Patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension during the COVID-19 pandemic (2020–2022): clinical outcomes, prognostic factors, and response to vaccination

 CC BY 4.0
CC BY 4.0
Patients with pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension during the COVID-19 pandemic (2020–2022): clinical outcomes, prognostic factors, and response to vaccination
Introduction
Pulmonary arterial hypertension (PAH) and inoperable, recurrent or persistent chronic thromboembolic pulmonary hypertension (CTEPH) are severe diseases characterized by increased mean pulmonary arterial pressure (>20 mm Hg), pulmonary vascular resistance above 2 Wood units and pulmonary arterial wedge pressure equal to or lower than 15 mm Hg caused by remodeling in pulmonary arterioles and / or embolization.1 Patients with PAH and CTEPH were recognized as a COVID‑19 high‑risk group. Consistently, during the dominance of early SARS‑CoV‑2 lineages, their hospitalization and fatality rates were higher than in the general population.2 However, with COVID‑19 vaccination becoming available and SARS‑CoV‑2 evolving into lineages associated with a milder course of the disease, it became important to understand whether PAH and CTEPH patients are still at an increased risk advocating for additional protective measures.
This study aimed to comprehensively understand how the situation of PAH and CTEPH patients evolved during the COVID‑19 pandemic. For this purpose, all such patients treated in one of the Polish referral cardiology centers were monitored from the beginning of the COVID‑19 pandemic (March 2020) till December 2022. The primary end point was an assessment of the incidence of SARS‑CoV‑2 infections, mortality, and the need for hospitalization for COVID‑19 in the patients with PAH or CTEPH. The secondary end point included an assessment of 1) clinical risk factors for death and hospitalization due to COVID‑19, 2) humoral response to COVID‑19 vaccination, and 3) prognosis during 1‑year follow‑up: risk factors of death and hospitalization for exacerbation of PAH or CTEPH, including a history of COVID‑19 and antispike (anti‑S) antibody concentration. So far, these issues have not been addressed jointly in the PAH and CTEPH patients. The study’s novelty includes a comprehensive approach focused on morbidity, mortality, SARS‑CoV‑2 reinfections, long‑term COVID‑19 consequences, prognostic factors, and the response to COVID‑19 vaccination in the PAH and CTEPH patients, as well as exploring their situation following infections with viral variants differing in clinical significance.
Patients and methods
Study design
All consecutive patients with diagnosed PAH or inoperable or persistent / recurrent CTEPH treated in the referral cardiology center (First Department of Cardiology, Poznan University of Medical Sciences, Poland) were included in the study. All patients underwent regular follow‑up every 3 to 6 months. Echocardiography, a 6‑minute walk test (6MWT), and laboratory results, including N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP) and troponin I, were evaluated at each visit in our hospital. All study patients received recommended specific drugs, and staged balloon angioplasty was performed in CTEPH patients.
The data assessing COVID‑19 and vaccination status in each patient were recorded between March 2020 and December 2022. Using sequence data submitted by Polish laboratories to the Global Initiative on Sharing All Influenza Data, the most reliable database on SARS‑CoV‑2 variant prevalence in different regions of the world, 3 periods of the COVID‑19 pandemic were distinguished, namely 1) pre‑Delta period (March 1, 2020–June 30, 2021), 2) Delta period (July 1, 2021–December 31, 2021), and Omicron period (January 1, 2022–December 31, 2022), which correspond to the periods of dominance of the variants preceding the appearance of the Delta variant, dominance of the Delta variant, and of the Omicron variant, respectively.3
Vaccinated patients were defined as those who received at least 2 doses of mRNA vaccines (BNT162b2, BioNTech / Pfizer, or mRNA‑1273 from Moderna) or chimpanzee adenovirus‑based vaccine (AZD1222, Oxford / AstraZeneca) or a single‑dose adenoviral vaccine (Janssen Ad26.COV2.S). The data associated with vaccination, including dates and types, were derived from the Polish national database (www.gabinet.gov.pl).
Serum concentration of anti‑S antibodies was evaluated between October 2021 and March 2022 with the Siemens SARS‑CoV‑2 immunoglobulin (Ig) G assays (Siemens Healthineers, Munich, Germany) at the Central Laboratory of our hospital. The cutoff concentration indicating seropositivity was 20 BAU/ml.
During the follow‑up period, the data were collected at regularly scheduled visits and emergency hospitalizations. Clinical worsening comprised a change in the World Health Organization (WHO) functional class (FC), a need for specific treatment escalation, or emergency hospitalization associated with right ventricular failure.
