Introduction
Lipoprotein (Lp)(a) is a complex plasma protein that consists of 3 components, that is, low‑density lipoprotein (LDL) cholesterol with apolipoprotein B100, which is bound to apolipoprotein(a) (apo[a]) with a disulfide bond.1 Lp(a) is considered a proatherosclerotic, proinflammatory, prothrombotic, and antifibrinolytic compound. Its functions include binding and carrying oxidized phospholipids (OxPLs) that are involved in plaque sensibility and its destabilization, activating and inhibiting various stages of the coagulation cascade, inducing expression of inflammatory cytokines, such as interleukin (IL)-1β, IL‑6, or tumor necrosis factor α.1 Elevated Lp(a) levels increase a risk of degenerative aortic valve stenosis, atherosclerosis, myocardial infarction and in‑stent restenosis, ischemic stroke, or atherothrombosis.2,3 In patients with severe aortic stenosis and Lp(a) level equal to or above 50 mg/dl, elevated valvular OxPL expression was observed.4 According to recent cardiovascular recommendations of the European Society of Cardiology / European Atherosclerosis Society from 2019,5 Lp(a) level should be measured once in a lifetime in every person. Levels of this protein are genetically determined by the LPA gene, predominantly inherited in an autosomal codominant manner, and remain stable over lifetime.6,7 Diet and lifestyle have only minor impact on the Lp(a) level.8 In our previous study,9 we showed that elevated Lp(a) levels in patients with COVID‑19 might affect the course of the disease. Patients with Lp(a) level equal to or above 30 mg/dl were hospitalized significantly longer, demonstrated more extensive pulmonary radiologic changes, higher oxygen demand on admission, increased risk of high‑flow nasal oxygen therapy, intubation, intensive care unit hospitalization, and death without a higher risk of pulmonary embolism.
Our study aimed to evaluate Lp(a) levels in patients from our previous work9 a year after COVID‑19–induced acute inflammatory state.
Patients and methods
Our study was conducted between November 2020 and April 2021 (first visit) and between November 2021 and April 2022 (second visit). Of 124 patients with polymerase chain reaction–confirmed COVID‑19 that took part in our previous study, 44 had Lp(a) levels equal to or above 30 mg/dl during the disease. Of those, 7 died during hospitalization, 18 did not agree to participate in the second Lp(a) measurement, and 2 were excluded due to insufficient data. We finally included 17 patients with elevated Lp(a) levels who agreed to re‑examination a year after their hospitalization for COVID‑19 (second visit). In this prospective pilot study, the following parameters were measured, analyzed, and compared with the results obtained in the previous research: total cholesterol (TC; reference range [RR], 130–200 mg/dl, LDL cholesterol (LDL‑C), high‑density lipoprotein (HDL) cholesterol (HDL‑C; RR >65 mg/dl), non‑HDL cholesterol (non–HDL‑C), triglycerides (TG; RR <150 mg/dl), Lp(a) (RR <30 mg/dl), IL‑6 (RR <7 pg/ml), glomerular filtration rate (GFR; RR >60 ml/min/1.73 m2), platelet count (RR, 150–400 × 109/l), leukocyte count (RR, 4–10 × 109/l), lymphocyte count (RR, 0.9–5.2 × 109/l), and neutrophil count (RR, 1.9–8 × 109/l).8 Lp(a) measurement was performed using kinetic nephelometry (Immage Immunchemie System, Fa. Beckman Coulter, Indianapolis, Indiana, United States). All parameters were compared in 3 groups of patients: 1) with Lp(a) levels below 30 mg/dl (n = 80), 2) with Lp(a) levels equal to or above 30 mg/dl and with no follow‑up visit (n = 27), and 3) with Lp(a) levels equal to or above 30 mg/dl and a follow‑up visit a year after hospitalization (n = 17).
