balloon‑expandable systems (Edwards Lifesciences, Irvine, California, United States), self‑expandable Accurate Neo systems (Symetis / Boston Scientific, Marlborough, Massachusetts, Unites States), mechanically expanded Lotus systems (Boston Scientific), self‑expandable Portico systems (Abbott Vascular, Redwood City, California, United States), and balloon‑expandable MyVal systems (Meril Life Sciences Pvt. Ltd., Vapi, Gujarat, India) for PTA TAVI.
At NIKARD, transfemoral TAVI was mostly performed via PTA. In selected cases featuring severe obesity, plaque calcification, or severe kinking and tortuosity of the femoral arteries, access was obtained by surgical incision. The choice between surgical cutdown and PTA was made by the institutional Heart Team.
Different types of vascular closure devices were used for arterial access management in PTA TAVI procedures: suture‑based, including the Prostar XL percutaneous vascular surgical system and the ProGlide suture‑mediated closure system (both Abbott Vascular), or collagen‑based, including the Manta vascular closure device (Teleflex, Morrisville, North Carolina, United States), and the Angio‑Seal VIP vascular closure device (Abbott Vascular). Protamine sulfate was administered after the valve deployment to reverse unfractionated heparin.
The effectiveness of each procedure was assessed immediately by TTE. Additional TTE examinations were performed on the day of discharge and during follow‑up visits on day 30, 180, and 360, and then annually.
Data acquisition and end points
Baseline data, procedural characteristics, and outcomes of all patients accepted for TAVI at NIKARD were prospectively collected in a local database and additionally, since January 2013, in the Pol‑TAVI national registry.9
The primary end point of the study was the composite of life‑threatening bleeding, major vascular complications, or death at 30 days. Secondary end points encompassed all‑cause mortality at 30, 90, 275, and 540 days, as well as procedure failure or access site–related vascular and bleeding complications, assessed in accordance with the VARC‑2 definition / criteria10 (comprehensive definitions are presented in Supplementary material).
Clinical and echocardiographic follow‑up data were gathered either during in‑person visits or via telephone interviews if the in‑person visit was not feasible. For the collection and verification of mortality data, we relied on the Polish personal identification number database, a national registry that was cross‑checked with the electronic beneficiary entitlement verification system for additional validation.
Out of 574 patients, 560 (97.6%) were available for the 30‑day follow‑up, and 472 of 520 (90.8%) for the 1‑year follow‑up. Complete follow‑up data regarding mortality at 30, 90, 275, and 540 days were successfully obtained. The mean (SD) survival follow‑up was 1293.8 (750.35) days, with a median (interquartile range [IQR]) of 1280.5 days (677–1560).
Due to a retrospective design of the study, patient consent and ethical approval were not required.
Statistical analysis
Data normality was assessed with the Kolmogorov–Smirnov test. Results for continuous variables are presented as means and SD (normal distribution) or median and IQR (non‑normal distribution), and were compared with the t test or the Wilcoxon test, as appropriate. Categorical variables are reported as counts and percentages, and were compared with the χ2 test or the Fisher exact test. Propensity‑score matching with the nearest neighbor method was used to adjust for baseline differences between the groups. In the sensitivity analysis, we matched the patients according to the variables significant in univariable analyses and those considered clinically relevant. Validity of logistic regression was assessed with the Hosmer–Lemeshow goodness‑of‑fit test. Survival curves were constructed using the Kaplan–Meier estimator, and the 2 study groups were compared with the log‑rank tests.
Multivariable Cox proportional hazards regression for mortality and multivariable logistic regression for composite periprocedural complications were used with a stepwise selection procedure. Mandatory variables retained in the final model included age, sex, and group timing (late vs early). The proportional hazards assumption was met.
All hypotheses were 2‑tailed with a 0.05 type I error. P values below 0.05 were deemed significant. All statistical analyses were performed using the SAS statistical software, version 9.4 (SAS Institute, Cary, North Carolina, United States).
Results
Baseline characteristics
The baseline, clinical, and procedural characteristics and the early and late experience groups are presented in Tables 1 and 2. The median (IQR) age of the study population was 82 (77–85) years with the median EuroSCORE II of 4.15% (2.73%–6.15%). Median body mass index was 26.6 (24–30.1) kg/m2 with 37.5% (n = 224) diabetes mellitus prevalence. The mean (SD) renal function assessed by estimated glomerular filtration rate (eGFR) was 54.8 (16.9) ml/min/1.73 m2, and median of the mean aortic gradient was 49 (39–61) mm Hg.
Parameter | Total (n = 600) | Early experience (n = 200) | Late experience (n = 400) | P value |
Data are presented as mean (SD) or median (interquartile range) unless stated otherwise.
Abbreviations: BMI, body mass index; CABG, coronary artery bypass grafting; EuroSCORE, European System for Cardiac Operative Risk Evaluation; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; TAVI, transcatheter aortic valve implantation; TIA, transient ischemic attack | ||||
Baseline characteristics | ||||
Age, y | 82 (77–85) | 81.5 (77–85) | 82 (76–86) | 0.98 |
BMI, kg/m2 | 26.6 (24–30.1) | 26.8 (24.1–29.9) | 26.4 (24.4–28.7) | 0.62 |
Men, n (%) | 239 (39.8) | 62 (31) | 177 (44.2) | 0.002 |
Diabetes mellitus, n (%) | 224 (37.5) | 73 (36.5) | 151 (38) | 0.72 |
Previous myocardial infarction, n (%) | 123 (20.5) | 42 (21) | 81 (20.3) | 0.84 |
Chronic obstructive pulmonary disease, n (%) | 97 (16.2) | 41 (20.5) | 56 (14) | 0.04 |
Previous stroke or TIA, n (%) | 72 (12) | 28 (14) | 44 (11) | 0.29 |
Previous PCI, n (%) | 168 (28) | 48 (24) | 120 (30.1) | 0.12 |
Previous CABG, n (%) | 67 (11.2) | 28 (14) | 39 (9.8) | 0.12 |
Atrial fibrillation, n (%) | 211 (35.3) | 55 (27.5) | 156 (39.3) | 0.004 |
Previously implanted pacemaker, n (%) | 91 (15.2) | 35 (17.5) | 56 (14) | 0.26 |
Creatinine clearance, ml/min | 54.8 (16.9) | 57.3 (17.8) | 53.5 (16.2) | 0.009 |
EuroSCORE II, % | 4.15 (2.73–6.15) | 3.78 (2.7–5.81) | 4.23 (2.76–6.25) | 0.47 |
Bicuspid aortic valve, n (%) | 53 (8.8) | 13 (6.5) | 40 (10) | 0.15 |
Echocardiographic data | ||||
LVEF, % | 60 (50–65) | 60 (50–65) | 60 (50–65) | 0.88 |
Aortic valve area calculated using the continuity equation prior to TAVI, cm2 | 0.65 (0.16) | 0.64 (0.14) | 0.65 (0.17) | 0.79 |
Maximum aortic gradient, mm Hg | 82 (68–98) | 90 (75.2–104.5) | 79 (64–93) | <0.001 |
Mean aortic gradient, mm Hg | 49 (39–61) | 52 (43–66) | 47 (37–55) | 0.007 |
Parameter | Early experience (n = 92) | Late experience (n = 92) | P value |
Data are presented as mean (SD) or median (interquartile range) unless stated otherwise.
Abbreviations: see Table 1 | |||
Propensity score | 0.4084 (0.2309) | 0.4082 (0.2308) | 0.99 |
Baseline characteristics | |||
Men, n (%) | 27 (29.3) | 30 (32.6) | 0.63 |
Age, y | 82.0 (77–86) | 81.5 (76–85.5) | 0.65 |
BMI, kg/m2 | 26.9 (24.2–29.4) | 26.4 (24.2–29.9) | 0.68 |
Diabetes mellitus, n (%) | 37 (33.7) | 36 (39.1) | 0.44 |
Previous myocardial infarction, n (%) | 15 (16.3) | 14 (15.2) | 0.84 |
Chronic obstructive pulmonary disease, n (%) | 17 (18.5) | 15 (16.3) | 0.7 |
Previous stroke or TIA, n (%) | 12 (13) | 14 (15.2) | 0.67 |
Previous PCI, n (%) | 25 (27.2) | 21 (22.8) | 0.5 |
Previous CABG, n (%) | 10 (10.9) | 13 (14.1) | 0.5 |
Atrial fibrillation, n (%) | 25 (27.2) | 28 (30.4) | 0.63 |
Previously implanted pacemaker, n (%) | 14 (15.2) | 14 (15.2) | 1 |
Creatinine clearance, ml/min | 56.8 (16.7) | 58.0 (17.8) | 0.65 |
EuroSCORE II, % | 3.93 (2.68–5.71) | 4.24 (2.73–6.29) | 0.69 |
Echocardiographic data | |||
LVEF prior to TAVI, % | 60 (50–65) | 60 (51–65) | 0.94 |
Bicuspid aortic valve, n (%) | 7 (7.6) | 10 (10.9) | 0.45 |
Aortic valve area calculated using the continuity equation, cm2 | 0.64 (0.14) | 0.65 (0.16) | 0.8 |
Maximum aortic gradient, mm Hg | 90 (75.7–100) | 86.5 (77.5–106) | 0.78 |
Mean aortic gradient, mm Hg | 55.2 (46–70) |
| 0.31 |
The early experience group patients had better renal function (mean eGFR, 57.3 [17.8] vs 53.5 [16.2] ml/min/1.73 m2; P = 0.009) and higher maximum and mean aortic gradients at baseline. There were no significant differences in terms of mean EuroSCORE II between the groups.