The study was approved by the Bioethics Committee of the Poznan University of Medical Sciences, Poland (372/21). All patients included in the study signed their informed consent.
Statistical analysis
Statistical analyses were performed with the PQStat package version 1.6.6 (PQStat Software, Poznań, Poland). The distribution of data was assessed with the Shapiro–Wilk test. The data were presented as median values (interquartile range [IQR]). Group comparison (the pre‑Delta and Delta periods vs the Omicron period), assessing the number of COVID‑19 cases, hospitalizations and deaths due to COVID‑19, and the number of vaccinated patients, was performed with the Fisher exact test. Univariable Cox regression analysis assessed the risk factors of death and hospitalization due to COVID‑19, and multivariable Cox regression analyses determined the risk factors of death and hospitalization due to clinical worsening. P value below 0.05 was deemed significant.
Results
Clinical characteristics
A total of 88 patients with PAH (n = 62; 70%) or inoperable / recurrent / persistent CTEPH (n = 26; 30%) were included in the study. Their median (IQR) age was 58 (46–69) years, and a majority (62%) were women (Supplementary material, Table S1)
COVID‑19 vaccination and anti‑spike protein antibodies
A majority of patients (n = 68; 77%) were vaccinated against COVID‑19, including 48 (70%) with BNT162b2, 8 (12%) with mRNA‑1273, 8 (12%) with AZD1222, and 4 (6%) with Ad26.COV2.S vaccine. In addition, 47 individuals (69%) received 1 booster dose of the mRNA vaccine. The concentration of anti‑S IgG antibodies was assessed in 75 patients (85%). Among them, 14 (19%) were seronegative, with 5 (36%) being vaccinated (2 with Ad26.COV2.S, 2 with mRNA‑1273, and 1 with the BNT162b2 vaccine). There were only 2 nonresponders (7%) among all the vaccinated patients. In contrast, 5 unvaccinated patients (25% of the unvaccinated individuals) had positive antibody levels: 3 of them had a confirmed and 2 not confirmed SARS‑CoV‑2 infection.
SARS‑CoV‑2 infection and COVID‑19 clinical course
During the study period (from March 2020 to December 2022), 34 patients (39%) had a SARS‑CoV‑2 infection confirmed by a real‑time polymerase chain reaction or an antigen test.
As many as 30 individuals (34%) were infected with SARS‑CoV‑2 between April 2020 and December 2021 (pre‑Delta and Delta periods). Among them, only 2 patients (7% of this subgroup; 2% of the entire group) were vaccinated with 2 doses of the vaccine. One of them (3% of the subgroup; 1% of the entire group) received 1 dose of the mRNA vaccine, whereas 27 individuals (90%) had not been vaccinated. In this period, 10 patients (34% of the subgroup; 11% of the entire group) were hospitalized for COVID‑19 and 5 of them (17% of the subgroup; 6% of the entire group) died. All of these patients were unvaccinated (Figure 1A and 1B).
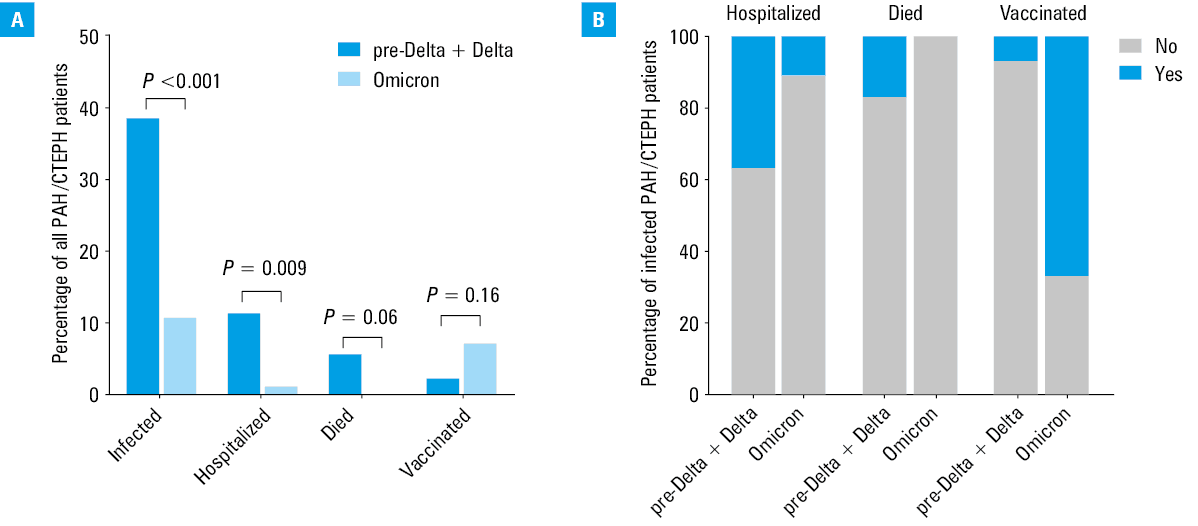
Abbreviations: CTEPH, chronic thromboembolic pulmonary hypertension; PAH, pulmonary arterial hypertension
Between January 2022 and December 2022 (Omicron period), 9 patients (10% of the entire group) had a confirmed SARS‑CoV‑2 infection (with 50% of cases representing reinfection), and 6 of them (67% of the subgroup; 7% of the entire group) were vaccinated. Only 1 patient (11% of the subgroup; 1% of the entire group) who was unvaccinated was hospitalized for COVID‑19, and no deaths were recorded (Figure 1A and 1B). A group comparison revealed a higher number of COVID‑19 cases (P <0.001), hospitalizations (P = 0.009), and deaths (5 vs 0 patients; P = 0.06) for COVID‑19 in the pre‑Delta and Delta periods as compared with the Omicron period. However, the number of vaccinated and infected patients during the pre‑Delta and Delta periods was not higher than in the Omicron period (P = 0.16; Figure 1A).
