Previous hepatitis E virus infection is associated with increased liver stiffness in patients with autoimmune hepatitis
Key words: autoimmune hepatitis, elastography, hepatitis E virus, liver fibrosis

 CC BY 4.0
CC BY 4.0
Previous hepatitis E virus infection is associated with increased liver stiffness in patients with autoimmune hepatitis
Introduction: Autoimmune hepatitis (AIH) is a chronic, progressive liver disease that, in most cases, may require lifelong immunosuppression. Hepatitis E virus (HEV) is a leading cause of acute, typically self‑limited hepatitis worldwide, although immunocompromised patients may develop chronic hepatitis.
Objectives: We aimed to evaluate the impact of HEV seropositivity on the clinical course of AIH.
Patients and methods: The study involved a group of 374 adult patients with AIH (68% women; median [interquartile range] age, 34 [18–83] years; 38% with liver cirrhosis). Serum anti‑HEV immunoglobulin (Ig) G and IgM antibodies were measured by enzyme‑linked immunosorbent assay, liver fibrosis was assessed by liver stiffness measurement (LSM), and liver cirrhosis was confirmed with liver histology or LSM.
Results: Fifty‑five patients (15%) with AIH were anti‑HEV IgG‑positive. These patients were older (P <0.001), had higher body mass index, and higher value of LSM (both P <0.05). In a multivariable model including the levels of alanine aminotransferase and IgG, the HEV seropositive status was associated with an increased risk of advanced liver fibrosis with odds ratio of 3.69 (95% CI, 1.26–10.77; P = 0.02), as reflected by liver stiffness equal to or above 10.5 kPa. Anti‑HEV IgG seropositivity was, however, not linked with the type of treatment or worse AIH outcome. Seroprevalence of anti‑HEV IgGin the patients with AIH was lower than in the general population of Polish blood donors (43%).
Conclusions: Previous HEV infection in patients with AIH is associated with more advanced liver fibrosis. However, the overall seroprevalence of anti‑HEV IgG is lower in patients with AIH than in blood donors in Poland.
What's new?
Hepatitis E virus (HEV) is recognized globally as a leading cause of acute hepatitis, which is typically self‑limited. However, in immunocompromised individuals, it may progress to chronic hepatitis. In our study, involving 374 patients with autoimmune hepatitis (AIH), seroprevalence of anti‑HEV immunoglobulin (Ig) G was 15%. This prevalence was notably higher in older patients, those with higher body mass index, and those exhibiting more advanced liver fibrosis. We showed a considerable impact of HEV on the progression of AIH, with a 3.69‑fold increase in the risk of advanced fibrosis according to multivariable analysis. Overall, seroprevalence of anti‑HEV IgG among the study participants was lower than reported previously in Polish blood donors.
Introduction
Autoimmune hepatitis (AIH) is a chronic liver disease whose incidence and prevalence have been consistently increasing worldwide over time, with higher rates observed in women than men.1 The incidence and prevalence of AIH among adults in Poland are not precisely established; however, they are estimated at 1.8 and 23.1 per 100 000 people, respectively.1 The clinical course of AIH varies from asymptomatic to liver failure.2 A characteristic presentation includes icteric acute hepatitis, presence of antibodies, hypergammaglobulinemia, and typical histologic findings.3 An absence of viral hepatitis, mainly cytomegalovirus (CMV), hepatitis A virus, hepatitis B virus (HBV), and hepatitis C virus (HCV), represents 1 of the 4 factors included in simplified diagnostic criteria for AIH.3,4 Treatment is based on steroids and azathioprine, and most patients require lifelong immunosuppression,2 which may increase the risk of infectious complications.
Pathogenesis of AIH has not been fully elucidated. However, it is believed that an unknown factor triggers a loss of self‑tolerance to liver autoantigens in patients with AIH, leading to self‑perpetuated liver inflammation.2 Common viral infections with, for example, CMV, Epstein–Barr virus, herpes simplex virus (HSV), HBV, HCV, and hepatitis E virus (HEV), have been suggested as potential precipitating factors for AIH.2,5,6 This association might be attributed to molecular mimicry between immunogenic antigens (ie, nuclear, smooth muscle, and liver kidney microsome type 1 antigen) and HSV, HBV, or HCV. Still, none of these viruses has been definitively identified as a cause of autoimmune hepatitis.6,7
HEV infection is the most common cause of acute viral hepatitis worldwide, which affects approximately 20 million people each year, mostly in developing countries through contaminated water.8,9 In developed countries, including those in Europe and North America, HEV affects immunocompromised patients through zoonotic transmission, primarily due to consumption of undercooked, contaminated meat, and might lead to chronic hepatitis.8 Immunoglobulin (Ig) G seroprevalence analysis is a standard method to assess past and present infections in a community.9 Prevalence of anti‑HEV IgG in Europe varies from 0.6% to 52.5%10; a relatively high prevalence of 43% was reported in Polish blood donors.11
The impact of HEV infection on patients with AIH was analyzed in several studies, yielding inconsistent results. Seroprevalence of anti‑HEV IgG antibodies reported at 7.7% to 40% varied across European regions.12-15 These rates were typically higher than those observed in the general population. The relationship between anti‑HEV IgG seropositivity and liver fibrosis has also been explored, though with varying methodologies and inconclusive findings. Notably, Eder et al13 observed a trend toward higher prevalence of cirrhosis (42% vs 21%; P = 0.053) in anti‑HEV IgG‑positive patients with AIH. Furthermore, a recent study on nonalcoholic fatty liver disease (NAFLD) demonstrated an association between anti‑HEV IgG seropositivity and increased liver stiffness measurements (LSMs), as well as liver cirrhosis.16
HEV may act as a potential trigger of AIH (acute hepatitis) or as a hypothetical modulator of clinical course (chronic hepatitis). The aims of the study were: 1) to evaluate the impact of previous HEV infections on AIH course, 2) to study a potential link between anti‑HEV IgG status and liver fibrosis, and 3) to quantify the seroprevalence of anti‑HEV antibodies in adult Polish patients with AIH.
Patients and Methods
Study population
A group of 379 Polish adult patients with AIH was recruited at the Department of Hepatology, Transplantology and Internal Medicine of the Medical University of Warsaw between 2015 and 2019. A diagnosis of AIH was established according to the current European guidelines,17 and liver biopsy was obligatory at the time of diagnosis. Patients with active or past HBV (tested as HBs antigen and HBc antibodies) or HCV (tested as anti‑HCV antibodies) infections and those who tested positive for the anti‑HEV IgM antibodies as well as liver transplant recipients were excluded from further analyses. A local ethics committee approved the study protocol (KB/128/2015) developed according to the ethical guidelines of the 1975 Declaration of Helsinki (latest revision, 2013), and written informed consent was obtained from all participants.
Clinical variables and liver fibrosis assessment
Fasting venous blood samples were collected for tests (including blood count, biochemical tests, and serologic markers), as a part of regular standard of care at the Department of Hepatology, Transplantology, and Internal Medicine of the Medical University of Warsaw, Poland. Complete biochemical response was defined as serum alanine aminotransferase (ALT) and IgG levels within the reference ranges.18 Liver fibrosis was assessed on the day of enrolment to the study by LSM and fibrosis‑4 (FIB‑4) serum fibrosis index. Liver and spleen stiffness was measured using 2‑dimensional shear wave elastography (Aixplorer, SuperSonic Imagine, Aix‑en‑Provence, France), as presented previously.19 We used cutoffs of 10.5 kPa and 16 kPa for advanced liver fibrosis and liver cirrhosis, respectively.19 FIB‑4 was calculated according to Sterling et al,20 and a cutoff of 2.67 was used to define patients at risk of advanced liver fibrosis.21
Testing for hepatitis E infection markers
Detection of anti‑HEV IgG- and IgM‑specific antibodies was performed at the Department of Medical Biology (Pomeranian Medical University, Szczecin, Poland) by enzyme‑linked immunosorbent assay (ELISA; Euroimmun Medizinische Labordiagnostika AG, Luebeck, Germany). The antigen for this test included recombinant structural proteins of the HEV (genotypes 1 and 3), and the test was calibrated using the World Health Organization reference serum (reference reagents HEV antiserum, human, 1st IS NIBSC Code 95/584). The assays were used according to the manufacturer’s instructions. Out of 379 patients tested using ELISA, 5 (1%) were positive for anti‑HEV IgM. To avoid bias due to possible acute HEV infection, these anti‑HEV IgM‑positive patients were excluded, as illustrated in Figure 1. The aim of this study was to evaluate the impact of a previous HEV infection (indicated by anti‑HEV IgG positivity) on the clinical course of AIH. Thus, the analysis proceeded with the remaining 374 patients, all of whom were anti‑HEV IgM‑negative, as shown in Figure 1.
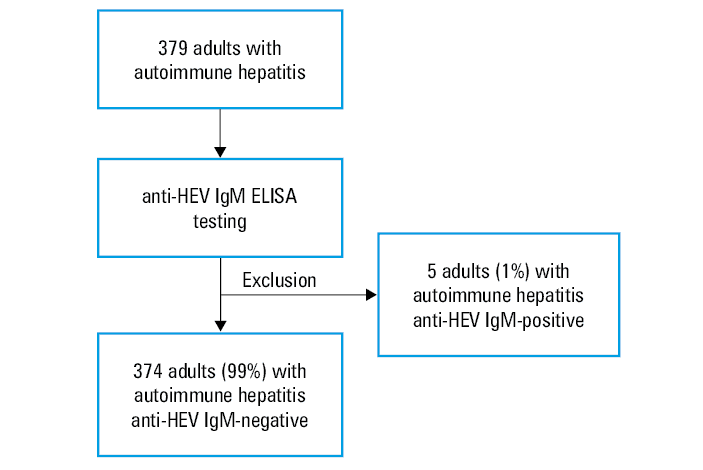
Abbreviations: ELISA, enzyme‑linked immunosorbent assay; HEV, hepatitis E virus; Ig, immunoglobulin
Statistical analysis
Statistical analyses were performed using SPSS software version 27.0 (SPSS Statistics, IBM Corporation, Armonk, New York, United States) and GraphPad Prism package, version 10.1.1 (GraphPad Software, Boston, Massachusetts, United States). Continuous variables are shown as median with interquartile range (IQR; not normally distributed), and categorical variables are expressed as absolute and relative (%) frequencies. The Kolmogorov–Smirnov test was applied to determine whether the continuous variables were normally distributed. The Wilcoxon Mann–Whitney test was used to analyze continuous variables. The χ2 and Fisher exact tests were used to compare categorical variables. Logistic regression analyses tested the associations between anti‑HEV IgG status and clinical data. All statistical tests were 2‑sided, and P values below 0.05 were treated as significant.
Results
Clinical characteristics of the study cohort
Baseline characteristics of the AIH study cohort are presented in Table 1. Of 374 patients, 68% were women, and a median (IQR) age of the patients was 34 (18–83) years. A diagnosis of AIH was established at a median (IQR) age of 27 (3–83) years, and liver cirrhosis was present in 23% of the patients at the time of the diagnosis. More than half of the cohort (53%) was diagnosed before the age of 30 years. Median (IQR) liver stiffness was 11 (4–74) kPa. In 183 patients (49%), the LSM was equal of above 10.5 kPa, suggesting advanced liver fibrosis. The median (IQR) model of end stage liver disease (MELD) score was 8 (6–37) points, and 39 patients (10%) had a MELD score above 15 points. Most of the patients in the study group (73%) were on azathioprine with or without steroids, 21% received none immunosuppressive therapy at inclusion, and 6% were on mycophenolate mofetil with or without calcineurin inhibitors and steroids.
Parameter | Whole cohort (n = 374) | anti‑HEV IgG (+) (n = 55) | anti‑HEV IgG (–) (n = 319) | P value |
All quantitative data are shown as median and interquartile range.
The χ2 and Wilcoxon Mann–Whitney tests were used to compare the subgroups and P <0.05 was considered as significant.
a Reference range <55 U/l
b Reference range, 70–400 mg/dl
c Reference range, 800–1600 mg/dl
d Reference range, 50–280 mg/dl
SI conversion factors: to convert immunoglobulin A, G, and M to g/l, multiply by 0.01.
Abbreviations: ALT, alanine aminotransferase; BMI, body mass index; MELD, model of end stage liver disease; others, see Figure 1 | ||||
Age at inclusion, y | 34 (18–83) | 43 (18–73) | 32 (18–83) | <0.001 |
Age at diagnosis, y | 27 (3–83) | 38 (10–72) | 26 (3–83) | <0.001 |
Women, n (%) | 256 (68) | 40 (72) | 216 (68) | 0.53 |
BMI, kg/m2 | 23 (16–41) | 25 (18–34) | 23 (16–41) | 0.047 |
ALT, U/la | 55 (8–3400) | 55 (15–930) | 57 (8–3400) | 0.7 |
Immunoglobulin A, mg/dlb | 233 (3–1480) | 260 (70–1054) | 230 (3–1480) | 0.047 |
Immunoglobulin G, mg/dlc | 1488 (318–6508) | 1592 (567–3490) | 1466 (318–6508) | 0.62 |
Immunoglobulin M, mg/dld | 159 (14–1035) | 166 (27–904) | 156 (14–1035) | 0.58 |
Spleen length, cm | 12 (8–25) | 13 (8–22) | 12 (8–25) | 0.06 |
MELD, points | 8 (6–37) | 8 (6–34) | 8 (6–37) | 0.99 |
The HEV serologic status was assessed in a median (IQR) of 4 (0–32) years after the diagnosis. Fifty‑five (15%) patients in the entire cohort were anti‑HEV IgG‑positive. Among patients recruited at the moment of AIH diagnosis (n = 105), 20% were positive for anti‑HEV IgG antibodies.
As shown in Table 1, the anti‑HEV IgG‑positive patients were older at the AIH diagnosis and at enrolment to the study (both P <0.001), and had higher body mass index than the patients with AIH and anti‑HEV IgG‑negative status (P = 0.047). Among clinical variables, the patients who were seropositive for anti‑HEV IgG had higher serum concentrations of total IgA (P = 0.047) and showed a trend for higher serum concentrations of γ-globulins (P = 0.058). In terms of markers of liver scarring, the patients positive for the anti‑HEV IgG antibodies had increased liver fibrosis markers, such as LSM (P = 0.03; Figure 2A), spleen stiffness (P = 0.04; Figure 2B), and FIB‑4 results (P = 0.02; Figure 2C). On the other hand, these antibodies were not associated with other disease activity markers, such as ALT, IgG, or MELD score (Table 1).
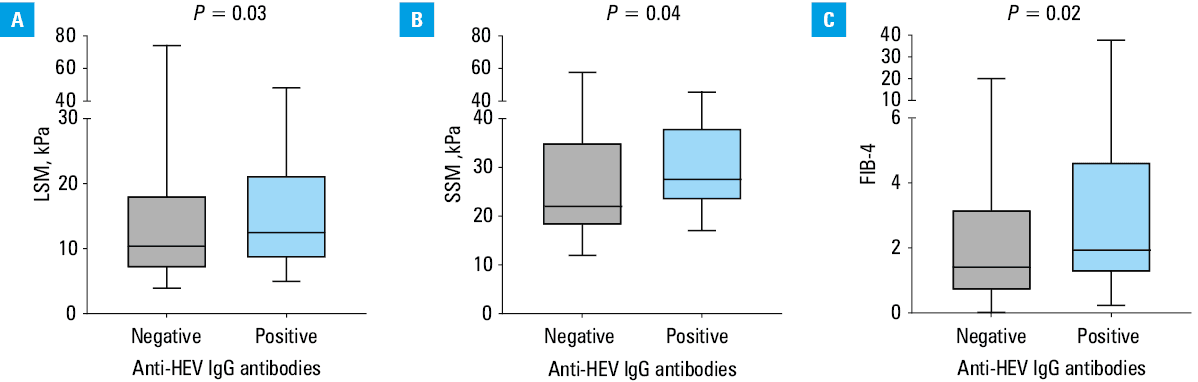
Abbreviations: FIB‑4, Fibrosis‑4 index; LSM, liver stiffness measurement; SSM, spleen stiffness measurement; others, see Figure 1
Hepatitis E virus serologic status during autoimmune hepatitis
From the entire study cohort, 269 patients were treated for AIH for at least 1 year. Overall, 39 patients (14%) were positive for anti‑HEV IgG. They had lower median (IQR) albumin concentrations (4.1 [2.7–5]) vs 4.3 [2.2–5.7] g/dl; reference range [RR], 3.5–5.5 g/dl; P = 0.009) than the anti‑HEV IgG‑negative individuals. The anti‑HEV IgG positivity was associated with higher median (IQR) LSM (12.6 [5.4–48] vs 10.2 [3.9–74] kPa; P = 0.03) in this subcohort. On the other hand, the presence of the anti‑HEV IgG antibodies was not associated with reaching a complete biochemical response after 12 months of therapy (P = 0.63). Moreover, we did not detect any significant associations between the anti‑HEV IgG status and treatment regimen, the odds of requiring liver transplantation, or liver‑related death.
Hepatitis E virus serologic status and liver fibrosis markers
To further explore the impact of anti‑HEV IgG seropositive status on liver fibrosis, we analyzed a subcohort of patients treated for AIH for at least 1 year, with normalized median (IQR) ALT activity (n = 160; ALT, 28 [8–55] U/l; RR <55 U/l; IgG, 1387 [677–1600] mg/dl; RR, 800–1600 mg/dl), to avoid inflammation bias on the fibrosis markers, in particular on LSM. Multivariable regression analysis demonstrated that seropositive anti‑HEV IgG status (odds ratio [OR], 3.69; 95% CI, 1.26–10.77; P = 0.02), ALT activity, and IgG serum concentration are independently associated with increased risk of advanced liver fibrosis (LSM ≥10.5 kPa), as presented in Table 2.
Parameter | Univariable | Multivariable | ||
P value | OR (95% CI) | P value | OR (95% CI) | |
Anti‑HEV IgG‑positive | 0.04 | 2.73 (1.07–7) | 0.02 | 3.69 (1.26–10.77) |
Immunoglobulin G, mg/dl | 0.002 | 1.01 (1–1.01) | 0.01 | 1.01 (1–1.01) |
ALT, U/l | <0.001 | 1.08 (1.04–1.11) | <0.001 | 1.07 (1.03–1.11) |
Age at blood sampling, y | 0.055 | 1.02 (1–1.05) | 0.67 | 1.01 (0.98–1.03) |
Disease duration, y | 0.13 | 1.04 (0.99–1.09) | – | – |
Age at diagnosis, y | 0.31 | 1.01 (0.99–1.03) | – | – |
Female sex | 0.39 | 1.4 (0.65–2.99) | – | – |
First‑line therapy or nil | 0.72 | 1.36 (0.26–6.96) | – | – |
Moreover, in a univariable regression analysis, the seropositivity of anti‑HEV IgG was linked to a higher risk of liver cirrhosis, defined as increased LSM (≥16 kPa), with OR of 2.78 (95% CI, 1.03–7.45; P = 0.04), as well as a higher risk of advanced liver fibrosis, defined as FIB‑4 above 2.67, with OR of 2.82 (95% CI, 1.09–7.28; P = 0.03); however, these 2 associations were not more significant in the multivariable model.
Discussion
In this study, we evaluated the potential role of a previous HEV infection on the clinical course of AIH in 374 patients, and assessed the anti‑HEV IgG seroprevalence among these patients. One of our major findings is that the patients with AIH and anti‑HEV IgG‑positive status had more pronounced liver fibrosis markers, that is, liver and spleen stiffness and FIB‑4 values, and were at a higher risk of advanced liver fibrosis. To the best of our knowledge, this observation was not previously reported in patients with AIH. In 2019, Eder et al13 evaluated the effects of previous HEV infections in 92 patients with AIH and noted a trend toward higher prevalence of cirrhosis (42% vs 21%; P = 0.053) in anti‑HEV IgG‑positive patients with AIH at the time of the first diagnosis. Authors of other reports15,22 stated no differences in AIH staging related to anti‑HEV IgG positivity. However, these studies primarily based their findings on histologic assessment of fibrosis at the time of diagnosis (cirrhosis or the Ishak score).13,15,22,23 One study reported using elastography but did not provide results specific to anti‑HEV IgG status.23 Additionally, none of these works assessed liver fibrosis at the time of sampling or reported LSMs.
Our observation regarding increased LSM in anti‑HEV IgG seropositive patients with AIH aligns with the results presented by Paternostro et al16 in 177 patients with NAFLD. The authors found that besides diabetes mellitus and older age, anti‑HEV IgG positivity was independently linked with increased liver stiffness (>10 kPa) and liver cirrhosis. Being aware of LSM limitations in AIH, we evaluated this aspect in a well‑characterized group of patients treated for at least 1 year,24 with normalized ALT activity, to limit the bias of hepatic inflammation on LSM.19,24 In our cohort, anti‑HEV IgG seropositive status was associated with increased liver fibrosis risk but not with development of cirrhosis, which might be caused, however, by low statistical power due to a small cohort of patients with liver cirrhosis.
The seroprevalence of anti‑HEV IgG in patients with AIH has been assessed in several studies. In 2014, Pischke et al12 analyzed anti‑HEV antibodies in 208 patients with AIH, finding a 7.7% positivity rate, which was higher than in healthy controls. A Dutch study14 investigated anti‑HEV IgG status in 354 patients with AIH, with 30% testing positive. This study also reported a higher frequency of anti‑smooth muscle antibody (ASMA) in patients who were anti‑HEV IgG positive.14 However, the same authors noted no evidence of a different clinical course of AIH in these patients.13 An analysis of German patients with AIH showed anti‑HEV IgG positivity in 40% of 109 individuals at diagnosis, highlighting higher prevalence in older patients.14 A 2019 study of 92 Austrian AIH patients15 found a 21% anti‑HEV IgG positivity rate, exceeding that in the general population (12%–14%), and another study confirmed the relationship with patient age.12 Contrastingly, we found lower seroprevalence of anti‑HEV IgG in the patients with AIH (15%) than in healthy blood donors (43%),11 liver transplant recipients (41%),25 and patients with advanced chronic liver diseases (48%)25 in Poland. These findings are in contrast with reports from Germany and Austria,12,13,15 where anti‑HEV IgG seroprevalence was found to be higher in patients with AIH than in the general population. However, reports from the Netherlands14 and Spain23 showed anti‑HEV IgG seroprevalence rates similar to those in the general population; therefore, the published results appear inconsistent.
The varied prevalence of anti‑HEV IgG in European cohorts of patients with AIH seems to depend on the geographic location and assay selection. The differences between patients with AIH and the healthy population in Poland might be explained by the assay used in the studies, the age of the study cohorts, and the patients’ awareness of the infection factors. First, we used the Euroimmune assay with previously reported27 61.5% sensitivity and 98.8% specificity. The other studies11,12,23,25 used the Wantai assay, which has the highest sensitivity across all available assays,10,26 and a bit lower specificity (96.5%) than Euroimmune.27 Nevertheless, available enzyme immunoassays for anti‑HEV IgG are yet to be standardized, leading to uncertainty in comparing published studies.9 Second, our cohort seems to be younger (mean [SD] age, 38 [16] years) than the reported Polish transplant recipients (mean age, 52 [13] years),25 or Polish patients with liver cirrhosis (mean age, 58 [11] years).25 Lastly, we speculate that patients with autoimmune liver diseases might be more aware of potential viral infections and prevent them by avoiding consumption of raw or undercooked meat (preventing HEV‑3 and HEV‑4 infection), as compared with the general population; however, no data support our assumption.
Finally, regarding autoimmune diseases, we should consider possible cross‑reactivity with antibodies commonly occurring in AIH, such as polyclonal γ-globulins, antinuclear antibodies (ANAs) and ASMAs. This aspect was evaluated from the HEV perspective by Terziroli et al,28 who found that 50% of 48 patients with acute HEV infection had at least 1 autoantibody (33% ANA, 21% ASMA, and 15% anti‑neutrophil cytoplasmic antibody). Previously, it was also reported that patients with AIH and anti‑HEV IgG positivity had higher serum IgG levels, γ-globulins, and higher ANA and ASMA titers, which might suggest cross‑reactivity between HEV and liver antigens.14,23 In our cohort, we found only elevated serum IgA levels and a trend toward higher γ-globulin concentrations in patients with AIH and positive for anti‑HEV IgG.
Our study has some limitations that need to be addressed. First, by using other assays as compared with previous studies, we were unable to directly compare seroprevalence with the data regarding Polish blood donors and other Polish patients with chronic liver diseases. Moreover, the HEV RNA polymerase chain reaction test was not performed in anti‑HEV IgG‑positive and anti‑HEV IgM‑negative patients; such testing should be considered in patients treated with immunosuppressants, particularly in highly suspicious cases. We have no data on antibodies at the time of blood sampling, and we cannot correlate their titers with anti‑HEV IgG antibodies. Finally, the cross‑sectional nature of the study cannot demonstrate a cause‑and‑effect relationship, which might require a prospective, multicenter study.
Conclusions
Anti‑HEV IgG seropositivity seems to correlate with more advanced liver fibrosis in patients with AIH, highlighting the influence of HEV infection on the disease progression in this population. The relatively low frequency of anti‑HEV IgG seropositivity in our study cohort might be attributed to different assays or hygienic awareness in the patients. The exact role of the HEV infection as a potential trigger of AIH needs to be elucidated in additional studies.
- Hahn JW, Yang HR, Moon JS, et al. Global incidence and prevalence of autoimmune hepatitis: a systematic review and meta‑analysis. eClinicalMedicine. 2023; 65: 102280. | Crossref
- Muratori L, Lohse AW, Lenzi M. Diagnosis and management of autoimmune hepatitis. BMJ. 2023; 380: e070201. | Crossref
- Dalekos GN, Samakidou A, Lyberopoulou A, et al. Recent advances in the diagnosis and management of autoimmune hepatitis. Pol Arch Intern Med. 2022; 132: 16334. | Crossref
- Hennes EM, Zeniya M, Czaja AJ, et al. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology. 2008; 48: 169‑176. | Crossref
- Ferri S, Muratori L, Lenzi M, et al. HCV and autoimmunity. Curr Pharm Des. 2008; 14: 1678‑1685. | Crossref
ARTICLE INFORMATION