Statistical analysis
Statistical analyses were performed with the GraphPad Prism 9.0 package (GraphPad Software, San Diego, California, United States). All tests were considered significant at a P value below 0.05. Data distribution was verified with the Shapiro–Wilk test. Most variables had a non‑normal distribution. Relationships between pairs of groups were tested with the t test (normal distribution) and the Wilcoxon test (non‑normal distribution). Relationships between unpaired 3 groups were tested with the Kruskal–Wallis test (non‑normal distribution) and with the ordinary one‑way analysis of variance (ANOVA) (normal distribution). The Dunn test (Kruskal–Wallis) and the Tukey test (ANOVA) were used for post hoc comparisons. The χ2 test was used for categorical variables.
The study was approved by the Bioethical Committee of the Medical University of Lodz, Poland (RNN/122/21/KE).
Results
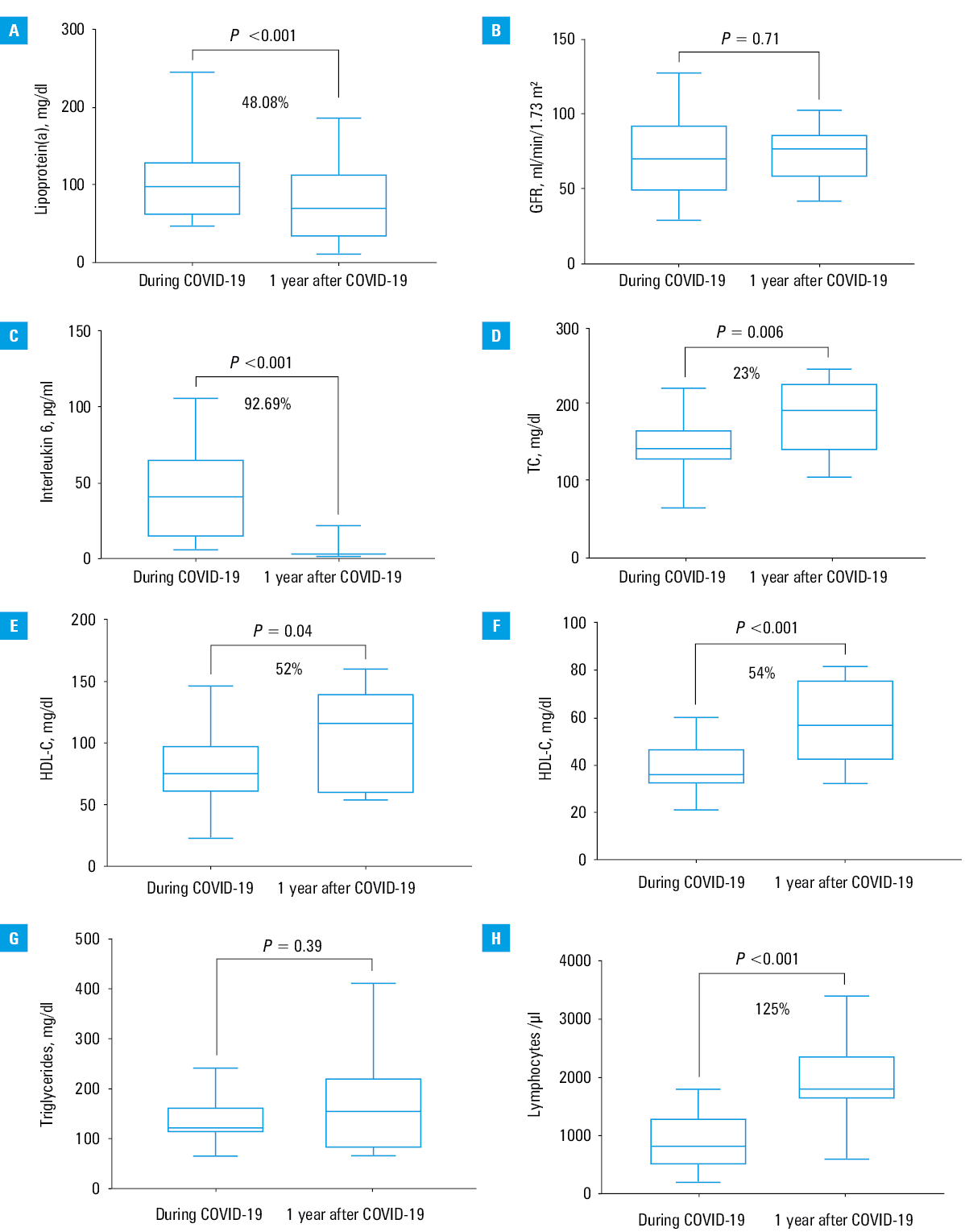
The mean (SD) age of our 17 patients was 65.6 (10) years. Men constituted 58.8% (n = 10) and women 41.2% (n = 7) of the study population. Median (interquartile range [IQR]) Lp(a) concentration during acute inflammatory state due to COVID‑19 was 98 (60.3–130) mg/dl, and a year after the disease it dropped to 50.88 (31.7–116.2) mg/dl (P = 0.001) (Figure 1A). In 3 patients, the Lp(a) level elevated during COVID‑19 fell below the threshold of 30 mg/dl at the follow‑up visit. There was no decrease in the Lp(a) level in the other 3 patients. Median GFR did not change