Advanced case of Waldenström macroglobulinemia complicated by acquired hemophilia A in a patient with neurofibromatosis type 1



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Advanced case of Waldenström macroglobulinemia complicated by acquired hemophilia A in a patient with neurofibromatosis type 1
Abdominal computed tomography (CT) showed enlarged liver (length, 19 cm) and spleen (22.5 cm). Intermediate WM, also known as lymphoplasmocytic lymphoma, was diagnosed (International Prognostic Scoring System for Waldenstrom Macroglobulinemia [IPSSWM]1) with concomitant acquired hemophilia A (AHA). Initially, the patient was administered a 4‑day pulse therapy with intravenous dexamethasone (20 mg per day). For WM, 5 treatment cycles with bortezomib, dexamethasone, and rituximab (BDR) protocol were scheduled. For the initial 21‑day cycle, bortezomib was given subcutaneously at 1.3 mg/m2 on days 1, 4, 8, and 11. For cycles 2 through 5, bortezomib was administered subcutaneously at a weekly dose of 1.6 mg/m2 on days 1, 8, 15, and 22 across 4 consecutive 35‑day cycles. Additionally, during cycles 2 and 5, the patient received intravenously a single dose of dexamethasone at 40 mg and rituximab at 375 mg/m2 on days 1, 8, 15, and 22, totaling 8 infusions of rituximab. Forty‑eight hours after completing the first BDR cycle, the patient reported severe abdominal pain in the upper left quadrant. Physical examination revealed abdominal wall rigidity and tenderness in that area. Subsequent tests showed a decrease in hemoglobin from 9.3 mg/dl to 6.7 mg/dl. Abdominal CT indicated a significant amount of fluid in the peritoneal cavity suggesting active bleeding (an oval fluid collection approximately 15 cm × 8.2 cm × 13.5 cm adjacent to the spleen) (Figure 1A). Additionally, the CT scan showed dissection of the abdominal aortic wall extending to the right common iliac artery over a length of about 7.2 cm without signs of active bleeding (Figure 1B). After the patient was qualified for urgent laparotomy, supplementation with recombinant coagulation factor VII (recombinant activated factor VIIa, 5 mg intravenously every 2 hours) was initiated. During the surgery, bleeding from the splenic artery was identified, and splenectomy was performed. On histopathologic examination of the spleen, a solid infiltrate of clonal Ig κ (+) plasma cells and a few PAX5 (+), CD20+ B lymphoid cells was demonstrated, consistent with the previously diagnosed lymphoplasmocytic lymphoma. In the following weeks, treatment was continued according to the BDR protocol, achieving gradual normalization of blood and bone marrow morphology, factor VIII activity, aPTT, and serum IgM levels. The patient completed treatment 6 months ago. Currently, she is asymptomatic and remains under observation.
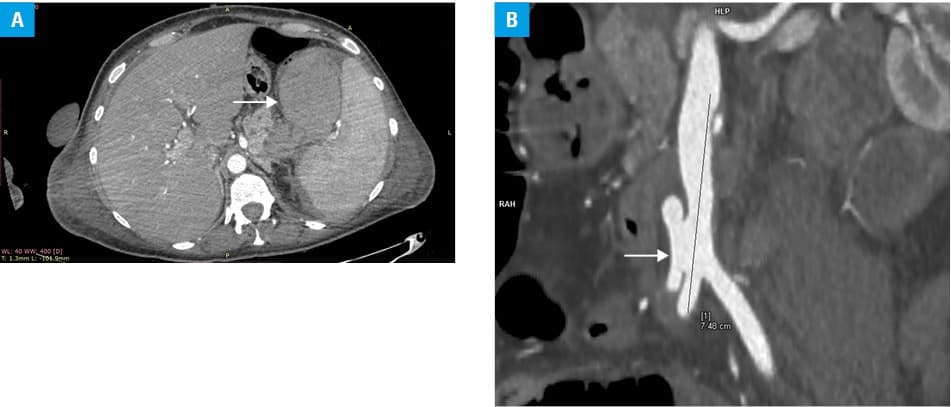
Abbreviations: HLP, main hilar artery supplying the right lower renal pole; RAH, radiologists’ handcrafted measurement
The literature has described cases of hemorrhagic complications in the course of WM associated with AHA,2 as well as spontaneous dissections and ruptures of arteries in the course of NF‑1.3,4 In the case described above, secondary AHA developed in the course of WM in a patient with NF‑1, where in the event of arterial rupture, the risk of life‑threatening hemorrhagic complications was significantly increased. NF‑1 is an autosomal dominant disorder with vascular abnormalities as a well‑recognized manifestation,5 and unlike WM and AHA cannot be effectively treated. A multicenter phase 2 trial confirmed high efficacy of the BDR protocol in the WM first‑line treatment, particularly for cases with low and intermediate IPSSWM6; however, this patient requires careful monitoring due to potential subsequent vascular complications in the course of NF‑1.
- Morel P, Duhamel A, Gobbi P, et al. International prognostic scoring system for Waldenstrom macroglobulinemia. Blood. 2009; 113:4163‑4170. | Crossref
- Brysland SA, Maqbool MG, Talaulikar D, et al. Bleeding propensity in Waldenström macroglobulinemia: potential causes and evaluation. Thromb Haemost. 2022; 122: 1843‑1857. | Crossref
- Yoshida K, Tobe S. Dissection and rupture of the left subclavian artery presenting as hemothorax in a patient with von Recklinghausen’s disease. Jpn J Thorac Cardiovasc Surg. 2005; 53: 117‑119. | Crossref
- Sakamoto S, Sumida M, Takeshita S, et al. Ruptured subclavian artery pseudo‑aneurysm associated with neurofibromatosis type 1. Acta Neurochir (Wien). 2009; 151: 1163‑1166. | Crossref
- Oderich GS, Sullivan TM, Bower TC, et al. Vascular abnormalities in patients with neurofibromatosis syndrome type I: clinical spectrum, management, and results. J Vasc Surg. 2007; 46: 475‑484. | Crossref
ARTICLE INFORMATION