Significant risk factors of death in a univariable Cox analysis in the patients with COVID‑19 included a lack of vaccination, older age, higher mean right atrial pressure (mRAP), red blood cell distribution width (RDW) and right atrial area (RAA), lower mixed venous oxygen saturation (Sat mixO2), and lower 6MWT score (Supplementary material, Table S2). Due to the small size of the study group, multivariable analysis was not performed. None of the assessed risk factors were found significant in the patients hospitalized for COVID‑19 vs those not requiring hospitalization.
One‑year follow‑up
At 1‑year follow‑up, mortality and hospitalization due to PH exacerbation reached 6% (n = 5) and 12% (n = 10), respectively. One case of fatal outcome was suspected to be associated with COVID‑19 prior to hospitalization (the patient had a high level of anti‑S antibodies on admission, ie, 4051.3 BAU/ml without vaccination). Significant risk factors of mortality and hospitalization due to clinical worsening in the univariable Cox regression analysis included higher WHO FC, RDW, mRAP, RAA, and mean pulmonary arterial pressure (mPAP), and independent risk factors in the multivariable analysis were RDW and RAA (Supplementary material, Table S3). A history of vaccination, a history of COVID‑19, and anti‑S antibody concentration were not predictors of death and hospitalization due to PH exacerbation.
Discussion
This study documents the experience of a referral cardiology center with PAH and CTEPH patients during the COVID‑19 pandemic encompassing different periods, including that dominated by the SARS‑CoV‑2 Omicron lineage. As shown, hospitalizations for COVID‑19 were more frequent during the pre‑Delta and Delta periods, and all deaths in the study cohort occurred before the emergence of the Omicron variant. This is in line with previous observations of high mortality rates among patients with PAH and CTEPH during the dominance of earlier SARS‑CoV‑2 lineages before the COVID‑19 vaccines were widely available.4,5
Before our study, the situation of PAH and CTEPH patients during the dominance of the Omicron SARS‑CoV‑2 variant was scarcely explored. Our findings indicate that during this period, the COVID‑19 course was milder, which is consistent with other analyses encompassing the general population or patients with different comorbidities.6 Indeed, there were no deaths during the Omicron period, in contrast with the early phases of the pandemic, when 17% of the infected patients died. Moreover, hospitalizations due to COVID‑19 were by 23% more frequent during the pre‑Delta and Delta waves than in the Omicron period. The milder course of the infection in the PAH and CTEPH patients is likely a joint effect of vaccinations, to which the majority of these patients adhered (by 60% more than in the general population), and mutation‑driven changes in the viral biology, particularly less efficient membrane fusion kinetics than in the previous SARS‑CoV‑2 lineages, preferential endocytic cell entry, and faster replication in the bronchus but less efficient in the lung cells.7,8 We hypothesize that it was the milder course of Omicron infection that did not prompt patients to take tests, which resulted in a lower percentage of confirmed Omicron cases than in the earlier waves of the pandemic.
As shown in our study, the patients with PAH or CTEPH who died due to COVID‑19 were significantly older and had a more advanced disease, including worse 6MWT score, higher mRAP, RAA, RDW, and lower Sat mixO2. In contrast, NT‑proBNP levels did not vary in the deceased patients, indicating RDW as a better biomarker of fatal COVID‑19 outcome in the PAH/CTEPH patients. Moreover, the study identified RDW as an independent predictor of death and hospitalization due to clinical worsening in 1‑year follow‑up. Previously, RDW, a basic and low‑cost parameter, was shown to be a valuable prognostic biomarker of death and clinical exacerbation in PAH and CTEPH patients.9 Another independent predictor of this composite end point was RAA, and risk factors derived from a univariable analysis were WHO FC, mPAP, and mRAP. All these clinical and hemodynamic parameters are well‑established prognostic factors.1,10,11
Importantly, a history of COVID‑19 vaccination, a history of SARS‑CoV‑2 infection, and concentration of anti‑S IgG antibodies were not predictors of death and hospitalization for PH exacerbation. Our results are in line with the observations of patients with PAH/CTEPH from other referral centers, where the calculated 1‑year risk of death due to PH did not increase significantly after surviving mild or moderate COVID‑19.12
Our cohort adhered to the primary course of vaccination at a rate of 77%, which was higher than a mean level in the European Union countries (73%) and in the general Polish population (60%).13 This indicates that the PAH and CTEPH patients were generally aware of COVID‑19 threats and willing to use preventive measures. Moreover, the response to COVID‑19 vaccination was high, with only 7% of vaccinated individuals revealing a lack of anti‑S antibodies. Of these, only 1 patient was immunocompromised. The mechanisms behind a lack of humoral response in other nonresponders would require further studies. However, one should note that being seronegative after vaccination does not exclude generating an adaptive cellular response, which is pivotal for preventing progression to more severe COVID‑19 in the case of a breakthrough infection.14
Our study has a few limitations. First, despite the extended follow‑up, it was a single‑center study with a limited number of patients. Second, the anti‑S antibodies were measured only once, while their concentration may decrease over time, translating into an increased risk of infection. Third, adaptive cellular immune responses were not measured. Last but not least, although the study showed the milder effect of the Omicron lineage in the patients with PAH and CTEPH, one cannot exclude the potential emergence of clinically more relevant SARS‑CoV‑2 variants in the future.15,16 Although the Omicron lineage is generally characterized by lower fusogenicity, a parameter that affects viral pathogenicity, more recent sublineages that emerged after the end of this study, including the XBB sublineage, reveal enhanced fusogenic potential.17,18 However, real‑world observations show that so far this has not translated into greater clinical relevance, which likely underlines the role of immunity levels induced by vaccination and previous SARS‑CoV‑2 infections.19 Nevertheless, further exploration of the impact of COVID‑19 on the PAH and CTEPH patients, exposed to the continuously evolving pathogen, is pivotal.
Conclusions
This study provides novel information on PAH and CTEPH patients and indicates that they were at a lower risk of severe COVID‑19 after the emergence of the Omicron SARS‑CoV‑2 lineage, although they experienced infections and reinfections despite being vaccinated. Before the Omicron‑dominated period, the risk factors of death due to COVID‑19 included worse 6MWT score, higher mRAP, RAA, RDW, and lower Sat mixO2 values. Adherence to COVID‑19 vaccination in the studied group was higher than in the general population, and the humoral response to the vaccines was satisfactory. Having COVID‑19 and being vaccinated against it were not associated with clinical worsening during 1‑year follow‑up, contrary to higher RDW and RAA. The approach of the present study could also be implemented in the context of infections with other respiratory viruses, such as influenza viruses or respiratory syncytial virus, which constitute a significant risk for the PAH and CTEPH patients, and for which vaccinations are also available.
- Humbert M, Kovacs G, Hoeper MM, et al; ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN‑LUNG). Eur Heart J. 2022; 43: 3618‑3731.
- Lee JD, Burger CD, Delossantos GB, et al. A survey‑based estimate of COVID‑19 incidence and outcomes among patients with pulmonary arterial hypertension or chronic thromboembolic pulmonary hypertension and impact on the process of care. Ann Am Thorac Soc. 2020; 17: 1576‑1582. | Crossref
- Flisiak R, Rzymski P, Zarębska‑Michaluk D, et al. Variability in the clinical course of COVID‑19 in a retrospective analysis of a large real‑world database. Viruses. 2023; 15: 149. | Crossref
- Mamzer A, Waligora M, Kopec G, et al. Impact of the COVID‑19 pandemic on pulmonary hypertension patients: insights from the BNP‑PL national database. Int J Environ Res Public Health. 2022; 10: 8423. | Crossref
- Wieteska‑Miłek M, Kuśmierczyk‑Droszcz B, Ryczek R, et al. Outcomes of COVID‑19 in patients vaccinated and unvaccinated against SARS‑CoV‑2 and suffering from pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. Pol Arch Intern Med. 2023; 133: 16406. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION