Tuberculosis is an infectious opportunistic bacterial disease caused by Mycobacterium species. In transplant recipients, it can manifest as a result of latent infection reactivation, failure to diagnose infection in the allograft, or a new post‑transplantation infection.1 Solid organ transplant recipients are particularly vulnerable to a severe course of the disease, with elevated mortality rates.1-3 Pulmonary tuberculosis is the most common form of post‑transplant tuberculosis (47.6%–60%).1,3 However, tuberculosis of a transplanted kidney is extremely rare, with only a limited number of reported cases.
Involvement of the urinary system can present with various manifestations, including caseous, parenchymal, potentially necrotizing tubercles, interstitial nephritis, ureteral fibrosis, and sterile cystitis. In certain instances, the disease may be oligo- or asymptomatic, with sterile pyuria or microhematuria incidentally detected in urinalysis.2-4
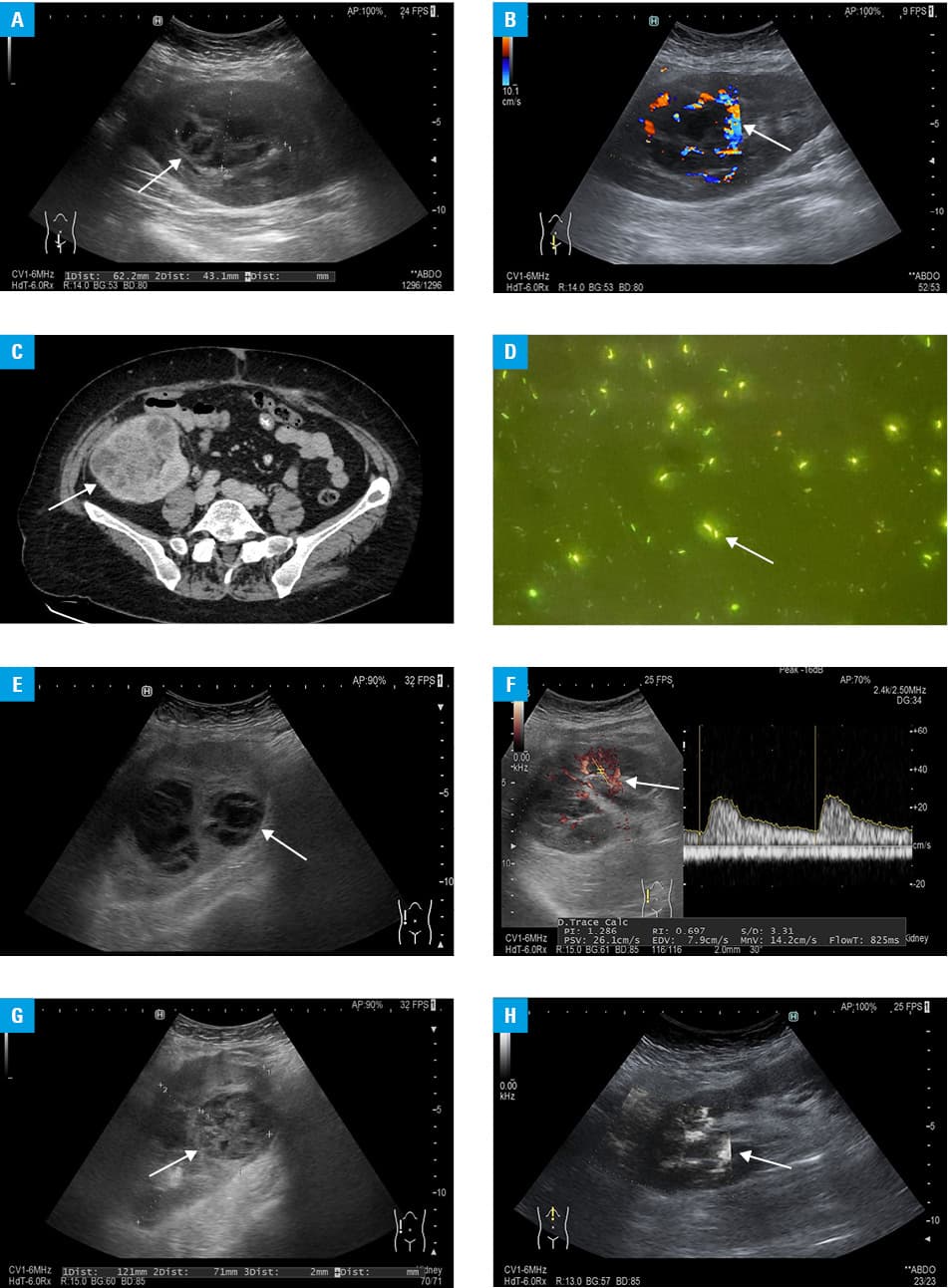
A 66‑year‑old woman, who underwent kidney transplantation from a deceased unrelated donor 9 months earlier, with end‑stage chronic kidney disease due to hypertensive nephropathy, was admitted to a hospital due to recurrent fever with shivering. The patient initially developed similar symptoms 1 month post‑transplantation and received several courses of antimicrobial treatment, which temporarily alleviated the symptoms, but subsequent relapses occurred. Abdominal ultrasound revealed a lesion on the kidney graft, comprising solid and fluid‑filled components (Figure 1A), with hypervascularization observed in the peripheral part (Figure 1B). Computed tomography confirmed nonhomogeneous masses corresponding to abscesses (Figure 1C). The patient underwent ultrasound‑guided percutaneous puncture and drainage of the lesions. Microbiologic testing identified acid‑fast bacilli in the collected material (Figure 1D), leading to a diagnosis of renal tuberculosis. Treatment with 4 tuberculostatic agents (rifampin, isoniazid, pyrazinamide, and ethambutol) resulted in rapid clinical improvement within a few days. The patient’s immunosuppressive regimen was adjusted by discontinuing mycophenolate mofetil while maintaining prednisone and tacrolimus (target levels, 5–7 ng/ml). Follow‑up examinations showed regression of the lesion on abdominal ultrasound (Figure 1E) with improved blood flow in the affected area (Figure 1F). Due to persistent focal lesions in the transplanted kidney found during the follow‑up ultrasound examinations (Figure 1G), antituberculosis treatment was continued for 2 years, resulting in a complete regression of the lesion and normalization of intrarenal blood flow (Figure 1H). Over this period, there were no episodes of tuberculosis recurrence and the transplanted kidney function remained stable, without signs of rejection.
In this particular case, transmission through the donated kidney was deemed the most likely source of tuberculosis, given the localized involvement of the transplanted kidney and the concurrent diagnosis of pulmonary tuberculosis in another kidney recipient from the same cadaveric donor. Nonetheless, confirming this hypothesis is technically unfeasible.
Mycobacterium tuberculosis infection can lead to sporadic abscess formation in the kidney graft.4 It is crucial to consider renal tuberculosis in a differential diagnosis of transplant recipients presenting with fever of unknown origin, pyuria, and abdominal pain. Early initiation of tuberculostatic regimens improves the chances of recovery.1,4,5 Due to potential toxicity and drug interactions of antituberculosis agents with immunosuppressants, individual dose adjustments of these medications and extended antituberculosis therapy are essential.1,4,5
- Sorohan BM, Ismail G, Tacu D, et al. Mycobacterium tuberculosis infection after kidney transplantation: a comprehensive review. Pathog Basel Switz. 2022; 11: 1041. | Crossref
- Toccaceli S, Persico Stella L, Diana M, et al. Renal tuberculosis: a case report. G Chir. 2015; 36: 76‑78. | Crossref
- Alizadeh AM, Marjani M, Moniri A, et al. Tuberculosis in solid organ transplantation. Tanaffos. 2016; 15: 124‑127.
- Sasi S, Varghese MK, Nair AP, et al. Tuberculosis in an allogeneic transplant kidney: a rare case report and review of literature. Cureus. 2020; 12: e11661. | Crossref
- Clemente WT, Faria LC, Cota GF, et al. Donor‑derived tuberculosis: a case report and the role of communication gaps in transplantation safety. Case Rep Transplant. 2021; 2021: 8816426. | Crossref
ARTICLE INFORMATION