much in our patients during COVID‑19 (70.25 [48–93] ml/min/1.73 m2; P = 0.7) and a year after (73.72 [58–82] ml/min/1.73 m2; P = 0.7) (Figure 1B). Intensity of the inflammatory state was assessed based on the median concentration of IL‑6, which decreased a year after hospitalization from 41.5 (14–66) pg/ml to 3.03 (2.5–3.5) pg/ml (P <0.001) (Figure 1C). According to the lipid panel, median values of the following blood lipids increased after COVID‑19: TC from 144 (129–169) mg/dl to 187 (138–230) mg/dl (P = 0.01) (Figure 1D), LDL‑C from 75 (60.5–98.5) mg/dl to 114 (58–141) mg/dl (P = 0.04) (Figure 1E), HDL‑C from 36.1 (32–47) mg/dl to 55.6 (41–77) mg/dl (P <0.001) (Figure 1F), non–HDL‑C from 106 (92–134) mg/dl to 129 (75–166) mg/dl (P = 0.21), and TG from 122 (112–164) mg/dl to 153 (75–237) mg/dl (P = 0.4) (Figure 1G). Differences in important parameters in the patients with elevated, Lp(a) level and with and without the follow‑up visit were significant only for TC and non–HDL‑C (Supplementary material, Table S1). We also analyzed whole blood count results. A year after COVID‑19, median leukocyte count did not change (6.3 [5.6–10.6] × 109/l vs 6.3 [5–7.2] × 109/l; (P = 0.64), median neutrophil count decreased by 34% from 5 (3.25–6.1) × 109/l to 3.3 (1.9–4.1) × 109/l (P = 0.008), and median lymphocyte count increased by 125%, from 0.8 (0.5–1.3) × 109/l to 1.8 (1.6–2.4) × 109/l (P <0.001) (Figure 1H). Platelet count hardly changed from 171 (140.5–245.5) × 109/l to 204 (147–242) × 109/l (P = 0.96).
Discussion
An association of Lp(a) with atherosclerosis‑related diseases has been well established, and our previous results suggest that it may also play a role in acute inflammatory states, such as SARS‑CoV‑2 infections.2,3,9 The main finding of our study is the fact that Lp(a) levels elevated during COVID‑19 decreased after a year by 48.08%. To the best of our knowledge, this study is unique as it demonstrates a potential transient increase in Lp(a) levels during an acute infection, such as SARS‑CoV‑2, challenging the previous belief that Lp(a) remains stable over a lifetime. A large cohort study, based on United Kingdom biobank data, revealed that elevated Lp(a) during COVID‑19 correlated more strongly with a risk of ischemic heart disease than in COVID‑19–negative patients.10 It has been confirmed in various studies that COVID‑19 induces acute inflammatory state, which may even manifest as cytokine storm with markedly elevated proinflammatory cytokines.11 Our results showed that the 48.08% decrease in the Lp(a) level, observed a year after COVID‑19, was accompanied by a significant decrease (by 92.69%) in the IL‑6 level. This suggests that Lp(a) levels may depend on ongoing inflammation, which was also noticed in a review by Dzobo et al,12 where Lp(a) was considered an acute‑phase protein. Our results may be explained by studies showing that in response to a proinflammatory stimulus, an increased IL‑6 level may activate a response element in the LPA gene promoter, and thus boost the production of apo(a) and induce an increase in the Lp(a) level.13 However, our previous study showed that only 44 of 124 patients with COVID‑19 demonstrated elevated Lp(a) levels (>30 mg/dl), which did not correlate with other inflammatory parameters.9 Interestingly, in our previous analysis, Lp(a) level equal to or above 30 mg/dl was associated with a higher death rate of 15.9% (7/44) than that of 6.25% (5/80) in the low Lp(a) group (χ2 test; one‑sided P = 0.04).9 Lp(a) upper limit of normal may be exceeded in patients with impaired renal function, when Lp(a) metabolic clearance is decreased. However, we excluded this possibility, as GFR in our patients did not change significantly over time.14
Another finding of our study is the fact that the significant decrease in Lp(a) and IL‑6 levels after COVID‑19 was associated with an opposite trend regarding other lipid parameters, including TC, LDL‑C, and HDL‑C, which increased significantly by 23%, 52%, and 54%, respectively, a year after the disease. Lower concentrations of lipids during COVID‑19 had been observed before and might be explained by their hypothetical role in viral replication or SARS‑CoV‑2 cellular entry by forming lipid rafts.15 Laboratory tests confirmed lymphopenia during COVID‑19. This observation is a major immunologic abnormality characteristic of SARS‑CoV‑2 infection, and it is also a prognostic factor of the disease outcome. There are several possible explanations for lymphopenia during COVID‑19, and some of them assume that proinflammatory ILs released during cytokine storm induce lymphocyte apoptosis.16 In our patients, lymphocyte count significantly increased by 125% a year after COVID‑19, which was associated with subsidence of the inflammatory state.
Limitations
The main limitation of the study is a small number of participants. Yet, this is a pilot study, and its results indicate a need for carrying out an analysis in a larger group of patients. A lack of Lp(a) analysis in patients with Lp(a) level below 30 mg/dl during COVID‑19 is another limitation. However, from the clinical point of view, even if their Lp(a) levels decreased significantly, these individuals would remain in the category of low‑level Lp(a), and consequently their cardiovascular risk associated with Lp(a) would remain unchanged.
Conclusions
Our research suggests that Lp(a) level may not be stable over a lifetime and may temporarily increase during an inflammatory state, including SARS‑CoV‑2 infection. Despite a significant reduction in Lp(a) level after COVID‑19, a majority of the patients still presented values exceeding the threshold of 30 mg/dl. This suggests that their cardiovascular risk remains elevated and may be potentially further aggravated by associated increase in lipid parameters, particularly LDL‑C. Due to differences in the measurement of Lp(a) level caused by acute inflammatory state, it should be considered whether determining Lp(a) once in a lifetime, as the current guidelines indicate, is sufficient. However, it requires further research conducted in larger groups of patients.
- Ugovšek S, Šebeštjen M. Lipoprotein (a)—the crossroads of atherosclerosis, atherothrombosis and inflammation. Biomolecules. 2021; 12: 26. | Crossref
- Lindman BR, Clavel M, Mathieu P, et al. Calcific aortic stenosis. Nat Rev Dis Prim. 2016; 2: 16006. | Crossref
- Li J, Li S, Pan Y, et al. Relationship between lipoprotein (a) [Lp(a)] and cognition in different ischemic stroke subtypes. Front Neurol. 2021; 12: 1‑8. | Crossref
- Kopytek M, Ząbczyk M, Mazur P, et al. Oxidized phospholipids associated with lipoprotein(a) contribute to hypofibrinolysis in severe aortic stenosis. Pol Arch Intern Med. 2022; 132: 16372. | Crossref
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41: 111‑188.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION