Clinical and echocardiographic characterization of patients hospitalized for severe tricuspid valve regurgitation: a single tertiary-care center experience with 2-year follow-up
Key words: heart failure, TAPSE, TAPSE/SPAP ratio, tricuspid regurgitation, TRI-SCORE

 CC BY 4.0
CC BY 4.0
Clinical and echocardiographic characterization of patients hospitalized for severe tricuspid valve regurgitation: a single tertiary-care center experience with 2-year follow-up
Introduction: Tricuspid regurgitation (TR) is a common acquired valvular heart disease. Recently, new transcatheter treatment options for severe TR have emerged that could change management of this condition, which warrants better characterization of this specific patient group.
Objectives: The aim of the study was to describe the clinical and echocardiographic characteristics of patients with severe TR and to evaluate their short- and mid‑term prognosis.
Patients and methods: This retrospective, observational, single‑center study enrolled consecutive patients with severe TR hospitalized between January 2016 and September 2021 in the Department of Cardiology, Medical University of Warsaw, Poland. The severity of heart failure (HF) was evaluated using the New York Heart Association classification. Echocardiographic assessment was performed by an experienced sonographer. EuroSCORE II and TRI‑SCORE models were computed for each patient, and 12- and 24‑month clinical outcomes were reported.
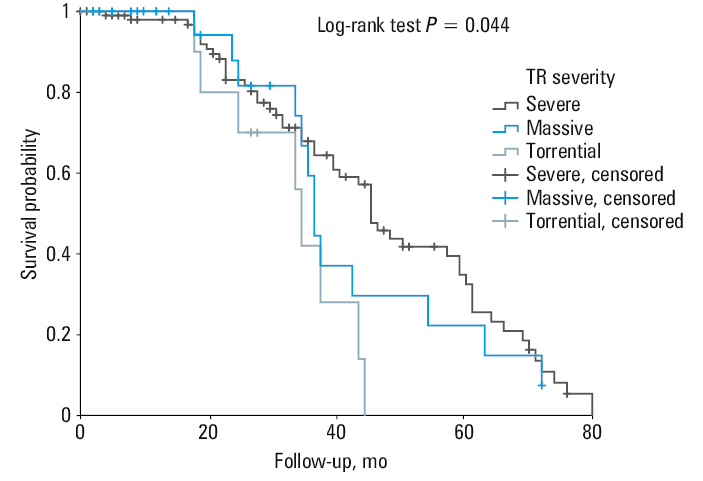
Results: The study comprised 172 patients (93 women [54.1%]) at a mean (SD) age of 76.4 (10.5) years. The most common comorbidities included: atrial fibrillation (84.9%), hypertension (68%), chronic kidney disease (54.1%), coronary artery disease (45.3%), and diabetes mellitus (30.9%). The median (interquartile range) EuroSCORE II and TRI‑SCORE values were 4.68% (2.88%–8.05%) and 14% (5%–34%), respectively. The median follow‑up was 24 (8.5–41) months. The overall mortality was 29.7% at 1 year and 47.3% at 2 years. TR grade, tricuspid annular plane systolic excursion (TAPSE) above 17 mm, TAPSE to systolic pulmonary artery pressure ratio below 0.26, and increased right atrial area were significant factors associated with mortality.
Conclusions: Patients presenting with severe TR are characterized by a large comorbidity burden and poor prognosis, despite intensive HF management.
What's new?
Tricuspid regurgitation (TR) only recently has been fully acknowledged as a serious condition and a target of specific treatment. Following introduction of new transcatheter treatment methods, more patients with severe TR could become eligible for treatment optimization. In order to do so, it is necessary to better characterize this demanding patient subset. Our study provides a thorough characterization of a real‑life cohort of patients with severe TR, including clinical and echocardiographic factors. Overall mortality in this group is disproportionately high, and tricuspid annular plane systolic excursion to systolic pulmonary artery pressure ratio and increased right atrial area are echocardiographic parameters associated with worse prognosis. Moreover, based on our study, we suggest the use of the TRI‑SCORE model instead of EuroSCORE II model in patients with severe TR, as the latter can underestimate the risk.
Introduction
Tricuspid regurgitation (TR) is a common acquired valvular heart disease (VHD). It is characterized by backflow of blood through a dysfunctional tricuspid valve (TV), which leads to right ventricular failure symptoms, such as peripheral edema and ascites. In the majority of cases, TR is a functional disease caused by right ventricular (RV) dilatation, usually secondary to left‑sided congestive heart failure (HF) or VHD. Recently, an alternative mechanism of TR due to the tricuspid annulus (TA) enlargement in the setting of long‑standing atrial fibrillation has been suggested. In some patients, TR can also be caused or exacerbated by the presence of a cardiac implantable electronic device (CIED).1,2
Echocardiography is a basic imaging modality to assess the mechanism and severity of TR.3-6 Severe TR affects morbidity and has been previously reported as a strong negative predictor of long‑term survival in the general population. Recent advances in both pharmacotherapy and transcatheter treatment techniques led to a reduction of mortality in a variety of cardiac conditions, such as HF or VHD; however, their influence on the prognosis in an unselected population of TR patients in a real‑life setting has not been fully evaluated. The aim of this study was to describe the clinical and echocardiographic characteristics and to evaluate the short- and mid‑term prognosis of the contemporary cohort of patients with severe TR diagnosed and treated in a tertiary VHD center.
Patients and methods
This retrospective, observational, single‑center study enrolled consecutive patients with severe TR hospitalized between January 2016 and September 2021 in the Department of Cardiology, Medical University of Warsaw, Poland. The severity of HF was evaluated using the New York Heart Association (NYHA) classification. EuroSCORE II and TRI‑SCORE models were calculated for each patient.7,8 Echocardiographic examination was performed by certified sonographers (PS and AKC), and 12- and 24‑month clinical outcomes were reported.
Study population
From the available records, we retrospectively identified consecutive patients admitted to the Department of Cardiology between January 2016 and September 2021 in whom the presence of severe TR was confirmed during the index hospitalization. The patients whose baseline clinical and echocardiographic data were not available were excluded.
Data collection
The data were collected from the electronic database and included: patient age, sex, comorbidities and previously performed cardiac procedures, the NYHA HF class, laboratory parameters, pharmacologic treatment, and procedures performed during the index hospitalization.
Routine transthoracic echocardiography (TTE) was performed and analyzed by a certified cardiologist during the index hospitalization, and the echocardiographic data were collected from the electronic database. The date of death was obtained from the patients’ family members and from the Polish national public registries. The primary end point was all‑cause mortality, and the period analyzed was from the day when the echocardiographic evidence of severe TR was obtained until death or the last follow‑up in May 2022.
Echocardiography
To obtain the analyzed parameters, 2‑dimensional TTE enriched with M‑mode and color Doppler was performed according to the guidelines4,5. Tricuspid annular plane systolic excursion (TAPSE) was measured in M‑mode at the junction of the TV and RV free wall. The severity of TR and the function of other valves were assessed using qualitative, semiquantitative, and quantitative approaches provided in the guidelines.5,9 Severe TR was defined based on echocardiographic parameters of TR as effective regurgitant orifice area (EROA) of 40–59 mm2, TR regurgitant volume (TRvol) 45–59 ml, or vena contracta width (VCW) 7–13.9 mm. Massive TR was defined as EROA 60–79 mm2, or TRvol 60–74 ml, or VCW 14–20.9 mm. Torrential TR was defined as EROA equal to or above 80 mm2, TRvol equal to or above 75 ml, or VCW equal to or above 21 mm.10 Quantification of the chambers was performed in apical 2- and 4‑chamber views or RV‑focused apical 4‑chamber view for the left and right chambers, respectively. The left ventricular ejection fraction was assessed with the Simpson method.11 Wall motion was measured using the 16‑segment model.11 The probability of pulmonary hypertension (PH) was evaluated using systolic pulmonary artery pressure (SPAP), tricuspid regurgitation pressure gradient (TRPG), and echocardiographic signs suggesting PH regarding the ventricles, pulmonary artery, inferior vena cava (IVC), and right atrium (RA).12-14 Additionally, the TAPSE/SPAP ratio was calculated for all patients.
We analyzed the prognostic significance of echocardiographic parameters associated with the RV function and remodeling,15,16 that is, RV dysfunction defined as TAPSE below 17 mm, diameter and collapse of the IVC, where a value above 21 mm was considered IVC dilatation, flattening of the interventricular septum, presence of the echocardiographic features of PH and the TA dilatation, defined as TA diameter above 40 mm.
Statistical analysis
Statistical analysis was carried out with IBM SPSS Statistics package (version 28.0; IBM, New York, New York, United States). The Shapiro–Wilk test was performed to assess distribution of the continuous variables. The normally distributed variables are presented as mean (SD) and compared with the t test. The non‑normally distributed variables are presented as median with interquartile range (IQR) and compared with the Mann–Whitney test. Categorical variables are presented as a number and percentage and compared using the χ2 test or the Fisher exact test. The survival analysis was performed using the Kaplan–Meier survival analysis, receiver operating characteristic (ROC) curve analysis, and nonadjusted and adjusted Cox regressions for evaluation of the factors associated with mortality. Adjusted Cox regression models included age, sex, diabetes mellitus (DM), chronic kidney disease (CKD), anemia, and echocardiographic parameters which were significant at univariable Cox regression. Statistical significance was established at 2‑sided P value below 0.05.
Results
Patient characteristics
Overall, we analyzed 172 patients (93 women [54.1%]) with severe or greater TR. Of those, 126 individuals (73.2%) had severe TR, 33 (19.2%) had massive TR, and 13 (7.6%) had torrential TR. Median (IQR) EROA was 58 mm2 (49–74 mm2), median TRvol was 57 ml (48–70.3 ml), and median VCW was 10 mm (8–12 mm). Baseline echocardiographic characteristics of TR are provided in Table 1. The mean (SD) age of the patients was 76.4 (10.5) years. The most common comorbidity was atrial fibrillation (n = 146; 84.9%). The remaining comorbidities included hypertension (n = 117; 68%), CKD (n = 93; 54.1%), coronary artery disease (CAD; n = 78; 45.3%), DM (n = 53; 30.9%), and respiratory diseases such as chronic obstructive pulmonary disease (COPD; n = 23; 13.4%) or asthma (n = 7; 4.1%). Some patients had a history of myocardial infarction (n = 42; 24.4%) and prior stroke or transient ischemic attack (n = 24; 14%). Peripheral edema or ascites were found in 79 (45.9%) and 33 (19.2%) patients, respectively. The median (IQR) EuroSCORE II and TRI‑SCORE values were 4.68% (2.88%–8.05%) and 14% (5%–34%), respectively.
Parameter | Value |
Data are provided as number and percentage or median and interquartile range.
Abbreviations: EROA, effective regurgitant orifice area; TR, tricuspid regurgitation; TRvol, regurgitant volume of tricuspid regurgitation; VCW, vena contracta width | |
Severe TR | 126 (73.2) |
Massive TR | 33 (19.2) |
Torrential TR | 13 (7.6) |
EROA, mm2 | 58 (49–74) |
TRvol, ml | 57 (48–70.3) |
VCW, mm | 10 (8–12) |
The past procedures included 23 systemic valve interventions (13.4%), of which transcatheter aortic valve implantation was performed in 3 patients (1.7%) and mitral transcatheter edge‑to‑edge repair (TEER) in 2 patients (1.2%). Nine patients (5.2%) underwent coronary artery bypass grafting, 32 (18.6%) had percutaneous coronary intervention (PCI), and 4 (2.3%) tricuspid valvuloplasty (isolated). Almost a half (n = 81; 47.1%) of the patients were provided with an implantable device, of which 78 (45.3%) had a ventricular lead placed.
Interventions
During the index hospitalization, the following procedures were performed: cardiac surgery (aortic valve replacement, mitral valve replacement, or mitral valve repair) in 3 patients, percutaneous treatment in 7 patients, including PCI in 6 patients (3.5%) and 1 mitral TEER, implantation of a CIED in 26 patients (15.1%), battery replacement in 11 patients (6.4%), the CIED lead removal in 5 patients (2.9%), and catheter ablation in 2 patients (1.2%). Coronary angiography was performed in 43 patients (25%), documenting CAD in 21 individuals (12.2%). That included 11 patients (6.4%) with multivessel disease. The data concerning pharmacologic treatment, laboratory results, and echocardiographic parameters are presented in Table 2.
Parameter | Overall (n = 172) | TAPSE ≥17 mm (n = 84) | TAPSE <17 mm (n = 88) | P value |
Data are provided as number and percentage or median and interquartile range unless stated otherwise.
SI conversion factors: to convert ALT and AST to μkat/l, multiply by 0.0167; creatinine to μmol/l, by 88.4; hemoglobin to g/l, by 10; NT‑proBNP to ng/l, by 1.
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ACT, acceleration time; AF, atrial fibrillation; ALT, alanine transaminase; ARNI, angiotensin receptor‑neprilysin inhibitor; Ao, aorta; Ao Vmax, peak aortic valve velocity; ASA, acetylsalicylic acid; AST, aspartate transaminase; CAD, coronary artery disease; CCB, calcium channel blocker; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; EF, ejection fraction; eGFR, estimated glomerular filtration rate; ERO, effective regurgitant orifice; HCTZ, hydrochlorothiazide; HF, heart failure; HT, hypertension; INR, international normalized ratio; IVC, inferior vena cava; IVS, interventricular septum; IVSd, interventricular septum thickness in diastole; LA, left atrium; LAA, left atrial area; LV, left ventricle; LVDd, left ventricular dimension in diastole; LVH, left ventricular hypertrophy; MI, myocardial infarction; MRA, mineralocorticoid receptor antagonist; NOAC, non–vitamin K antagonist oral anticoagulant; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide; NYHA, New York Heart Association; MR, mitral regurgitation; MRvol, mitral regurgitation volume; PA, pulmonary artery; PLT, platelets; PWTd, posterior wall thickness in diastole; RA, right atrium; RAA, right atrial area; RV, right ventricle; RVIT AP4C, right ventricular inflow tract in apical 4‑chamber view; SGLT2, sodium‑glucose transporter type 2; SPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TIA, transient ischemic attack; TRPG, tricuspid regurgitation pressure gradient; VKA, vitamin K antagonist | ||||
Age, y | 77 (70.3–83.8) | 77 (71–84) | 76 (70–82) | 0.55 |
Women | 93 (54.1) | 49 (58.3) | 44 (50) | 0.27 |
EuroSCORE II, % | 4.68 (2.88–8.05) | 3.32 (1.9–5.42) | 6.38 (4.04–1.08) | <0.001 |
TRI‑SCORE, % | 14 (5–34) | 5 (3–14) | 22 (5–48) | <0.001 |
Comorbidities | ||||
AF | 146 (84.9) | 67 (79.8) | 79 (89.8) | 0.07 |
HT | 117 (68) | 57 (67.9) | 60 (68.2) | 0.96 |
CAD | 78 (45.3) | 36 (42.9) | 42 (47.7) | 0.52 |
CKD | 93 (54.1) | 42 (50) | 51 (58) | 0.3 |
Hemodialysis | 7 (4.1) | 3 (3.6) | 4 (4.5) | 0.75 |
DM | 53 (30.9) | 26 (31) | 27 (30.7) | 0.97 |
Insulin | 15 (8.7) | 8 (9.5) | 7 (7.7) | 0.72 |
COPD | 23 (13.4) | 7 (8.3) | 16 (18.2) | 0.06 |
Asthma | 7 (4.1) | 1 (1.2) | 6 (6.8) | 0.06 |
Previous MI | 42 (24.4) | 18 (21.4) | 24 (27.3) | 0.37 |
Previous stroke / TIA | 24 (14) | 12 (14.5) | 12 (12.4) | 0.88 |
Symptoms of HF | ||||
Peripheral edema | 79 (45.9) | 33 (39.3) | 46 (52.3) | 0.09 |
Ascites | 33 (19.2) | 10 (11.9) | 23 (26.1) | 0.02 |
NYHA class | ||||
I | 34 (19.8) | 20 (23.8) | 14 (15.9) | 0.19 |
II | 43 (25) | 27 (32.1) | 16 (18.2) | 0.04 |
III | 57 (33.1) | 23 (27.4) | 34 (38.6) | 0.12 |
IV | 38 (22.1) | 14 (16.7) | 24 (27.3) | 0.09 |
Treatment | ||||
Any loop diuretic | 150 (87.2) | 68 (81) | 82 (93.2) | 0.02 |
Torasemide | 53 (30.8) | 30 (35.7) | 23 (26.1) | 0.174 |
Furosemide | 108 (62.8) | 44 (52.4) | 64 (72.7) | 0.006 |
HCTZ | 21 (12.7) | 5 (6) | 16 (10.5) | 0.01 |
Indapamide | 7 (4.2) | 6 (7.2) | 1 (1.2) | 0.053 |
MRA | 74 (44.6) | 34 (41) | 40 (48.2) | 0.35 |
Any diuretic | 172 (100) | 84 (100) | 88 (100) | 1.00 |
β-Blocker | 145 (84.3) | 68 (80.9) | 77 (87.5) | 0.06 |
ACEI | 98 (57) | 50 (59.5) | 48 (54.5) | 0.68 |
Sartan | 14 (8.4) | 8 (9.5) | 6 (6.8) | 0.58 |
CCB | 27 (15.7) | 16 (19) | 11 (12.5) | 0.29 |
ASA | 26 (15.1) | 12 (14.3) | 14 (15.9) | 0.69 |
ARNI | 2 (1.2) | 2 (2.4) | 0 | 0.16 |
P2Y12 inhibitor | 12 (7) | 5 (6) | 7 (8) | 0.56 |
VKA | 47 (27.3) | 21 (25) | 26 (29.5) | 0.39 |
NOAC | 66 (38.4) | 36 (42.9) | 30 (34.1) | 0.34 |
Heparin | 30 (17.4) | 13 (15.5) | 17 (19.3) | 0.46 |
Statin | 109 (63.4) | 56 (66.7) | 53 (60.2) | 0.62 |
SGLT2 inhibitor | 4 (2.3) | 2 (2.4) | 2 (2.3) | >0.99 |
Blood parameters | ||||
Hemoglobin, g/dl, mean (SD) | 12.04 (2.18) | 11.84 (2.35) | 12.22 (2) | 0.25 |
PLT, 103/μl | 177 (140–230) | 180 (135–229) | 168.5 (141–237) | 0.7 |
Urea, mg/dl | 55 (41.3–83.3) | 47 (37–69) | 69 (50–101) | <0.001 |
Creatinine, mg/dl | 1.28 (1.04–1.77) | 1.21 (0.94–1.59) | 1.39 (1.12–2.04) | 0.01 |
eGFR, ml/min/1.73 m2 | 43 (29.2–58) | 47 (31.6–61) | 41.2 (28.9–51.3) | 0.07 |
NT‑proBNP, pg/ml | 3123 (1261–8593) | 1751 (951–4076) | 4604 (2 118–11 657) | <0.001 |
INR | 1.42 (1.2–2.61) | 1.36 (1.19–2.05) | 1.45 (1.22–3.22) | 0.11 |
AST, U/l | 31 (24–42) | 30 (24–44) | 32 (25–42) | 0.57 |
ALT, U/l | 28 (21–36) | 28 (21–37) | 27 (20–36) | 0.32 |
Echocardiographic parameters | ||||
Significant MR | 70 (40.7) | 31 (36.9) | 39 (44.3) | 0.32 |
ERO, cm2 | 0.21 (0.15–0.36) | 0.2 (0.15–0.26) | 0.26 (0.16–0.39) | 0.11 |
MRvol, ml, mean (SD) | 38.6 (22.1) | 35.8 (22.1) | 40.5 (22.1) | 0.31 |
Ao Vmax, m/s | 1.4 (1.13–1.8) | 1.36 (1.1–1.7) | 1.4 (1.1–2.17) | 0.4 |
Tricuspid annular diameter, mm, mean (SD) | 46.8 (6.7) | 46.6 (7.7) | 47.1 (5.7) | 0.71 |
TRPG, mm Hg, mean (SD) | 39.9 (18.8) | 40.1 (18.3) | 39.8 (19.5) | 0.93 |
Presence of right ventricular lead | 77 (44.8) | 36 (42.9) | 41 (46.6) | 0.62 |
PA dilatation | 78 (45.3) | 33 (39.3) | 45 (51.1) | 0.14 |
ACT, ms, mean (SD) | 93.1 (23.3) | 92 (21) | 94.1 (25.4) | 0.57 |
Pericardial effusion | 42 (24.4) | 23 (27.4) | 19 (21.6) | 0.38 |
LVDd, cm, mean (SD) | 5.2 (1.1) | 5 (0.9) | 5.5 (1.2) | 0.002 |
IVSd, cm, mean (SD) | 1.1 (0.2) | 1.1 (0.2) | 1.2 (0.2) | 0.63 |
PWDTd, cm, mean (SD) | 1 (0.2) | 1 (0.1) | 1 (0.2) | 0.84 |
RV, cm, mean (SD) | 3.6 (0.7) | 3.5 (0.6) | 3.6 (0.7) | 0.14 |
Ao, cm, mean (SD) | 3.4 (0.4) | 3.4 (0.4) | 3.4 (0.5) | 0.58 |
LA, cm | 5.3 (4.8–6) | 5.1 (4.7–5.4) | 5.2 (4.6–5.8) | 0.15 |
EF, %, mean (SD) | 46.9 (14.5) | 47.6 (13.9) | 46.2 (15) | 0.54 |
LA enlargement | 162 (94.2) | 79 (94) | 83 (94.3) | 0.94 |
RA enlargement | 159 (92.4) | 76 (90.5) | 83 (94.3) | 0.34 |
LV enlargement | 52 (30.2) | 18 (21.4) | 34 (38.6) | 0.01 |
RV enlargement | 126 (73.3) | 59 (70.2) | 67 (76.1) | 0.38 |
LAA, cm2, mean (SD) | 37.4 (13.8) | 35.7 (9.1) | 39.1 (17.2) | 0.15 |
RAA, cm2, mean (SD) | 36.4 (11.3) | 36.2 (9.5) | 36.6 (12.9) | 0.87 |
RVIT AP4C, cm, mean (SD) | 5.2 (1.1) | 5.1 (1.0) | 5.3 (1.2) | 0.3 |
Asynchrony LV+IVS | 23 (13.4) | 13 (15.5) | 10 (11.4) | 0.38 |
Segmental contractility dysfunction | 88 (51.2) | 36 (42.9) | 52 (59.1) | 0.03 |
LVH | 58 (33.7) | 27 (32.1) | 31 (35.2) | 0.67 |
Hepatic vein flow reversal | 77 (44.8) | 37 (44.1) | 40 (45.5) | 0.85 |
IVC dilatation | 52 (30.2) | 28 (33.3) | 24 (27.3) | 0.41 |
IVC width, cm | 2.7 (2.4–3) | 2.6 (2.2–2.95) | 2.6 (2.2–3) | 0.59 |
Absent respiratory collapse of IVC | 117 (68) | 54 (64.3) | 63 (71.6) | 0.58 |
Flattening of the IVS | 34 (19.8) | 22 (26.2) | 12 (13.6) | 0.04 |
SPAP, mm Hg, mean (SD) | 60.4 (17.2) | 59.6 (18.1) | 62.6 (16) | 0.29 |
Follow‑up
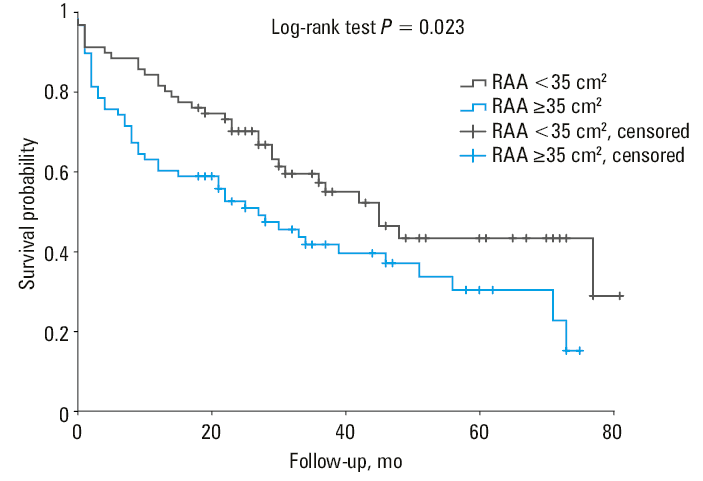
Median (IQR) follow‑up was 24 (8.5–41) months. Clinical status at 1 year was available for 90.1% of patients, and at 2 years for 86% of patients. The overall mortality was 29.7% at 1 year and 47.3% at 2 years. Higher grade of TR, TAPSE below 17 mm, TAPSE/SPAP ratio below 0.26, and right atrial area (RAA) equal to or above 35 cm2 were associated with worse survival in the Kaplan–Meier survival analysis with log‑rank test values of P = 0.04, P = 0.002, P = 0.02, and P = 0.02, respectively (Figures 1, 2, 3, 4). The characteristics of the patients according to the TAPSE value are presented in Table 2. The ROC curve analysis regarding 2‑year mortality showed the area under the curve (AUC) values for the cutoff of the RAA at 35.95 cm2 (AUC = 0.612; P = 0.03); SPAP of 52.5 mm Hg (AUC = 0.627; P = 0.046), and IVC diameter of 2.45 cm (AUC = 0.621; P = 0.03).
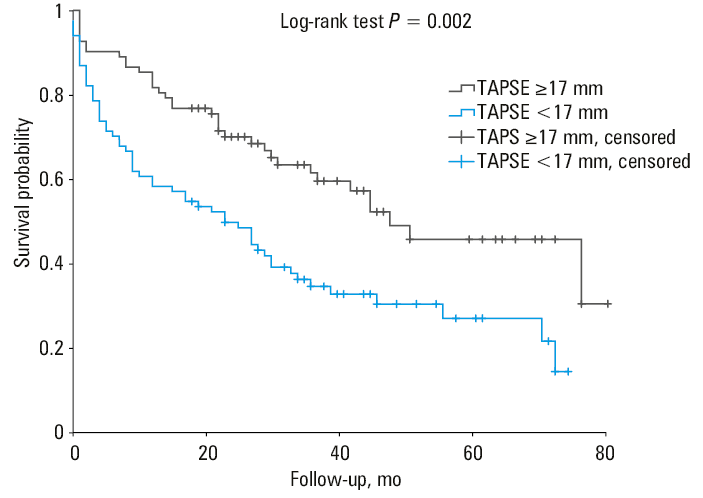
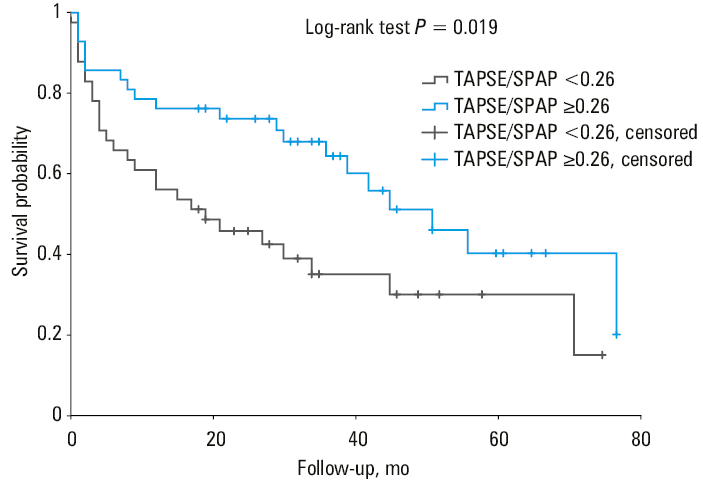
The nonadjusted Cox regression results are presented in Table 3. Meaningful results were found for TAPSE below 17 mm (hazard ratio [HR], 1.905; 95% CI, 1.25–2.902; P = 0.003), median TAPSE/SPAP equal to or above 0.26 (HR, 0.502; 95% CI, 0.277–0.908; P = 0.02), TRPG above 36 mm Hg (HR, 1.52; 95% CI, 1.006–2.297; P = 0.047), anemia (HR, 1.869; 95% CI, 1.214–2.877; P = 0.005), and DM (HR, 1.915; 95% CI, 1.274–2.88; P = 0.002). The results for CAD and COPD were insignificant.
Variable | HR (95% CI) | P value |
Abbreviations: AR, aortic regurgitation; others, see Table 2 | ||
TAPSE/SPAP ≥0.26 | 0.502 (0.277–0.908) | 0.02 |
TAPSE <17 mm | 1.905 (1.25–2.902) | 0.003 |
EF <50% | 1.193 (0.801–1.793) | 0.38 |
TRPG >36 mm Hg | 1.52 (1.006–2.297) | 0.047 |
AR presence | 1.536 (0.957–2.465) | 0.08 |
Severe MR | 1.073 (0.718–1.604) | 0.73 |
Anemia | 1.869 (1.214–2.877) | 0.005 |
CKD | 1.504 (0.995–2.275) | 0.053 |
CAD | 1.391 (0.93–2.08) | 0.11 |
COPD | 1.621 (0.969–2.713) | 0.07 |
RAA ≥35 cm2 | 1.67 (1.065–2.619) | 0.03 |
Age ≥75 y | 1.305 (0.86–1.982) | 0.21 |
DM | 1.915 (1.274–2.88) | 0.002 |
IVC diameter, mm | 1.63 (0.968–2.742) | 0.07 |
SPAP >52 mm Hg | 1.532 (0.835–2.811) | 0.17 |
The adjusted Cox regression models were developed for age, sex, diabetes, CKD, anemia, and all echocardiographic parameters (Models 1–5), and Model 6 included age, sex, diabetes, CKD, anemia, and all significant echocardiographic parameters from models 1–5. In model 5, statistically signficant results were obtained for DM (HR, 2.048; 95% CI, 1.261–3.324; P = 0.004), anemia (HR, 2.161; 95% CI, 1.22–3.827; P = 0.008), RAA equal to or above 35 cm2 (HR, 1.774; 95% CI, 1.101–2.856; P = 0.02), and TAPSE below 17 mm (HR, 2.054; 95% CI, 1.273–3.317; P = 0.003). All significant results are shown in Table 4.
Variable | HR (95% CI) | P value |
Model 1 (age, sex, CKD, anemia, DM, TAPSE) | ||
DM | 1.902 (1.24–2.918) | 0.03 |
Anemia | 1.922 (1.153–3.202) | 0.01 |
TAPSE <17 mm | 2.071 (1.344–3.192) | <0.001 |
Model 2 (age, sex, CKD, anemia, DM, TAPSE/SPAP) | ||
DM | 2.621 (1.378–4.987) | 0.003 |
Model 3 (age, sex, CKD, anemia, DM, RAA) | ||
DM | 1.935 (1.199–3.124) | 0.007 |
Anemia | 1.917 (1.098–3.346) | 0.02 |
RAA ≥35 cm2 | 1.893 (1.193–3.004) | 0.007 |
Model 4 (age, sex, CKD, anemia, DM, TRPG) | ||
DM | 1.76 (1.138–2.722) | 0.01 |
Anemia | 1.815 (1.087–3.03) | 0.02 |
Model 5 (age, sex, CKD, anemia, DM, TAPSE, RAA) | ||
DM | 2.048 (1.261–3.324) | 0.004 |
Anemia | 2.161 (1.22–3.827) | 0.008 |
RAA ≥35 cm2 | 1.774 (1.101–2.856) | 0.02 |
TAPSE <17 mm | 2.054 (1.273–3.317) | 0.003 |
The main echocardiographic findings included enlargement of the left (94.2%) and right (92.4%) atria and RV (73.3%). Dilatation of the pulmonary trunk was observed in nearly half of the patients, and more than a half had segmental contractility dysfunction. The remaining echocardiographic parameters are presented in Table 2.
Discussion
The present study characterizes an unselected cohort of severe TR patients diagnosed and treated in a tertiary VHD center. It provides insight into the contemporary real‑life practice in this heterogenous population. Although TR is a highly common echocardiographic finding,17,18 it used to be frequently considered as a concomitant disorder and neglected as a potential therapeutic target.
According to the current guidelines, cardiac surgery remains the first‑choice method in the invasive treatment of patients with severe symptomatic TR refractory to optimal medical therapy.8 At present, valve repair or replacement in primary symptomatic severe TR is accepted as a class I indication. Also, patients referred for the left‑sided valve surgery with concomitant TR should undergo simultaneous tricuspid valve repair, regardless of the presence of the symptoms. Furthermore, in patients with isolated severe symptomatic TR without significant pulmonary hypertension, surgery should be considered before development of advanced RV failure. However, in contemporary practice, most of the TR patients are denied surgery and treated conservatively due to unacceptably high perioperative mortality.
Optimal medical treatment administered according to current guidelines19 drastically improves outcomes in patients with HF. However, management of patients with severe TR is exceptionally difficult, as demonstrated by our study. The diuretic therapy often consists of more than 1 diuretic agent to manage fluid retention. In our study, 150 patients (87.2%) received a loop diuretic, 21 (12.7%) received hydrochlorothiazide, 7 (4.2%) received indapamide, and 74 (44.6%) a mineralocorticoid receptor antagonist. Moreover, a recent study suggests that an add‑on diuretic therapy with oral acetazolamide could be a both safe and effective option in patients with fluid retention.20 Despite intensive treatment, the mortality and re‑hospitalization burden is disproportionately high in the subgroup of patients with severe TR. One of the main findings of our study is the mortality rate of 29.7% at 12 months, reaching the level of 47.3% at 24‑month follow‑up. The excessive death rate observed in this unselected cohort indicates that the recognition of prognostic factors and their appropriate management is of paramount importance in the treatment of TR patients. Moreover, this proves that additional treatment options, beyond medical therapy, should be taken into consideration in patients with severe TR, especially those not suitable for surgery.
Improving our risk‑stratification tools could prove beneficial in treatment optimization in selected patients. EuroSCORE II is a widely used model for estimating in‑hospital mortality in patients undergoing cardiac surgery. TRI‑SCORE is a disease‑specific model similar to EuroSCORE II. The TRI‑SCORE scale estimates the in‑hospital mortality in patients undergoing cardiac surgery for isolated TR. Although these risk models have been originally developed and validated for patients undergoing surgery, we decided to perform exploratory analyses using these scores in our mostly conservatively managed cohort. These calculations indicated very high surgical risk in our cohort. Moreover, our analysis showed differences in predicted mortality risk between those risk stratification models. We found that TRI‑SCORE calculations resulted in significantly higher predicted risk than EuroSCORE II, despite the conservative treatment approach. The potential role of these models as predictors of adverse outcomes in conservatively managed patients with severe TR needs further research.
We also observed a correlation between RV dysfunction in echocardiographic assessment and mortality rate. Already developed right HF (RHF) resulted in a higher mortality rate. This proves that adequate treatment should be administered before irreversible remodeling of the RV. In our study, TAPSE value below 17 mm was independently related to the mortality observed during follow‑up. In addition, in the patients with TAPSE values below 17 mm, significantly higher incidence of ascites as well as elevated N‑terminal pro–B‑type natriuretic peptide levels were observed.
Ongoing is a search for other echocardiographic parameters that could have a predictive value. A novel simple parameter for identification of RHF‑prone patients that has been proposed is TAPSE/SPAP ratio.21-24 This ratio combines the assessment of RV function with the RV afterload, and has a prognostic role in other clinical settings. In our cohort, the patients with median TAPSE/SPAP below 0.26 had a significantly higher mortality rate than those with the ratio equal to or above 0.26, warranting prospective validation among the patients with severe TR. Moreover, we found that SPAP equal to or above 52.5 mm Hg, RAA equal to or above 35.95 cm2, and the IVC diameter equal to or above 2.45 cm were associated with higher 2‑year mortality in the ROC curve analysis. These parameters could have prognostic significance in patients with severe TR and should be reviewed thoroughly in further studies.
Limitations
A major limitation of our study is a relatively small number of included patients and its retrospective nature. Another limitation is the fact that RH catheterization was not routinely performed in the studied patients and full characteristics of PH could not be performed. Although consecutive patients were enrolled, some selection bias cannot be excluded. Furthermore, this is a single‑center experience.
Conclusions
Patients presenting with severe TR are characterized by large comorbidity burden and high mortality despite intensive HF management. The choice of treatment method should be made based on disease‑specific risk‑stratification tools, such as TRI‑SCORE scale, to avoid the risk of underestimation. RV function is one of the most important predictive factors in TR, and echocardiographic parameters of RV function (TAPSE <17 mm and TAPSE/SPAP ratio <0.26) are associated with mortality.
- Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio‑Thoracic Surgery (EACTS). Eur J Cardiothorac Surg. 2012; 42: S1‑S44.
- Mangieri A, Montalto C, Pagnesi M, et al. Mechanism and implications of the tricuspid regurgitation: from the pathophysiology to the current and future therapeutic options. Circ Cardiovasc Interv. 2017; 10: e005043. | Crossref
- Arsalan M, Walther T, Smith RL, 2nd, et al. Tricuspid regurgitation diagnosis and treatment. Eur Heart J. 2017; 38: 634‑638.
- Lancellotti P, Tribouilloy C, Hagendorff A, et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2013; 14: 611‑644. | Crossref
- Lancellotti P, Moura L, Pierard LA, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur J Echocardiogr. 2010; 11: 307‑332. | Crossref
ARTICLE INFORMATION