Procedural characteristics
Details of the procedure and the results are presented in Tables 3 and 4.
Parameter | Total (n = 600) | Early experience (n = 200) | Late experience (n = 400) | P value |
Data are presented as mean (SD) or median (interquartile range) unless stated otherwise.
Abbreviations: see Table 1 | ||||
Procedural characteristics | ||||
Local anesthesia, n (%) | 336 (56) | 54 (27) | 282 (71.4) | <0.001 |
Fluoroscopy time, min | 28.4 (22.2–37) | 30.2 (24.5–38) | 28 (21.5–36.5) | 0.02 |
Total volume of contrast used, ml | 200 (150–200) | 180 (150–200) | 200 (150–200) | 0.31 |
Self‑expandable valves, n (%) | 374 (62.4) | 112 (56) | 262 (65.7) | 0.02 |
Postprocedural characteristics | ||||
Creatinine clearance, ml/min | 60.2 (21.3) | 64.5 (21.9) | 58.4 (20.8) | 0.002 |
Maximum aortic gradient, mm Hg | 16 (12–22) | 17 (12.4–23) | 16 (12–22) | 0.06 |
Mean aortic gradient, mm Hg | 8 (7–14) | 10 (7–14) | 8.4 (6–12) | 0.002 |
Length of hospitalization, d | 8 (7–14) | 11 (8–16) | 8 (6–12) | <0.001 |
Major vascular complications, n (%) | 26 (4.3) | 8 (4) | 18 (4.5) | 0.78 |
Minor vascular complications, n (%) | 56 (9.3) | 30 (15) | 26 (6.5) | <0.001 |
Life‑threatening bleeding, n (%) | 19 (3.2) | 9 (4.5) | 10 (2.5) | 0.19 |
Major bleeding, n (%) | 69 (11.5) | 35 (17.5) | 34 (8.5) | 0.001 |
Minor bleeding, n (%) | 66 (11) | 16 (8) | 50 (12.5) | 0.1 |
Myocardial infarction up to 72 hours after the procedure, n (%) | 5 (0.8) | 2 (1) | 3 (0.75) | >0.99 |
Stroke / TIA up to 72 hours after the procedure, n (%) | 11 (1.8) | 4 (2) | 7 (1.7) | >0.99 |
Coronary occlusion during the procedure, n (%) | 5 (0.8) | 2 (1) | 3 (0.7) | >0.99 |
Annulus rupture, n (%) | 3 (0.5) | 3 (1.5) | 0 | 0.04 |
New pacemaker, n (%) | 89 (14.8) | 50 (25) | 39 (9.7) | <0.001 |
Moderate‑to‑severe aortic regurgitation after the procedure, n (%) | 93 (15.5) | 40 (20) | 53 (13.2) | 0.03 |
Composite end points | ||||
Any vascular complication (major or minor vascular complications), n (%) | 81 (13.5) | 38 (19) | 43 (10.7) | 0.005 |
Life‑threatening bleeding, major vascular complication, or death at 30 days, n (%) | 126 (21) | 56 (28) | 70 (17.5) | 0.003 |
Mortality rate, % (95% CI) | ||||
30‑day | 4.3 (2.7–5.9) [n = 26] | 5 (2.1–7.9) [n = 10] | 4 (2–6) [n = 16] | 0.57 |
90‑day | 7 (5–9) [n = 42] | 8 (4.3–11.7) [n = 16] | 6.5 (4.2–8.9) [n = 26] | 0.5 |
275‑day | 11 (8.4–13.5) [n = 66] | 13 (8.3–17.7) [n = 26] | 10 (7.1–12.9) [n = 40] | 0.27 |
365‑day | 14.5 (11.7–17.3) [n = 84] | 15.0 (11–19.9) [n = 31] | 14.2 (10.8–17.6) [n = 57] | 0.81 |
540‑day | 18.7 (15.6–21.8) [n = 112] | 20.5 (14.8–26.2) [n = 41] | 17.7 (14–21.4) [n = 71] | 0.42 |
Cardiac mortality rate, % (95% CI) | ||||
30‑day | 4.3 (2.7–5.9) [n = 26] | 5 (2.1–7.9) [n = 10] | 4 (2–6) [n = 16] | 0.57 |
90‑day | 6.3 (5–9) [n = 38] | 7.5 (3.8–11.2) [n = 15] | 5.7 (3.4–8) [n = 23] | 0.41 |
275‑day | 8.7 (8.4–13.5) [n = 52] | 11 (6.7–15.3) [n = 22] | 7.5 (4.9–10) [n = 30] | 0.15 |
365‑day | 10.6 (8.1–13.1) [n = 63] | 13 (8.3–17.7) [n = 26] | 9 (6.1–11.9) [n = 37] | 0.16 |
540‑day | 13.2 (15.6–21.8) [n = 79] | 18 (13.3–22.7) [n = 36] | 10.7 (7.6–13.8) [n = 43] | 0.01 |
Parameter | Early experience (n = 92) | Late experience (n = 92) | P value |
Abbreviations: see Table 1 | |||
Procedural characteristics | |||
General anesthesia, n (%) | 64 (70.3) | 24 (26.1) | <0.001 |
Fluoroscopy time, min | 27.8 (22.5–34.6) | 28.3 (23–38) | 0.49 |
Postprocedural characteristics | |||
Creatinine clearance, ml/min | 64.8 (21.6) | 61.7 (22.9) | 0.38 |
Maximum aortic gradient, mm Hg | 18 (14–25) | 16 (12–22) | 0.09 |
Mean aortic gradient, mm Hg | 10.5 (6.9–15) | 8.7 (6.3–12.5) | 0.03 |
Length of hospitalization, d | 11 (8–18) | 7 (6–12) | <0.001 |
Major vascular complications, n (%) | 6 (6.5) | 7 (7.6) | 0.77 |
Minor vascular complications, n (%) | 9 (9.8) | 4 (4.3) | 0.15 |
Life‑threatening bleeding, n (%) | 4 (4.3) | 2 (1.1) | 0.37 |
Major bleeding, n (%) | 18 (19.6) | 12 (13) | 0.23 |
Minor bleeding, n (%) | 7 (7.6) | 8 (8.7) | 0.79 |
Myocardial infarction up to 72 hours after the procedure, n (%) | 2 (2.2) | 0 | 0.5 |
Stroke / TIA up to 72 hours after the procedure, n (%) | 2 (2.2) | 2 (2.2) | 1 |
Coronary occlusion during the procedure, n (%) | 2 (2.2) | 0 | 0.5 |
Annulus rupture, n (%) | 2 (2.2) | 0 | 0.5 |
New pacemaker implantation after the procedure, n (%) | 21 (22.8) | 10 (10.9) | 0.03 |
Moderate‑to‑severe aortic insufficiency after the procedure, n (%) | 15 (16.3) | 15 (16.3) | 1 |
Composite end points | |||
Any vascular complication (major or minor vascular complications), n (%) | 15 (16.3) | 10 (10.9) | 0.28 |
Life‑threatening bleeding, major vascular complication, or death at 30 days, n (%) | 29 (31.5) | 17 (18.5) | 0.04 |
Mortality rate, % (95% CI) | |||
30‑day | 6.5 (1.4–11.6) [n = 6] | 1.1 (0–3.3) [n = 1] | 0.12 |
90‑day | 10.9 (4.6–17.2) [n = 10] | 6.5 (1.4–11.6) [n = 6] | 0.3 |
275‑day | 16.3 (8.8–23.7) [n = 15] | 12 (5.3–18.7) [n = 11] | 0.4 |
365‑day | 16.3 (8.8–23.7)
[n = 15] | 17.4 (9.7–25.1)
[n = 16] | 0.88 |
540‑day | 21.7 (13.3–30.1) [n = 20] | 20.6 (12.4–28.8) [n = 19] | 0.86 |
Cardiac mortality rate, % (95% CI) | |||
30‑day | 6.5 (1.4–11.6) [n = 6] | 1.1 (0–3.3) [n = 1] | 0.12 |
90‑day | 9.8 (3.7–15.9) [n = 9] | 6.5 (1.4–11.6) [n = 6] | 0.42 |
275‑day | 12 (5.3–18.7) [n = 11] | 9.8 (3.7–15.9) [n = 9] | 0.64 |
365‑day | 12 (5.3–18.7)
[n = 11] | 14.1 (6.8–21.2)
[n = 13] | 0.66 |
540‑day | 16.6 (9–24.2) [n = 15] | 14.3 (7–21.5) [n = 13] | 0.68 |
Increased use of local anesthesia was observed (27% in the early group vs 71.4% in the late group; P <0.001). Self‑expandable valves were more often used in the late group (56% vs 65.7%; P = 0.02).
Access‑related vascular and bleeding complications
Data regarding access‑related vascular and bleeding complications, assessed according to the VARC‑2 definitions, are outlined in Tables 3 and 4. In our cohort, serious vascular complications occurred in 26 cases (4.3%), while minor vascular complications were observed in 56 cases (9.3%). Notably, there were fewer minor vascular complications in the late group (15% vs 6.5%; P = 0.001), and a general reduction in vascular complications (19% vs 10.7%; P = 0.005), with no significant difference in the rate of major vascular complications (4% vs 4.5%; P = 0.78) were noted.
Furthermore, major bleeding complications were less prevalent in the late group (17.5% vs 8.5%; P = 0.001). However, there was no significant difference between these groups concerning life‑threatening or minor bleeding events (Tables 3 and 4).
In‑hospital mortality
Overall, in‑hospital death occurred in 15 patients (2.5%), with 6 cases (1%) attributed to ventricular arrhythmia and sudden cardiac arrest nonresponsive to resuscitation. Among these, 2 patients died periprocedurally and 4 within 2–6 days after the procedure. Additionally, 2 patients (0.33%) died due to aortic dissection, 2 to retroperitoneal hematoma, 2 to periprocedural myocardial infarction, 2 to cardiac tamponade, and 1 (0.16%) to aortic rupture.
Short- and long‑term follow‑up
Follow‑up data are presented in Tables 3 and 4.
The study primary end point, that is, the composite of life‑threatening bleeding, major vascular complications, or death at 30 days was less frequent in the late group (28% vs 17.5%; P = 0.003).
There was no significant difference in the occurrence of periprocedural stroke, myocardial infarction, or coronary occlusion between the groups (Tables 3 and 4). The need for pacemaker implantation prior to discharge occurred in 89 (14.8%) patients, and was lower in the late group (25% vs 9.7%; P <0.001).
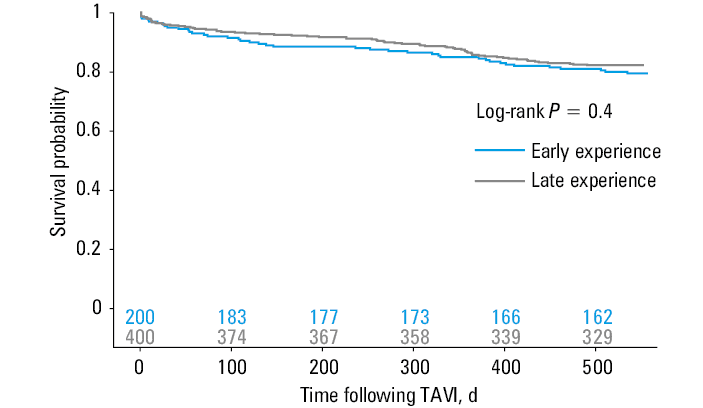
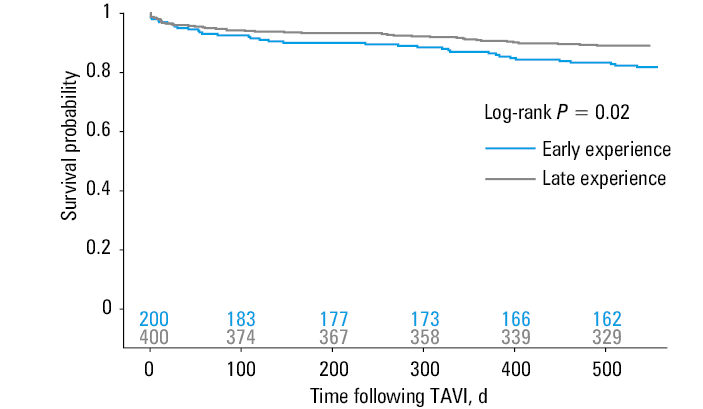
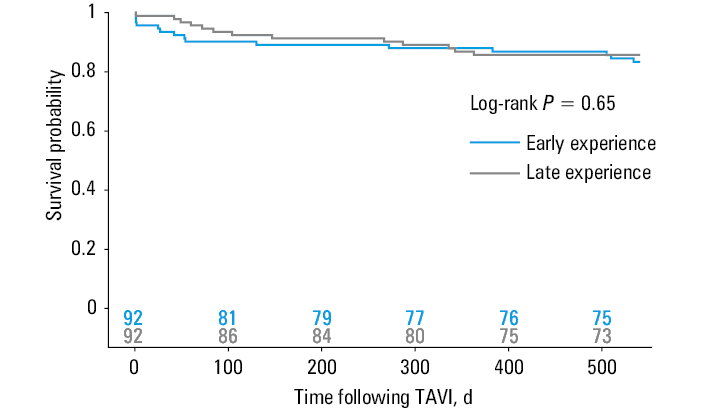
The median length of hospital stay decreased with the increasing experience of the operators from 11 (8–16) days to 8 (6–12) days (P <0.001). The 540‑day mortality was higher in the early group (18% vs 10.7%; P = 0.01). The Kaplan–Meier curves for all‑cause and cardiac mortality at 540 days are presented in Figure 1 and Figure 2.
Abbreviations: see Table 1
Abbreviations: see Table 1
Baseline characteristics, procedural characteristics, and outcomes after propensity matching
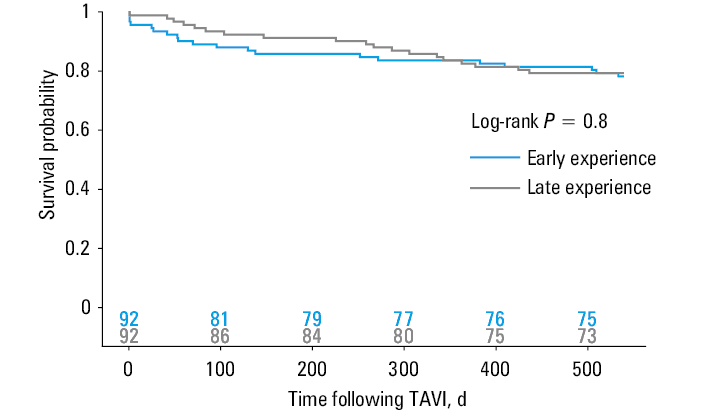
The groups were analyzed using a propensity matched model with 92 pairs of patients. The model was well calibrated (χ2 = 9.81; degrees of freedom = 8; P = 0.28). The propensity model yielded a concordance index of 0.832 (95% CI, 0.799–0.865). Standardized differences before and after propensity score matching are presented in Figure 3. The baseline characteristics of the matched groups are summarized in Tables 1 and 2. Procedural and outcome data stratified by experience after propensity score matching are presented in Tables 3 and 4. The primary end point of composite of life‑threatening bleeding, major vascular complications, or death at 30 days was less frequent in the late experience group (31.5% vs 8.5%; P = 0.04). The percentage of procedures performed under local anesthesia was higher (26.15% vs 70.3%; P <0.001), with a less frequent need for pacemaker implantation (22.8% vs 10.9%; P = 0.03) and shorter hospitalization (11 [8–18] vs 7 [6–12] days; P <0.001) in the late experience group. No significant difference in 30-, 90-, 275-, 365-, or 540‑day all‑cause mortality or cardiac mortality was shown between the 2 groups. The Kaplan–Meier curves for all‑cause and cardiac mortality at 540 days after propensity matching are presented in Figure 4 and Figure 5.
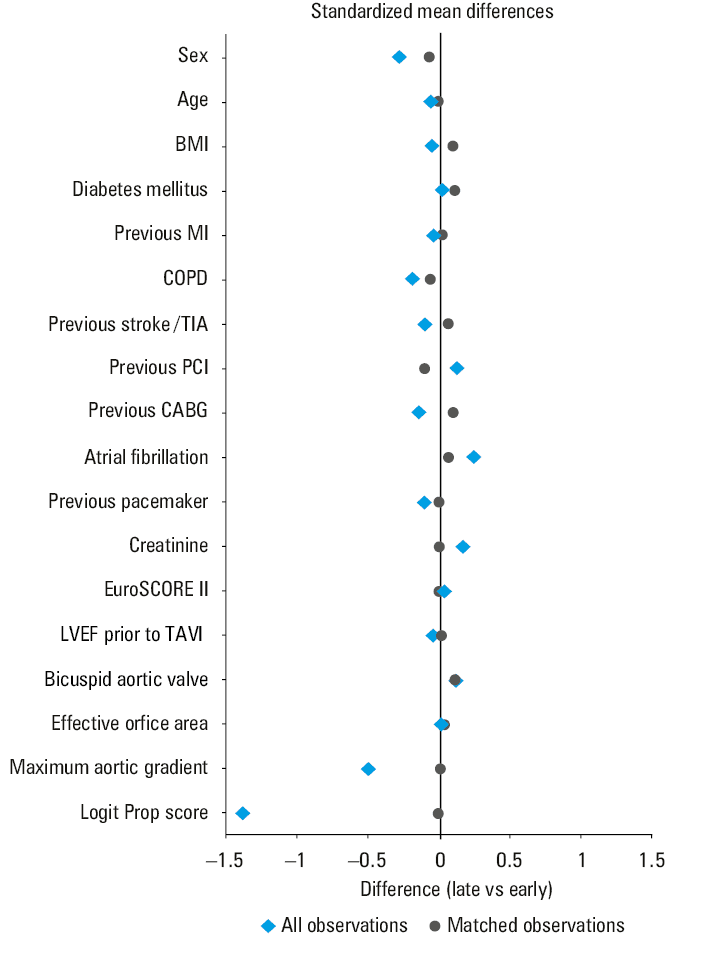
Abbreviations: COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; others, see Table 1
Abbreviations: see Table 1
Abbreviations: see Table 1
Analysis of risk factors for mortality and complications
Further multivariable analysis was conducted to determine the factors influencing mortality and the occurrence of composite end points, as detailed in Supplementary material, Tables S1 and S2. The Cox proportional hazards regression identified no significant predictors of all‑cause death when considering sex, age, and early vs late group. However, chronic obstructive pulmonary disease (hazard ratio [HR], 1.597; 95% CI, 1.013–2.517; P = 0.04) and creatinine clearance (HR, 1.421; 95% CI, 1.038–1.944; P = 0.03) were associated with a higher risk. For cardiac death, being in the late group was associated with a reduced risk (HR, 0.511; 95% CI, 0.323–0.807; P = 0.004), and creatinine clearance remained a significant predictor (HR, 1.469; 95% CI, 1.304–2.088; P = 0.03).
Risk assessment of composite end points through multivariable logistic regression demonstrated a lower risk in the late group for any vascular complication (odds ratio [OR], 0.459; 95% CI, 0.281–0.751; P = 0.002) and for the composite end point of life‑threatening bleeding, major vascular complications, or death at 30 days (OR, 0.48; 95% CI, 0.314–0.733; P <0.001). Elevated creatinine clearance was associated with an increased risk (OR, 1.847; 95% CI, 1.251–2.726; P = 0.002), and a smaller aortic valve area calculated using the continuity equation prior to TAVI was a protective factor (OR, 0.244; 95% CI, 0.059–0.998; P = 0.05).
Discussion
To our knowledge, this is the largest Polish single‑center study comprising patients who underwent PTA TAVI.
The predominant approach for TAVI, both percutaneous and surgical, is currently transfemoral, as indicated by the European Society of Cardiology guidelines, emphasizing its suitability, especially in elderly patients.2-4,14 In alignment with global trends, Polish TAVI centers have witnessed a steady rise in transfemoral procedures, reaching 93.5% by 2020.3,15
While surgical cutdown was the preferred femoral access strategy in early clinical experience, recent trends favor PTA procedures with local anesthesia and optionally under conscious sedation. Technologic advances of PTA TAVI systems, optimization of treatment pathways, and operator experience allow for a timely patient discharge with minimized risk of adverse events.16
In light of the current lack of conclusive evidence establishing clear superiority of percutaneous vs surgical cutdown approaches in TAVI,17-20 the choice of access should be tailored to the patient’s clinical characteristics and the center’s experience. At our institution, the use of the surgical method is infrequent and typically guided by factors such as extreme obesity or specific anatomic features, including marked tortuosity or significant calcifications at the potential puncture site of the femoral artery. Given the considerably smaller number of patients undergoing transfemoral TAVI with surgical arteriotomy as compared with PTA, we did not aim to compare the results between these 2 groups.
Over the 2 decades of continuous development in TAVI, the procedure evolved far beyond optimization of the preferred access site.
One of the notable advances observed over time in TAVI practice involves a reduction in the incidence of access site–related and bleeding complications. Numerous studies have validated a significant decrease in vascular complications associated with increased procedural experience.11 For example, Hayashida et al12 demonstrated a noteworthy reduction in the incidence of both any vascular complications (11.4% vs 28.6%; P = 0.012) and major complications (2.9% vs 14.3%; P = 0.018) in complete percutaneous TAVI procedures with improved center experience, incorporating the use of novel closure devices.12
In parallel with these findings, our cohort exhibited a significantly reduced incidence of minor vascular and major bleeding complications when stratified by experience levels. The late experience group demonstrated a significantly lower risk of any vascular complications. This reduction is of particular significance given that major vascular complications are recognized contributors to increased mortality, higher incidence of renal impairment, prolonged hospitalization, and diminished quality of life.19,21 Integration of novel closure devices and increased procedural experience are likely the key factors contributing to these improved outcomes.
Another aspect related to TAVI vascular access is utilization of protamine sulfate. Notably, in our center, consistent incorporation of protamine sulfate during TAVI was observed. Nonetheless, the precise impact of protamine sulfate administration on the incidence of access site–related complications remains uncertain. As illustrated by Zbroński et al,22 other studies do not demonstrate a significant decrease in bleeding complications, emphasizing the pressing need for further research in this field.
