Successful treatment of disseminated fungal abscess-type lesions in the brain and lungs in the course of aspergillosis in a kidney transplant recipient

 CC BY 4.0
CC BY 4.0
Successful treatment of disseminated fungal abscess-type lesions in the brain and lungs in the course of aspergillosis in a kidney transplant recipient
Aspergillosis is a rare opportunistic infection that affects transplant recipients and patients with chemotherapy‑induced neutropenia.1,2 Invasion of the central nervous system (CNS) occurs by hematogenous dissemination in immunocompromised patients.3,4 Effective management of cerebral and pulmonary aspergillosis requires rapid and accurate diagnosis.2,5 This form of aspergillosis is associated with high mortality, but clinical data have shown that liposomal amphotericin and isavuconazole provide significant efficacy in the treatment of fungal neuroinfections.1,5
A 62‑year‑old man with end‑stage renal disease due to glomerulonephritis after deceased donor kidney transplantation in 2021 was admitted to a department of nephrology with pneumonia on high‑resolution computed tomography (HRCT) and leukopenia (white blood cells, 0.54 × 103/µl; reference range [RR], 4.5–11 × 103/µl). Graft function was stable (creatinine concentration, 86 µmol/l; RR, 44–80 µmol/l). After 3 months, renal biopsy was performed and showed histopathologic features of borderline cellular rejection, which was treated with 3 doses of methylprednisolone (250 mg). After 8 months, the patient presented in severe general condition with respiratory failure requiring low‑flow oxygen, dyspnea, cough, and fever of 38.5 °C. Chest HRCT showed massive inflammatory changes (Figure 1A). Laboratory tests showed high inflammatory parameters, pancytopenia, and acute renal failure. The patient required multiple bronchoscopies. Multiple cultures (bronchoalveolar lavage [BAL], urine, blood, sputum) were positive for opportunistic pathogens. Findings included positive galactomannan in the serum and BAL, Aspergillus fumigatus in BAL, respiratory syncytial virus and parainfluenza type 4 virus, Acinetobacter baumanii in the sputum culture (negative bacteriologic tests in BAL). Direct preparation and genetic probe for tuberculosis and pneumocystosis were negative. Treatment was given according to BAL results (tigecycline, colistin, cymevene, voriconazole, all intravenously). Antibiotics, antifungals, and antivirals were changed according to microbiologic tests and glomerular filtration rate (GFR). Filgrastim was given for severe neutropenia. The patient required intravenous immunoglobulins and 2 hemodialyses for acute kidney injury. An episode of right upper limb paresis and limited responsiveness was observed and magnetic resonance (MR) neuroimaging was performed (Figure 1B–1D). Stroke could not be excluded due to newly‑diagnosed atrial fibrillation and low‑molecular‑weight heparin and acetylsalicylic acid were recommended. The patient was transferred to a nephrology department for further management.
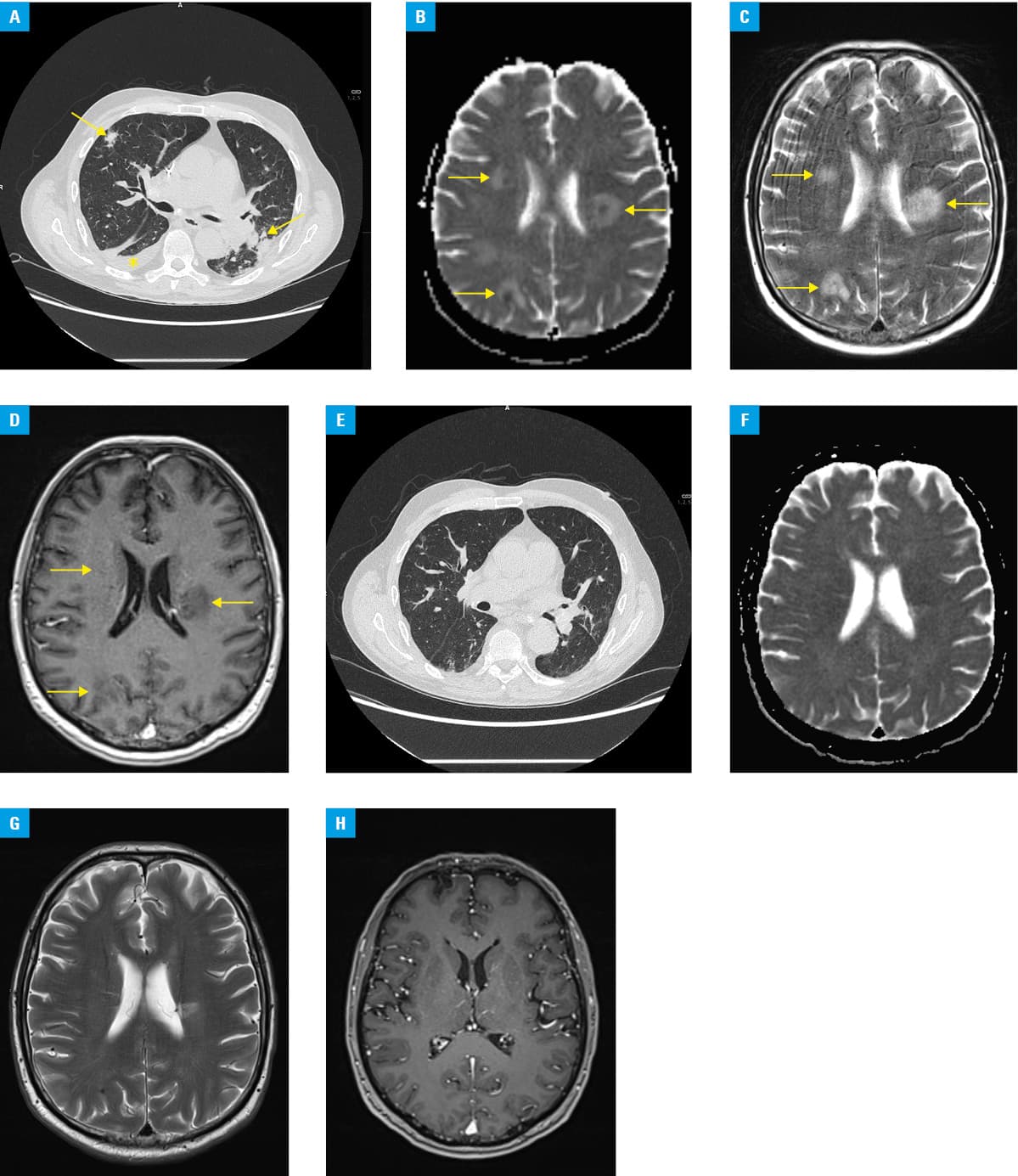
After the onset of fever and worsening of pulmonary inflammation and new lesion on brain MR, liposomal amphotericin was added at a GFR‑adjusted dose, followed by intravenous isavuconazole. The patient had symptoms of focal brain damage for several days, probably related to CNS fungal abscess‑type lesions. He suffered from persistent dysarthria and dysphonia, with central facial muscle paresis on the right side, with paresis of the right upper limb, without meningeal or pathologic symptoms. Treatment stabilized his general condition, with a decrease in inflammatory parameters, improvement in renal function, and regression of radiologic changes in the lungs (Figure 1E) and brain (Figure 1F–1H).The current follow‑up from the diagnosis of brain and lung aspergillosis to April 2024 has been 30 months. The patient is on a maintenance dose of oral voriconazole 200 mg twice daily. The mortality risk in patients with CNS involvement in the course of this infection exceeds 80%–90%, resulting in very limited data on long‑term survival.3-5
- Husain S, Camargo JF. Invasive aspergillosis in solid‑organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019; 33: e13544. | Crossref
- Pérez‑Jacoiste Asín MA, López‑Medrano F, Fernández‑Ruiz M, et al. Risk factors for the development of invasive aspergillosis after kidney transplantation: systematic review and meta‑analysis. Am J Transplant. 2021; 21: 703‑716. | Crossref
- Dybko Z, Poznański P, Mazanowska O, et al. Fatal case of invasive fungal disease due to Aspergillus infection in liver transplant recipient. Pol Arch Intern Med. 2024; 15: 16702. | Crossref
- Tyll T, Lyskova P, Hubka V, et al. Cerebral aspergillosis: Aspergillus calidoustus. Mycopathologia. 2022; 187: 133‑135. | Crossref
- Cadena J, Thompson GR, Patterson TF. Aspergillosis: epidemiology, diagnosis, and treatment. Infect Dis Clin North Am. 2021; 35: 415‑434. | Crossref
ARTICLE INFORMATION