Alcohol, health loss, and mortality: can wine really save the good name of moderate alcohol consumption?
Key words: alcohol, mortality, polyphenols, prevention, wine

 CC BY 4.0
CC BY 4.0
Alcohol, health loss, and mortality: can wine really save the good name of moderate alcohol consumption?
It is estimated that one‑third of the world’s population consumes alcohol. At the same time, it is well‑known that excessive alcohol consumption in one of the leading causes of premature mortality. The history of production of alcoholic beverages, especially wine, dates back as long as 8000 years. However, people soon realized adverse effects of alcohol abuse and tried to limit its consumption. Higher alcohol consumption is associated with health loss and increased risk of all‑cause mortality. It is linearly associated with a greater risk of many types of cancers, liver disease, incidence of atrial fibrillation, hemorrhagic stroke, or heart failure. Although many scientific societies recommend reduction of alcohol intake and specify the recommended limits of consumption, there is no proven safe amount of alcohol for the general population. There are conflicting data on the effect of low‑to‑moderate alcohol consumption on mortality, with most of the studies indicating a J‑shaped curve related mostly to a reduction of coronary artery disease complications, including cardiovascular death. Among different types of alcohol, red wine consumption may have different health effects, due to its high content of antioxidative polyphenols. Wine, together with abundance of plant‑based foods, olive oil, and fish, is an important part of the Mediterranean diet. There are both observational and randomized studies documenting a wide spectrum of health‑promoting effects of such a diet, especially a reduction in major adverse cardiovascular events. People who want to drink alcohol should be advised to limit their consumption to a minimum, and should consider choosing red wine.
Brief history of alcohol consumption
Determining the exact origins of alcohol consumption is challenging. The history of wine began in Georgia 8000 years ago. Hippocrates did not recommend wine to children and pregnant women, and he expressed his philosophy regarding the beneficial effects of wine in a well‑known principle: “Wine is fit for man in a wonderful way provided that it is taken with good sense by the sick as well as the healthy.” Galen, who successfully developed this theory, also considered wine an important element of medical therapy. In his work De antidotis, he also mentioned many wine‑based antidotes against poisons commonly used at that time.1,2 Growing popularity of alcohol consumption was linked to its perceived medicinal properties. Aristotle noted wine’s sedative, analgesic, diuretic, and antidiarrheic properties around the 4th century BC. For ages, until the 20th century, alcohol was widely used as a medicinal remedy, as seen in the New Testament’s parable of the Good Samaritan, where wine was applied to dress wounds.1,2 In Poland, the first vineyards appeared 1000 years ago on the Wawel Hill. Wine is a drink resulting from alcoholic fermentation, obtained exclusively from fresh grapes or their juice (so‑called must), with a possible addition of permitted substances, produced in accordance with established enological processes.1,2
It is believed that fermented drinks were consumed as far back as in the Late Neolithic period. The earliest surviving texts mentioning beer brewing and consumption date back to around 4000 BC from Mesopotamia.1,2
Egypt implemented the first restrictions on alcohol consumption, particularly in temples, to prevent theft, intoxication, and other types of abuse. Around 2000 BC, the pharaoh’s army in Egypt introduced a ban on alcohol to avoid losing battles due to soldiers’ alcohol abuse.1
Development of the process of alcohol distillation is attributed to an Arab alchemist Jābiribn Hayyān around 800 AD. In Poland, the first taverns emerged in the 11th century, with beer being the primary beverage until the early Enlightenment, when alcohol distillation became common. Mass‑scale alcohol abuse in Poland began in the 16th century, with establishment and spread of propination, that is, a monopoly granted to nobles over the production and sale of alcoholic beverages.1
Over the centuries, alcohol consumption statistics in Poland have fluctuated. Historical data from the first half of the 19th century indicate that in the Kingdom of Poland, annual per capita consumption of pure alcohol could reach up to 38 liters.3
The word “alcohol” originates from the Arabic “al‑kuhl,” a black powder used for cosmetic and medical purposes. Initially applied to powders and elixirs, it eventually referred to volatile substances, such as alcohol.
Current epidemiologic data on alcohol consumption
Global epidemiology
In 2016, approximately 32.5% (with a 95% uncertainty interval [UI], 30–35.2) of the world’s population were reported as current drinkers. Specifically, 25% of women (95% UI, 23–27) and 39% of men (95% UI, 36–43) were identified as such. These percentages equal to a total of 2.4 billion people (95% UI, 2.2–2.6) who were current drinkers, comprising 1.5 billion current drinkers among men (95% UI, 1.4–1.6) and 0.9 billion among women (95% UI, 0.8–1). On a global scale, the average amount of alcohol consumed daily was 0.73 standard drinks (1 standard drink = 10 g of pure ethanol) (95% UI, 0.68–0.78) for women and 1.7 standard drinks (95% UI, 1.5–1.9) for men.4
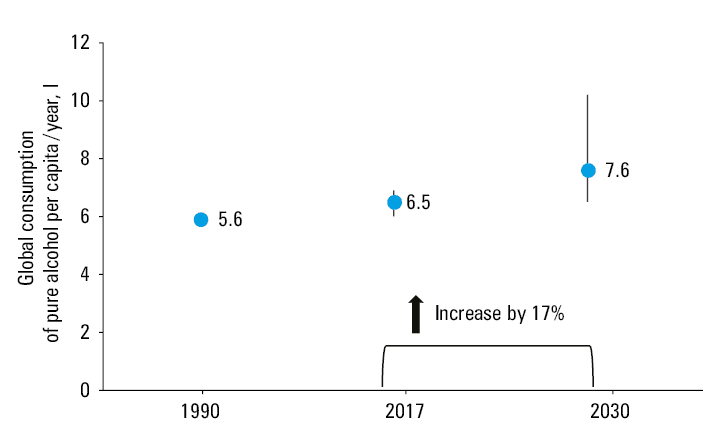
In an interesting study by Manthey et al,5 data on alcohol consumption in 189 countries in the years 1990–2017 were summarized and forecasted until 2030. Global alcohol consumption was found to increase between 1990 and 2017. Moreover, the researchers predicted a further increase in alcohol consumption by 2030 (Figure 1).