In addition to the noteworthy advances related to the access site and reduced bleeding rates, our study highlights another positive trend, that is, a substantial decrease in the number of procedures conducted under general anesthesia, a shortened length of hospital stay, and a diminished need for pacemaker implantation within the late experience group. This positive trajectory was evident in both unmatched and propensity‑matched groups, underscoring sustained improvement in procedural efficiency and patient outcomes over time. In our institution, 56.5% of all PTA TAVI procedures were performed under local anesthesia, and similarly to other reports17-19 we observed significantly fewer procedures under general anesthesia over time (27% of procedures under local anesthesia in the early experience group vs 71.4% in the late experience group). While current literature indicates that opting for TAVI under local anesthesia, as opposed to general anesthesia, does not exert a discernible impact on cardiac or all‑cause mortality, it significantly contributes to procedural efficiency. Specifically, this approach results in shortened total procedure time, reduced intervention time, and decreased costs. Additionally, local anesthesia facilitates earlier patient mobilization. These advantages hold particular significance in the context of typical demographic features of a TAVI patient, characterized by frailty and advanced age.23,25,26 Shortening the hospital stay and decreasing the need for pacemaker implantation are further trends reflecting advances in TAVI procedures and device selection. As shown by Nakamura et al,18 these not only reduce the procedural and postprocedural financial burden of TAVI, but also minimize invasiveness of the procedures reflecting best practices in modern medicine. It should also be noted that the prevalence of more than mild paravalvular leak in the unmatched analysis was reduced in the late experience group, which is in line with previous reports assessing the impact of the learning curve on TAVI.18,20
These benefits may be related not only to the learning curve per se but also to technologic progress in TAVI systems and devices, mastering the qualification process, proper device selection, and increasing technical skills, resulting in optimal procedure outcomes.
These positive trends will become increasingly relevant in a landscape marked by a growing number of structural transcatheter procedures and broadening eligibility criteria for TAVI in younger patient groups. As TAVI continues to evolve, these favorable developments play a crucial role in shaping the landscape of cardiovascular interventions, emphasizing their practical significance in diverse patient populations.
Limitations
The data included in our analysis are retrospective and limited to a single center, and therefore our conclusions should be confirmed in further studies.
As mentioned, we did not aim to compare the results between the PTA and surgical TAVI procedures due to a lack of extensive experience in the latter.
Regarding follow‑up, a majority of our cohort, that is, 97.6% (560 out of 574) and 90.8% (472 out of 520) were available for the 1‑month and 1‑year follow‑ups, respectively. While these rates are comparatively high, they are not comprehensive. The absence of complete follow‑up introduces a potential for selection bias.
Conclusions
Over the past 2 decades, the evolution of operator proficiency, alongside with technologic enhancements in TAVI systems, refined treatment pathways, and adoption of advanced closure devices have substantially reduced the rate of periprocedural complications, affirming the enhanced safety of TAVI. While PTA TAVI is now characterized by a lower risk of periprocedural and mid‑term complications, our propensity score matching analysis indicates that these safety improvements have not been accompanied by a significant reduction in long‑term mortality rates. This finding underscores the importance of continuous improvement and monitoring in TAVI practices to translate procedural safety gains into longer‑term survival benefits.
- Leon MB, Smith CR, Mack M, et al. Transcatheter aortic‑valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010; 363: 1597‑1607. | Crossref
- Parma R, Zembala MO, Dąbrowski M, et al. Transcatheter aortic valve implantation. Expert consensus of the Association of Cardiovascular Interventions of the Polish Cardiac Society and the Polish Society of Cardio‑Thoracic Surgeons, approved by the Board of the Polish Cardiac Society. Kardiol Pol. 2017; 75: 937‑964. | Crossref
- Dąbrowski M, Parma R, Huczek Z, et al. The Polish Interventional Cardiology TAVI Survey (PICTS): 10 years of transcatheter aortic valve implantation in Poland. The landscape after the first stage of the Valve for Life Initiative. Pol Arch Intern Med. 2021; 131: 413‑420. | Crossref
- Hecker F, Arsalan M, Kim WK, Walther T. Transcatheter aortic valve implantation (TAVI) in 2018: recent advances and future development. Minerva Cardioangiol. 2018; 66: 314‑328. | Crossref
- Durmuş G, Belen E, Bayyiğit A, Can MM. Comparison of complication and success rates of ProGlide closure device in patients undergoing TAVI and endovascular aneurysm repair. Biomed Res Int. 2018; 2018: 2687862. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION