Atrial fibrillation, comorbidities, stroke, and mortality in real-world clinical practice



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Atrial fibrillation, comorbidities, stroke, and mortality in real-world clinical practice
Atrial fibrillation (AF) is a cardiac arrhythmia whose prevalence is increasing due to aging of the population. It is frequently associated with comorbidities, such as heart failure (HF), chronic kidney disease (CKD), cognitive impairment, diabetes, hypertension, and other diseases, which modulate its clinical course and contribute to adverse outcomes associated with this arrhythmia.1
Detection of AF is a key component of the holistic approach to patient care according to the Atrial fibrillation Better Care (ABC) pathway proposed by the current guidelines.2,3 Indeed, it is noteworthy that the risk of stroke associated with AF is not different for symptomatic and asymptomatic patients.1,4 Thus, early detection of AF and subsequent appropriate prescription of anticoagulants in the patients at a risk of thromboembolism has a potential to substantially reduce the rate of stroke and morbidity.4
The possibility to detect AF varies depending on the extent of rhythm monitoring, and new mobile health solutions5 available nowadays complement the more traditional Holter electrocardiography (ECG).6 In particular, mobile health devices are validated both in monitoring and screening scenarios.5,7 The accuracy of these devices differs according to the type of the device itself, technology used, monitoring time, and the target population. In this context, simplicity and widespread availability of these technologies should be considered in combination with their accuracy, and physicians need to choose the correct device for each patient in that particular context.8 High sensitivity and specificity values have been reported for both photoplethysmography (PPG)-based and ECG‑based devices.5 The former use an optical technique that is easy to use and widely available. The latter, however, are capable of monitoring and transmitting an ECG trace, which is sufficient to diagnose AF, while the results of a PPG examination require further confirmation to establish a definite diagnosis.8 According to the guidelines, diagnosing AF requires an ECG documentation in the form of a standard 12‑lead ECG recording or a single‑lead ECG tracing of at least 30 seconds showing heart rhythm with no discernible repeating P waves and irregular RR intervals (when atrioventricular conduction is not impaired), confirmed by a cardiologist.
In the present issue of Polish Archives of Internal Medicine, Mitręga et al9 report on 1‑year follow‑up results of the NOMED‑AF (Noninvasive Monitoring for Early Detection of Atrial Fibrillation) study. NOMED‑AF was a study including around 3000 Polish citizens aged 65 years old or older, who underwent up to 30 days of continuous ECG monitoring. Of note, the study adopted a strategy based on intensification of monitoring, as compared with standard practice, in order to increase the ability to detect AF in individuals at risk. Through ECG monitoring and clinical evaluation, AF was found in up to 19.2% of the participants; of those 4.1% were patients with newly diagnosed AF.10 Among the patients with AF, one‑third were not treated with anticoagulants, which is a rather high proportion. This finding requires further investigation and indicates the need for a more extensive implementation of consensus guidelines and the ABC pathway.2
In the current study, the authors report on 1‑year outcomes of 2795 patients enrolled in NOMEAD‑AF with available follow‑up data.9 Of those, 22.1% had AF. In the whole cohort, the factors associated with cardiovascular hospitalization were AF, a history of myocardial infarction, peripheral artery disease, and diabetes. Moreover, AF was an independent risk factor for death, together with CKD and age of at least 65 years. Treatment with oral anticoagulants was associated with a lower risk of death and stroke, even if the interpretation of this finding has to be considered in the context of the observational nature of the study. The cohort included also 125 patients with de novo diagnosed AF, and this subgroup (particularly women) was at a relatively higher risk of stroke and also of death. These findings should be interpreted considering the low prescription rate of oral anticoagulants in the case of a first diagnosis of AF, and this observation, which is not in line with the current guidelines, has been confirmed by a series of studies.3,11 Moreover, we should also consider that physicians may underestimate the risk associated with de novo AF or first‑diagnosed AF despite the evidence that atrial arrhythmias may recur or progress during follow‑up.11,12
Mitręga et al9 reported that 6.7% of the AF patients died and 3.8% had a stroke during 1‑year follow‑up. These data highlight the important clinical impact of AF, and the extent to which it is associated with hard clinical outcomes, such as death or stroke, which per se represent also a heavy financial burden on health care services and societies.
Considering that AF is a chronic condition, extended follow‑up of this cohort (3–5 years) would be highly valuable, as it would allow for testing the effect of the interaction between AF and comorbidities (either present at baseline or developed over time) on clinical outcomes. It would also enable evaluation of long‑term clinical trajectories of patients with and without AF. There is a complex interplay between AF and a series of comorbidities, which has important implications on patient outcomes (Figure 1). Moreover, it would be interesting to assess whether early rhythm control interventions, such as catheter ablation and / or antiarrhythmic drugs, are effective also in the subset of patients with a higher burden of comorbidities.13
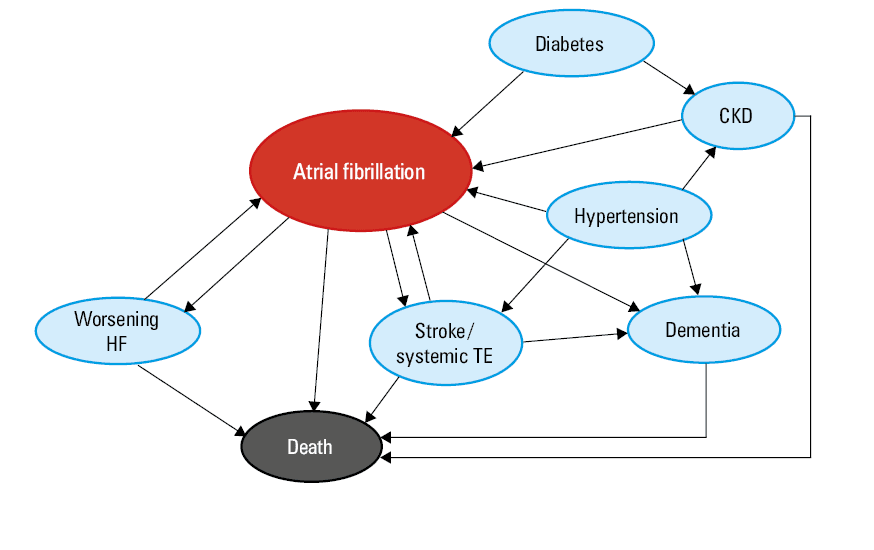
Abbreviations: CKD, chronic kidney disease; HF, heart failure; TE, thromboembolism
The study by Mitręga et al9 shows that AF, and particularly the AF type, directly modulates a patient’s clinical course. Of note, AF has a tendency to cluster with comorbidities, which increases the risk of adverse outcomes and influences clinical management.14 In a recent study on 10 169 European patients, 40.5% of the participants had at least 1 feature of clinical complexity (defined as a history of bleeding, CKD, or frailty). Having a feature of clinical complexity was associated with multimorbidity, frailty, and polypharmacy on one hand, and with less frequent prescription of oral anticoagulation on the other. Moreover, a history of bleeding, frailty, CKD, and presence of at least 2 of these features were associated with a higher risk of worse clinical outcomes (a composite of all‑cause death, major adverse cardiovascular events, and major bleeding).14
In fact, AF, similarly to other chronic conditions, is associated with multiple clinical presentations and / or comorbidities, and requires complex integrated multidisciplinary care, with the aim to address the multifaceted nature of this disease and also to predict, prevent, and treat incident comorbidities. Of note, a holistic approach to AF patient care has proven effective also in selected subgroups of patients, such as those with cancer.15 Indeed, adherence to the ABC pathway was found to be associated with a significantly lower occurrence of the composite end point of all‑cause death, major adverse cardiovascular events, and major bleeding, as compared with nonadherence, both in the patients with and without cancer. Moreover, complying with a higher number of criteria was associated with an incremental benefit.15
Increasing age, incident comorbidities, and adverse outcomes highlight that the clinical course of patients with AF is dynamic, and that patient risk stratification should follow the same principle. In this regard, artificial intelligence (AI) offers a new opportunity to deliver dynamic, comprehensive, and personalized assessment of disease trajectories by an integrated analysis of a large amount of data from multiple sources, with the aim to improve patient outcomes. Recent AI models showed good performance in predicting incident AF, but also recurrence of AF after rhythm control interventions, success of electrical cardioversion, and incident HF. Clinical implementation of accurate, interpretable, generalizable, and reliable AI tools might in the future improve risk prediction, thus allowing physicians to deliver better and more personalized patient care; however, appropriate evaluations according to the rules of evidence‑based medicine are required also in this emerging field.
- Boriani G, Bonini N, Vitolo M, et al. Asymptomatic vs. symptomatic atrial fibrillation: clinical outcomes in heart failure patients. Eur J Intern Med. 2024; 119: 53‑63. | Crossref
- Imberti JF, Mei DA, Vitolo M, et al. Comparing atrial fibrillation guidelines: focus on stroke prevention, bleeding risk assessment and oral anticoagulant recommendations. Eur J Intern Med. 2022; 101: 1‑7. | Crossref
- Lip GYH, Proietti M, Potpara T, et al. Atrial fibrillation and stroke prevention: 25 years of research at EP Europace journal. Europace. 2023; 25: euad226. | Crossref
- Kalarus Z, Mairesse GH, Sokal A, et al. Searching for atrial fibrillation: looking harder, looking longer, and in increasingly sophisticated ways. An EHRA position paper. Europace. 2023; 25: 185‑198. | Crossref
- Bonini N, Vitolo M, Imberti JF, et al. Mobile health technology in atrial fibrillation. Expert Rev Med Devices. 2022; 19: 327‑340. | Crossref
ARTICLE INFORMATION