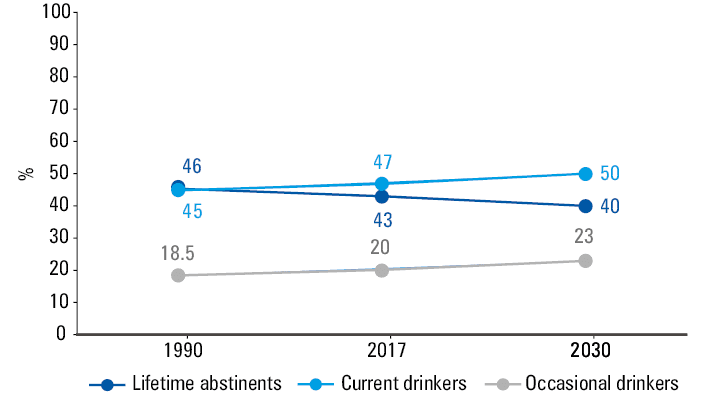
The prevalence of abstinence around the world is also gradually declining. Additionally, the percentage of people actively consuming alcohol and consuming alcohol episodically is growing. In the forecasts until 2030, these trends are expected to rise (Figure 2).5
The COVID‑19 pandemic significantly affected health‑related behaviors, including the amount of alcohol consumed and body weight.6,7 According to data from the National Institute on Alcohol Abuse and Alcoholism, during the first year of the pandemic, alcohol sales jumped by nearly 3%, the largest increase in more than 50 years. Multiple small studies suggest that during the pandemic, about 25% of people drank more than usual, often to cope with stress. Sales of hard liquor, or spirits, accounted for most of the increase.8 This resulted in a growing number of deaths related to alcohol consumption. In 2019, that is, before the COVID‑19 pandemic, there were 78 927 such cases and during the COVID‑19 pandemic 99 017 and 108 791 in 2020 and 2121, respectively.8 A study by Raza et al,9 including 45 292 people covered by the National Health and Nutrition Examination Survey (1999–2020), assessed the structure of alcohol consumption among obese patients. The authors showed that the overall weighted prevalence of combined heavy alcohol drinking and obesity increased from 1.8% (95% CI, 1.2%–3.1%) in 1999–2000 to 3.1% (95% CI, 2.7%–3.7%) in 2017–2020, representing an increase by 72%.9
According to estimates of the Organization for Economic Cooperation and Development made before the onset of the COVID‑19 pandemic, consuming more than 1–1.5 drinks per day is linked to approximately 1.1 billion new cases of alcohol dependence, constituting 88% of all cases. Additionally, this level of alcohol consumption is associated with 37 million cases of injuries (4%), 5 million cases of cirrhosis (38%), and 10 million cases of alcohol‑related cancer (4%). These projections span over the next 30 years and cover 52 countries, predicting millions of cases of various other diseases as well.10
Epidemiology in Poland
According to data from the World Health Organization (WHO) from 2019, Poland was among the countries with the highest alcohol consumption (10–13 l of pure alcohol per capita per year).11 In 2019, median (interquartile range [IQR]) alcohol consumption in Poland was 10.96 (8.2–13.56) l per capita. When broken down by the type of alcohol, the most popular in Poland were beer (5.72 [3.59–7.97] l), vodka (4.36 [2.54–5.98] l), and wine (0.88 [0.53–1.23] l).1 WHO forecasts are not optimistic, as they indicate that median alcohol consumption in Poland in 2025 will amount to 12.7 (11–14.4) l per capita.11
A significant problem contributing to the growing alcohol consumption in Poland is low social awareness. It is interesting to note that a relatively small percentage of Poles clearly recognize beer (46%), flavored beer (35%), and cider (29%) as alcohol.11 Importantly, low awareness of the effects of alcohol consumption on health refers to all age groups,1,12-17 and might be accompanied by improper diet and smoking.18
A standard unit of alcohol is 10 g (or 12.5 ml) of pure ethyl alcohol (ethanol). This dose, based on the most frequently consumed types of alcoholic beverages, is 200 g of 5% beer; 100 g of 10% wine, or 25 g of 40% vodka.1 It is worth emphasizing; however, that a definition of the standard unit of alcohol (pure ethanol content) differs in individual countries, for example, in the United States it is 14 g, in Germany 10–12 g, in Italy and Finland 12 g, in Spain and Poland 10 g, in Canada 13.6 g, in the United Kingdom (UK) 8 g, and in Japan 20 g.19
To sum up, epidemiologic data indicate that alcohol consumption in Poland significantly exceeds the global average. The trends are not favorable and indicate an increase in alcohol consumption, both worldwide and in Poland. In Poland, beer and spirits are the most popular.
Guidelines of scientific societies on permissible doses of alcohol
Guidelines of various scientific societies recommend reduction of alcohol intake or total abstinence.20-28 They also specify the recommended permissible amount of alcohol consumed (Table 1).
Scientific society | Recommendation |
a In the United States, 1 standard drink (or 1 alcoholic drink equivalent) contains roughly 14 g of pure alcohol (eg, 145 ml of wine), which is more than in Europe.19 | |
International Society of Hypertension (2024) | As part of the prevention of hypertension, it is recommended to limit the amount of alcohol consumed, ideally to zero. However, the recommended daily upper limit for alcohol consumption is 2 standard drinks for men and 1 for women. |
European Society of Hypertension (2023) | Adult men and women with elevated blood pressure or hypertension who currently consume alcohol (≥3 drinks/day) should be advised that reduction of alcohol intake close to abstinence will lower their blood pressure. |
Polish Society of Diabetology (2023) | Drinking alcohol by people with diabetes is not recommended. |
European Society of Cardiology (Cardiovascular Prevention 2021) | It is recommended to restrict alcohol consumption to a maximum of 100 g per week. |
Polish Lipid Association (2021) | Patients with lipid disorders should limit their alcohol consumption to a minimum. |
Polish Society of Hypertension (2019) | Alcohol consumption should be limited:
|
American Heart Association and American College of Cardiology (2019) | Alcohol consumption should be limited: in men: ≤2 drinks/day,a
in women: ≤1 drink/day |
Deutsche Hauptstelle für Suchtfragen (German Head Office for Dependence Matters, 2019) | Men: ≤24 g of alcohol per day, at least 2 nonalcoholic days per week
Women: ≤12 g of alcohol per day, at least 2 nonalcoholic days per week |
Alcohol and mortality or health loss
A meta‑analysis of 107 studies, including 4 838 825 participants and published by Zhao et al,29 assessed the impact of consuming different doses of alcohol on mortality. It was shown that occasional consumption (>0 to <1.3 g of ethanol per day) or low‑to‑moderate consumption (1.3–24 g of ethanol per day), as compared with lifetime nondrinkers, was not associated with increased risk of death (risk rate [RR], 0.96; 95% CI, 0.86–1.06 and RR, 0.93; 95% CI, 0.85–1.01, respectively). However, higher alcohol consumption (>25 g ethanol per day) was associated with an increased risk of death from any cause (5%–35% increased risk). Among women, higher alcohol consumption was more clearly associated with a risk of death from any cause.29 The results of this meta‑analysis indicated also that consuming low doses of alcohol did not reduce the risk of death, but confirmed that drinking up to 100 g of alcohol per week did not significantly increase the risk. A meta‑analysis of 83 studies30 including 599 912 current drinkers, showed that the risk of death from any cause was the lowest in people who drank around or below 100 g of alcohol per week. Alcohol consumption was roughly linearly associated with a higher risk of stroke (hazard ratio [HR] per 100 g per week of usual higher consumption, 1.14; 95% CI, 1.1–1.17), heart failure ([HF]; HR, 1.09; 95% CI, 1.03–1.15), fatal hypertensive disease (HR, 1.24; 95% CI, 1.15–1.33), and fatal aortic aneurysm (HR, 1.15; 95% CI, 1.03–1.28). Thus, despite the beneficial effect of drinking up to 100 g of alcohol per week on mortality, such consumption significantly increases the risk of selected cardiovascular diseases (CVDs).30 The results of this study indicate that the limits of alcohol consumption might be lower than those outlined in most current recommendations and guidelines. A very important information was provided by a study by Liu et al,31 covering 430 016 adults. It found that a gain of 1 year of life (+0.94 year) in the modest drinkers was erased by a 2- to 4‑fold increase in the risk of oral and esophageal cancer (HR, 2.35 and 3.84, respectively). Moreover, drinking more than the modest amounts led to a large reduction in life expectancy, by 6.86 years.
An umbrella review of 140 meta‑analyses of prospective studies32 analyzed the effect of alcohol consumption (low, moderate, and high, defined as ethanol intake of >0 and ≤14.9 g/day [>0 and <1 drink /day], 15–29.9 g/day [1–2.5 drinks/day], and ≥30 g/day [>2.5 drinks/day], respectively) on different health outcomes. It was found that low alcohol consumption, despite reducing the risk of death, was associated with a significant increase in the risk of esophageal cancer (RR, 1.47; 95% CI, 1.06–2.04), breast cancer (RR, 1.1; 95% CI, 1–1.2), basal cell carcinoma (RR, 1.23; 95% CI, 1.11–1.37), squamous cell carcinoma of the skin (RR, 1.15; 95% CI, 1.04–1.27), and subarachnoid hemorrhage (RR, 1.58; 95% CI, 1.03–2.44).32
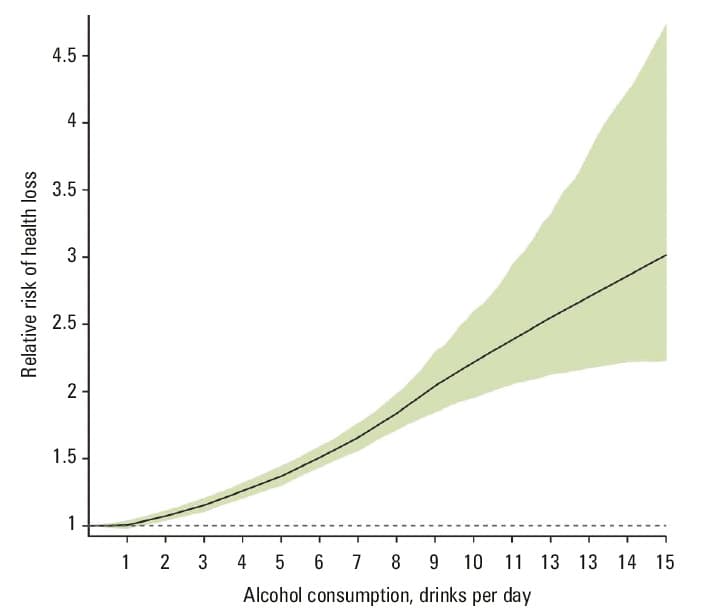
A meta‑analysis of 592 prospective and retrospective studies4 provided another very important observation, namely that there is no safe limit of drinking alcohol. This statement is in conflict with most recommendations, but the study showed that the risk of health loss increased significantly following consumption of 1 unit of alcohol per day (Figure 3).
Slightly different results were reported in a study by Ding et al,33 including 48 423 men and women with CVDs from the UK Biobank. After an observation period of 8.7 years, it was found that alcohol consumption was associated with all assessed outcomes in a J‑shaped manner relative to current nondrinkers, with a risk reduction that peaked at 7 g/day (RR, 0.79; 95% CI, 0.73–0.85) for all‑cause mortality, 8 g/day (RR, 0.73; 95% CI, 0.64–0.83) for cardiovascular mortality, and 6 g/day (RR, 0.5; 95% CI, 0.26–0.96) for cardiovascular events. The authors of the study indicated that the lowest risk of mortality and another cardiovascular event is likely to be associated with lower alcohol consumption up to approximately 105 g per week (or an equivalent to 13 UK units, with 1 unit equal to half a pint of beer / lager / cider, half a glass of wine, or 1 measure of spirits).33
The benefits of reducing alcohol consumption were demonstrated, among others, by Vaitkevičiūtė et al,34 who concluded that the alcohol control policies implemented between 2001 and 2020 reduced all‑cause mortality among men older than 20 years in the Baltic countries and in Poland. In this context, the results of a study by Yoo et al,35 which included 4 513 746 participants, are also noteworthy. This study analyzed the impact of changes in the amount of alcohol consumed on the risk of cancer, and found out that people who start consuming low, moderate, or high amounts of alcohol gradually increase their risk of cancer (HR, 1.03; 95% CI, 1–1.06; HR, 1.1; 95% CI, 1.02–1.18, and HR, 1.34; 95% CI, 1.23–1.45, respectively). In contrast, those who consumed low amounts of alcohol and stopped drinking it altogether had a lower risk of cancer (HR, 0.96; 95% CI, 0.92–0.99), similarly to those who consumed high amounts of alcohol and reduced the consumption to moderate or low (HR, 0.91; 95% CI, 0.86–0.97 and HR, 0.92; 95% CI, 0.86–0.98, respectively).35 It is also worth emphasizing that there is a reason why the recommendations indicate that the consumed doses of alcohol should not be accumulated. In a prospective study by Tian et al,36 including 918 529 participants followed for 12.65 years, it was found that binge drinking for 1 or more days a week was associated with a higher risk of mortality from all causes (HR, 1.15; 95% CI, 1.09–1.22), cancer (HR, 1.22; 95% CI, 1.1–1.35), and accidents (unintentional injuries) (HR, 1.39; 95% CI, 1.11–1.74).
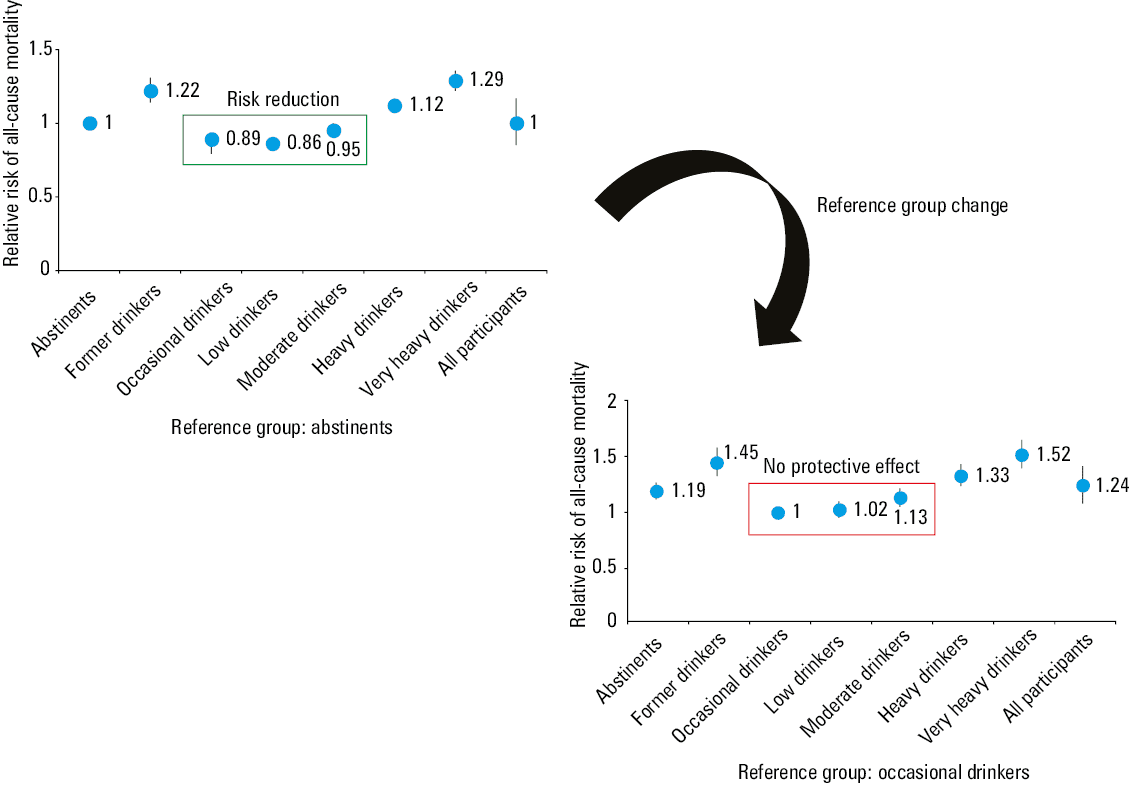
The results of this study are not unique. A meta‑analysis of 87 studies,37 covering 3 998 626 individuals, analyzed the impact of alcohol consumption and abstinence on the risk of death from any cause. It showed that low (1.3 to <25 g/day) and moderate (25 to <45 g/day) alcohol consumption reduced the risk of death from any cause when the reference group were teetotalers, but this effect was abolished when the reference group included occasional drinkers (Figure 4). A highly similar situation was described by Schutte et al,38 who followed 333 259 alcohol consumers and 21 710 never‑drinkers from the UK Biobank for 6.9 years. When the reference group were never‑drinkers, alcohol consumption reduced the risk of coronary artery disease (CAD) and cerebrovascular disease. The situation changed when the reference group included people from the 1st quartile of alcohol consumption, as then any beneficial effect of alcohol consumption was eliminated. Increased frequency of overall cardiovascular events was observed even for consumption below 14 units per week.38
It should be remembered that the results of observational studies do not allow for drawing definite conclusions. In a study by Biddinger et al,39 covering 371 463 participants from the UK Biobank, Mendelian randomization (approximating the possibility of causal inference) was performed to determine the impact of alcohol consumption on CVDs. It was shown that any alcohol consumption was associated with increased cardiovascular risk in the form of arterial hypertension (odds ratio [OR], 1.28; 95% CI, 1.18–1.39), CAD (OR, 1.38; 95% CI, 1.1–1.74), acute coronary syndrome (ACS; OR, 1.37; 95% CI, 1.05–1.78), stroke (OR, 1.26; 95% CI, 1.04–1.54), HF (OR, 1.39; 95% CI, 1.08–1.78), or atrial fibrillation (AF; OR, 1.24; 95% CI, 1.08–1.44). Similar observations were made by Lankester et al40 in a study involving 337 484 participants from the UK Biobank. It was found that 1 additional drink of alcohol per day was positively associated with systolic blood pressure (β = 2.65 mm Hg; 95% CI, 1.4–3.89), hemorrhagic stroke (OR, 2.25; 95% CI, 1.41–3.6), and AF (OR, 1.26; 95% CI, 1.07–1.48). A study using Mendelian randomization also allowed for a conclusion that alcohol consumption may contribute to shortening of telomeres, which significantly affects life expectancy and age‑related diseases.41
Different ways in which alcohol consumption affects health of the studied populations depend on numerous factors. However, socioeconomic status (highly industrialized vs poorer countries) is not one of them. In the context of potential confounding factors, the results of a meta‑analysis conducted by Probst et al,42 including 241 million women and 230 million men, should also be mentioned. It concluded that individuals along the entire continuum of socioeconomic statuses are evenly exposed to increased alcohol‑attributable mortality risk.
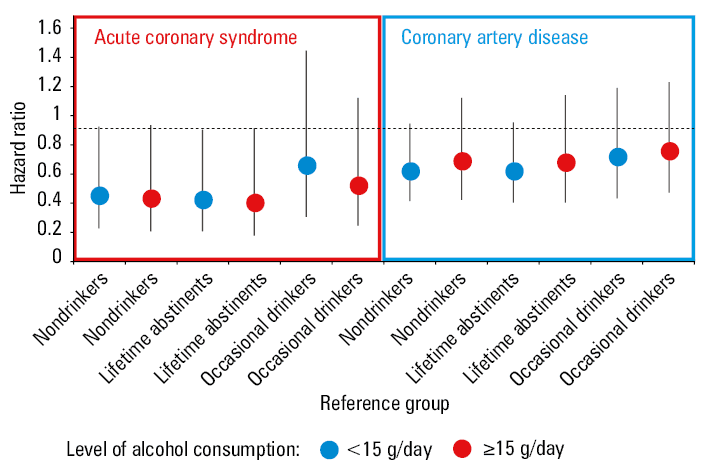
A limitation of some observational studies is a lack of distinction in the group of abstinents, that is, lifetime abstinents vs former heavy drinkers / current abstinents. The latter group may suffer long‑term health consequences of previous alcohol abuse. A study by Park et al,43 including 8330 participants followed for 10 years and classified as nondrinkers (0 g alcohol/day), drinker group 1 (<15 g alcohol/day), and drinker group 2 (≥15 g alcohol/day), analyzed the influence of alcohol consumption and abstinence on a risk of ACS or CAD. It was shown that a reduced risk of ACS or CAD could only be observed only in the group of abstinents and nondrinkers (Figure 5). A question arises why this was not demonstrated when the reference group was occasional drinkers? Perhaps this is because the teetotalers and nondrinkers were initially less healthy. The abovementioned factors limiting the results of observational studies may mean that in some of them the relationship between alcohol consumption and cardiovascular risk, which takes the shape of a J curve, may be a statistical artifact.
In summary, although low‑to‑moderate alcohol consumption reduced the risk of death, especially of CVDs, in some studies, even low consumption was associated with a greater risk of many other diseases. There is no proven safe amount of alcohol for the general population. It should also be emphasized that the threats related to alcohol consumption described above do not fully cover this issue, as alcohol consumption is associated with road accidents, accidents at work, crimes against health, and crimes against family members.
Alcohol and mortality: maybe the key is the type of alcohol?
When analyzing the impact of alcohol consumption on mortality and health outcomes, it is worth differentiating the type of alcohol. A study by Di Castelnuovo et al,44 covering 142 960 individuals, showed that among various types of alcohol, only wine consumption could reduce the risk of death from any cause (RR for spirits, 0.94; 95% CI, 0.88–1; RR for beer, 0.96; 95% CI, 0.9–1.03, and RR for wine, 0.87; 95% CI, 0.81–0.93). A meta‑analysis of 22 studies45 showed that wine consumption was associated with a lower risk of CAD (RR, 0.76; 95% CI, 0.69–0.84), CVD (RR, 0.83; 95% CI, 0.7–0.98), and cardiovascular mortality (RR, 0.73; 95% CI, 0.59–0.9). Similar findings were published for the risk of the most common arrhythmia, AF, which is especially frequent in the elderly.46-48 A meta‑analysis of 13 prospective studies,49 including 10 151 366 participants, showed that an increase in alcohol consumption of 1 drink per day elevated the risk of AF by 6% (RR, 1.06; 95% CI, 1.03–1.08). A study by Tu et al,50 of 403 281 middle‑aged individuals from the UK Biobank followed for 11.4 years, showed that virtually any amount of beer / cider or spirit increased the risk of AF. In the case of red and white wine, the risk of AF significantly increased in people drinking over >14 drinks per week.
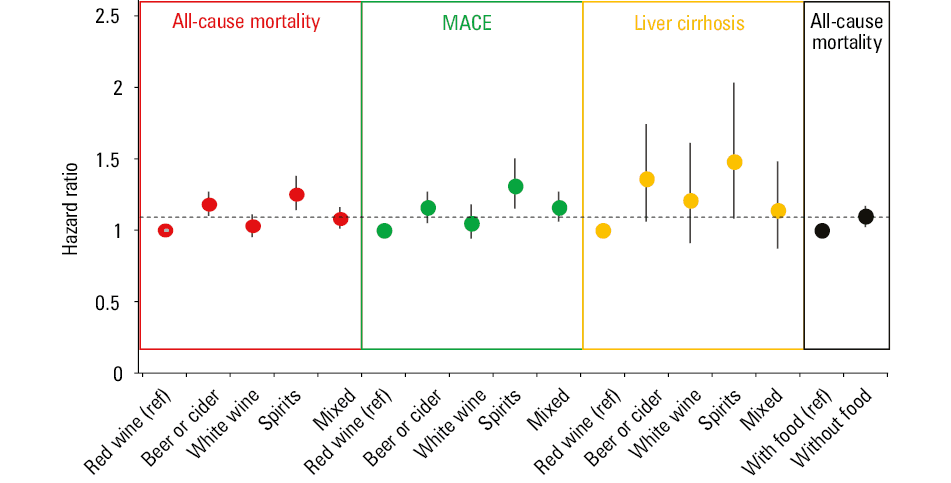
A prospective study by Jani et al,51 including 309 123 participants from the UK Biobank followed for 9 years, analyzed the effect of alcohol type on mortality and a risk of major adverse cardiovascular events (MACEs). It was shown that in comparison with people drinking red wine, those choosing beer or cider, spirits, or mixing different alcohols had a significantly higher risk of death (HR, 1.18; 95% CI, 1.1–1.27, HR, 1.25; 95% CI, 1.14–1.38, and HR, 1.08; 95% CI, 1.01–1.16, respectively). A similar effect was also found for MACE and liver cirrhosis (Figure 6).51 It is predicted that the number of deaths resulting from liver cirrhosis or liver cancer attributable to alcohol consumption will continue to increase.52
It is impossible not to mention the results of the already cited study by Schutte et al,38 which included 333 259 alcohol consumers and 21 710 never‑drinkers from the UK Biobank followed for 6.9 years. This study found that wine consumption was associated with a lower risk of cardiovascular events, while removing the effect on CAD from the model resulted in the cardioprotective effect of alcohol being eliminated.
Drinking wine is an ingrained element of some diets. For example, in France people do not go out “to drink” but “to dine”, and that is why the impact of alcohol on health should be considered in the context of a diet. The previously cited study by Jani et al51 found that drinking without a meal was associated with a higher risk of death from any cause (HR, 1.1; 95% CI, 1.02–1.17) than drinking with a meal (Figure 6). A study by Barbería‑Latasa et al,53 including 2226 participants, assessed the impact of Mediterranean alcohol‑drinking patterns (ie, with meals, in moderate amounts) and showed that strict adherence to such a pattern was associated with a reduced risk of death from any cause (HR, 0.54; 95% CI, 0.37–0.8). The key role of a diet in the context of alcohol consumption and mortality is also indicated by the results of a prospective study by Morales et al,54 which included 20 506 participants followed for 12.1 years. It was found that nonadherence to the Mediterranean diet and the Mediterranean alcohol‑drinking patterns was associated with a higher risk of death from any cause (HR, 2.02; 95% CI, 1.33–3.07).
Thus, of different types of alcohol, wine may have some health benefits, but its effect is strictly linked to the amount consumed and the quality of daily diet.
Mediterranean diet and wine
The essential features of the Mediterranean diet are abundance of plant‑based foods, olive oil, and fish and poultry. This is frequently accompanied by regular but low‑to‑moderate alcohol intake (particularly red wine with meals). Moreover, in the Mediterranean diet, the “philosophy of food” is very important, and it involves positive psychological and social effects associated with having meals with family / friends, eating small portions, and consuming fresh products.55,56
The benefits of the Mediterranean diet were found in a meta‑analysis of 30 prospective cohort studies (225 600 deaths).57 It showed that people following the Mediterranean diet had a significantly lower risk of death (RR, 0.79; 95% CI, 0.77–0.81). An analysis of individual components of the Mediterranean diet revealed that moderate alcohol consumption (in accordance with the principles of this diet) markedly contributed to reducing the risk of death (RR, 0.86; 95% CI, 0.77–0.97). A network meta‑analysis conducted by Karam et al58 and including 40 eligible randomized trials with 35 548 participants, investigated the impact of different types of diet on cardiovascular risk. It revealed that the Mediterranean diet was characterized by the greatest reduction in the risk of death from any cause (as compared with the following diets: low‑fat, very low‑fat, modified‑fat, combined low‑fat low‑sodium, Ornish, and Pritikin) (OR, 0.72; 95% CI, 0.56–0.92), and the risk of death from cardiovascular causes (HR, 0.55; 95% CI, 0.39–0.78), stroke (HR, 0.65; 95% CI, 0.46–0.93), and nonfatal ACS (HR, 0.48; 95% CI, 0.36–0.65). The results of this study indicated that the Mediterranean diet and wine (the most frequent type of alcoholic beverage consumed in traditional Mediterranean diet) should be treated jointly, as their health effects are a final manifestation of their various mechanisms of action.
Adopting the Mediterranean diet has a positive effect on cardiovascular risk also in patients with CVD risk factors and existing CVDs. In a study by Fan et al,59 including 8301 patients with metabolic syndrome from the National Health and Nutrition Examination Survey (2007–2018) followed for 6.3 years, the individuals who strictly adhered to the Mediterranean diet had a significantly lower risk of death from any cause (HR, 0.74; 95% CI, 0.64–0.86) and death from cardiovascular causes (HR, 0.65; 95% CI, 0.49–0.87). In this study, an analysis of dietary components showed a borderline significant beneficial effect of alcohol. A meta‑analysis of 7 prospective cohort studies60 including 37 879 patients with CVDs found out that those who followed the Mediterranean diet had a lower risk of death from any cause (HR, 0.85; 95% CI, 0.78–0.93) and borderline significantly reduced risk of death from cardiovascular causes (HR, 0.91; 95% CI, 0.82–1.01).
A multicenter, randomized study by Estruch et al,61 which included 7447 participants at a high cardiovascular risk, compared the Mediterranean diet (allowing, eg, for wine consumption in habitual drinkers ≥7 glasses/week with meals) supplemented with extra‑virgin olive oil or nuts with a low‑fat diet. After 4.8 years of observation, the individuals assigned to the Mediterranean diet had by 30% (HR, 0.7; 95% CI, 0.55–0.89) lower risk of major cardiovascular events (myocardial infarction, stroke, or death from cardiovascular causes). The Mediterranean diet is also beneficial in other groups of patients. A meta‑analysis of 8 cohort studies,62 covering 514 816 participants and 33 576 deaths, found that following the Mediterranean diet was associated with a significant reduction in overall mortality (9%), mortality from CVDs (9%), incidence of or mortality from cancer (6%), and incidence of Parkinson disease and Alzheimer disease (13%). It is also worth emphasizing the results of a meta‑analysis of 117 studies,63 covering 3 202 496 participants, which concluded that adherence to the principles of the Mediterranean diet was associated with a lower risk of cancer mortality (RR, 0.87; 95% CI, 0.82–0.92), all‑cause mortality among cancer survivors (RR, 0.75; 95% CI, 0.66–0.86), breast cancer (RR, 0.94; 95% CI, 0.9–0.97), colorectal cancer (RR, 0.83; 95% CI, 0.76–0.9), head and neck cancer (RR, 0.56; 95% CI, 0.44–0.72), respiratory system cancer (RR, 0.84; 95% CI, 0.76–0.94), gastric cancer (RR, 0.7; 95% CI, 0.61–0.8), bladder cancer (RR, 0.87; 95% CI, 0.76–0.98), and liver cancer (RR, 0.64; 95% CI, 0.54–0.75). The Mediterranean diet is also beneficial in patients with metabolic dysfunction–associated fatty liver disease (MAFLD). A meta‑analysis of 3037 MAFLD patients64 revealed that the Mediterranean diet reduced activity of alanine aminotransferase and aspartate aminotransferase, and lowered fatty liver index, hepatic steatosis, and liver stiffness. The Mediterranean diet is also beneficial for patients with gastroesophageal reflux disease.65
Thus, following the Mediterranean diet provides numerous health‑promoting effects, which are very well documented. Therefore, the European Society of Cardiology recommends adopting the Mediterranean or similar diet to lower the risk of CVD (class of recommendation, I; level of evidence, A).23
A treasure hidden in wine: polyphenols
Polyphenols are important phytochemicals with strong antioxidant activity, found in plant‑based foods. They are present not only in wine but also in coffee, tea, fruit (oranges, cherries, apples, etc.), and vegetables (olives, spinach, potatoes, etc.). Coffee and tea also have health‑promoting properties, including cardioprotective ones.61,66 Consuming polyphenols in various food products is an important method of cardiovascular prevention.67-70
At this point, it is worth mentioning the “French food paradox” described by Dr Serge Renaud in 1992.71 Interestingly, the climate of France, unlike of Spain, is not Mediterranean at all. France is dominated by the Atlantic and continental climate, and the Mediterranean climate is mainly limited to the Côte d’Azur. Moreover, the French diet is different from that in the other Mediterranean countries (higher meat consumption, including beef, higher cheese and butter consumption, and smaller amount of olive oil in the diet). Another difference is that in France more wine is consumed than in Spain and Italy (in Spain and Croatia beer consumption predominates, while in Italy the most commonly drank alcohol is wine, but in smaller quantities).72 The higher the consumption of saturated fat and cholesterol, the greater the risk of death from CAD.23 France does not follow this pattern, as people there consume a significant amount of saturated fats and cholesterol, and still the CAD mortality rate is significantly lower than, for example, in Spain, where the consumption of saturated fats and cholesterol in the diet is several times lower.71 In France, the number of deaths from cardiovascular causes is lower than in Spain (women, 221.9 vs 279.9/100 000; men, 202.3 vs 246.1/100 000).73 This effect is probably due to many factors that are not limited to the amount of wine consumed and the daily diet. A good example is Norway. In Norway, cardiovascular mortality is at a similar level to that in Spain (women, 223.2/100 000; men, 194.8/100 000),73 and much less alcohol is consumed there. Nevertheless, the Health Index Score is much higher in Norway than in Spain (83 vs 79.7),74 which may explain these differences to some extent. This epidemiologic difference in France (French paradox) could be explained by the large amount of wine consumed and the health‑promoting effects (Figure 7) of numerous polyphenols it contains.75-84 The concept of the French paradox should be approached with caution. The most common cause of death in the French people is cancer, which may be related to the fact that their life expectancy is one of the longest in Europe,85 and that the incidence of cancer increases with age.86 Nevertheless, it is known that even small doses of alcohol are carcinogenic and increase the risk of various cancers.32 Moreover, the French diet is rich in cheese, including blue cheese. Blue cheeses contain carcinogenic aflatoxins.87 Thus, the French paradox should be analyzed in the context of a number of factors.
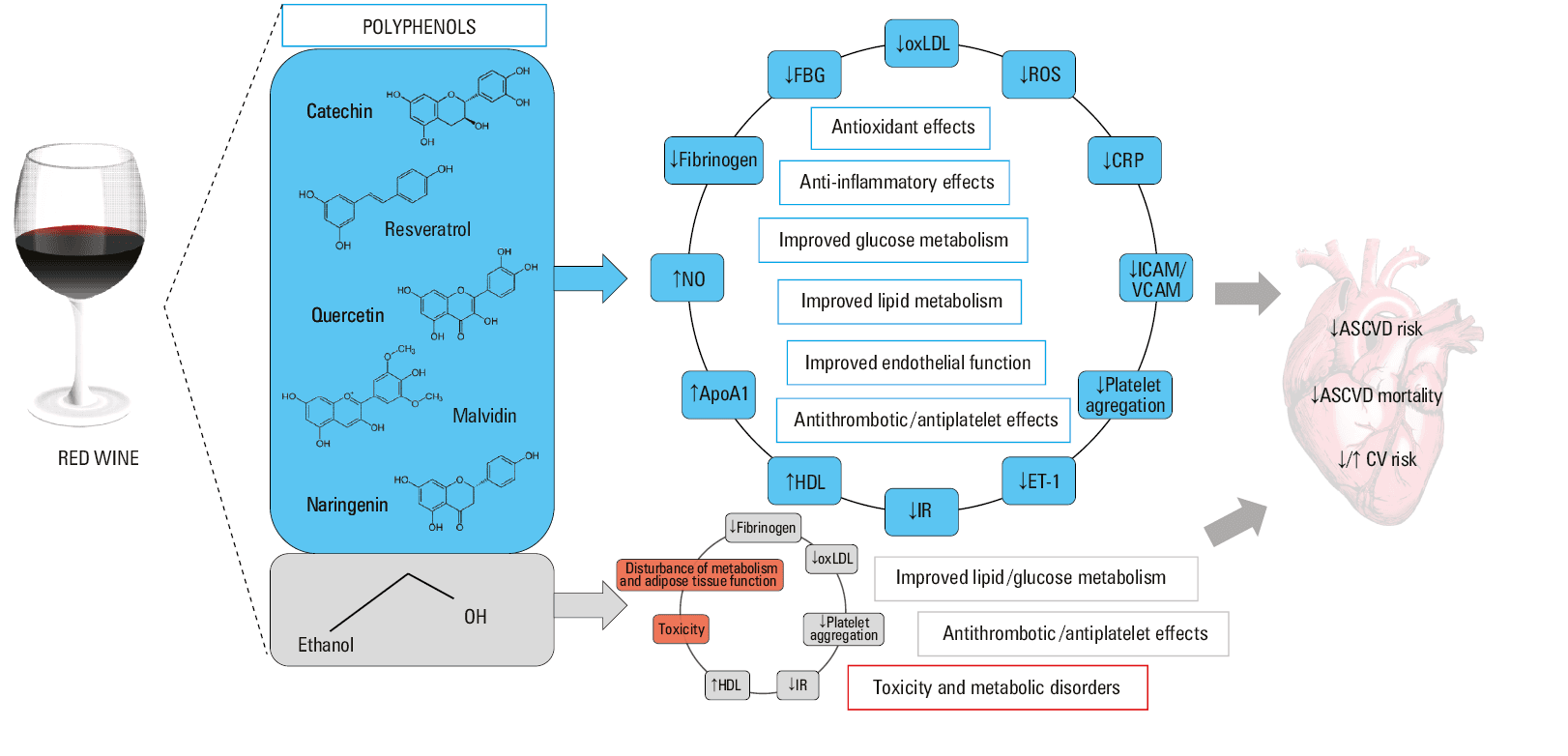
Abbreviations: ApoA1, apolipoprotein A1; ASCVD, atherosclerotic cardiovascular disease; CRP, C‑reactive protein; CV, cardiovascular; ET‑1, endothelin 1; FBG, fasting blood glucose; HDL, high‑density lipoprotein; ICAM, intercellular adhesion molecule; IR, insulin resistance; NO, nitric oxide; oxLDL, oxidized low‑density lipoprotein; ROS, reactive oxygen species; VCAM, vascular cell adhesion molecule
Red wine contains many chemical compounds, the most important of which are polyphenols. They are present primarily in the grape skin, seeds, and stalk, hence they are abundant in red wine and absent in most white wines that are made without skin maceration. Polyphenols include nonflavonoid compounds including hydroxybenzoic acids, hydroxycinnamic acids, stilbenes (resveratrol), and flavonoids (flavones, flavan‑3‑ols, flavonols, and anthocyanins).78 These compounds could be responsible for the health‑promoting properties of wine. A study by Bondonno et al,88 including 55 786 women from the Nurses’ Health Study and 29 800 men from the Health Professionals Follow‑up Study, found that the consumption of flavonoids contained in red wine was associated with a reduced risk of death by 4% (HR, 0.96; 95% CI, 0.93–0.99). Another study by Vázquez‑Ruiz et al,89 including 16 147 Spanish participants free of CVD followed for 12.2 years, assessed the impact of the amount of polyphenols consumed in the diet on the risk of CVD. It showed that suboptimal intake of phenolic compounds was independently associated with a higher risk of CVD (HR, 1.85; 95% CI, 1.09–3.16). In a meta‑analysis of 37 studies conducted by Weaver et al,90 consumption of wine polyphenols was associated with significant improvement in systolic blood pressure (−2.6 mm Hg; 95% CI, −4.8 to −0.4). An important polyphenol of red wine, resveratrol, significantly affects lipid profile and glucose metabolism. In their meta‑analysis of 1171 participants, Zhou et al91 reported that resveratrol significantly decreased waist circumference (standard mean difference [SMD], –0.36; 95% CI, –0.59 to –0.14), and the levels of hemoglobin A1c (SMD, –0.48; 95% CI, –0.69 to –0.27), total cholesterol (SMD, –0.15; 95% CI, –0.3 to –0.01), and low‑density lipoprotein cholesterol (SMD, –0.42; 95% CI, –0.57 to –0.27). Another study worth mentioning is one by María Mérida et al,92 covering 12 161 individuals observed for 12.5 years. It demonstrated that the consumption of various polyphenols (dihydroflavonols, flavonols, methoxyphenols, tyrosols, alkylmethoxyphenols, hydroxycinnamic acids, and hydroxyphenilacetic acids) was associated with a 20% lower all‑cause mortality risk and a 40% lower cardiovascular mortality risk over time. The PREDIMED randomized clinical trial by Tresserra‑Rimbau et al,93 which included 7447 participants followed for 4.8 years, found that higher polyphenol intake was associated with a 37% reduction in the risk of all‑cause mortality (HR, 0.63; 95% CI, 0.41–0.97). Moreover, among the polyphenol subclasses, stilbenes and lignans were significantly associated with reduced all‑cause mortality (HR, 0.48; 95% CI, 0.25–0.91 and HR, 0.6; 95% CI, 0.37–0.97, respectively). A meta‑analysis of 46 randomized clinical trials94 including 2494 participants showed that the consumption of polyphenols was associated with significantly reduced systolic blood pressure (−3.69 mm Hg; 95% CI, −4.24 to −3.15 mm Hg), diastolic blood pressure (−1.44 mm Hg; 95% CI, −2.56 to −0.31 mm Hg), waist circumference (−3.04 cm; 95% CI, −7.06 to −0.98 cm), total cholesterol (−9.03 mg/dl; 95% CI, −16.46 to −1.06 mg/dl) and triglycerides (−13.43 mg/dl; 95% CI, −23.63 to −3.23 mg/dl).
To sum up, polyphenols contained in wine (but also in fruit, coffee, or tea) are characterized by well‑documented multidirectional health‑promoting effects.
Conclusions
History of wine consumption started in the Neolithic period, although other fruits might have been exploited earlier for fermented beverages. However, humans soon realized the harmful consequences of alcohol consumption. Excessive alcohol consumption is still considered a major cause of mortality in the world. Therefore, every effort should be made to reduce the number of people consuming excessive amounts of alcohol, which is an independent risk factor for CVD and other diseases.95-102 Ideally, alcohol consumption should be zero at the population level, although this would be difficult to achieve taking into account the long history of alcohol presence in human diet. Moreover, most observational studies indicate a reduction in the risk of CVD associated with a small‑to‑moderate alcohol consumption, especially in the Mediterranean diet model. The cardiovascular benefits of drinking moderate amounts of red wine demonstrated in various studies are due to numerous polyphenols it contains, but these chemicals can also be found in other food products. Therefore, people should be comprehensively educated on the types of alcohol consumed and maximum permissible doses. In some patients, alcohol consumption is completely prohibited due to comorbidities.
- Surma S, Więcek A. Alcohol and health. Is regular drinking of small doses of alcohol really good for your health? Arch Med Sci Atheroscler Dis. 2022; 7: 49‑59. | Crossref
- Harding J, Robinson J, Thomas TQ, eds. The Oxford Companion to Wine. 4th ed. Oxford University Press; 2023.
- Wnuk M, Purandare B, Marcinkowski J. Structure of alcohol consumption in Poland in a historical perspective [in Polish]. Probl Hig Epidemiol 2013; 94: 446‑50.
- GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990‑2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2018; 392: 1015‑1035.
- Manthey J, Shield KD, Rylett M, et al. Global alcohol exposure between 1990 and 2017 and forecasts until 2030: a modelling study. Lancet. 2019; 393: 2493‑2502. | Crossref
ARTICLE INFORMATION