Validation of the Fibromyalgia Rapid Screening Tool in patients with axial spondyloarthritis: Polish version adaptation and value in clinical practice
1 ,
Key words: axial spondyloarthritis, fibromyalgia, Fibromyalgia Rapid Screening Tool, Polish, validation
,
Key words: axial spondyloarthritis, fibromyalgia, Fibromyalgia Rapid Screening Tool, Polish, validation

 CC BY 4.0
CC BY 4.0
Validation of the Fibromyalgia Rapid Screening Tool in patients with axial spondyloarthritis: Polish version adaptation and value in clinical practice
Introduction: Fibromyalgia frequently co‑occurs with axial spondyloarthritis. The Fibromyalgia Rapid Screening Tool (FiRST) is a well‑recognized screening tool for fibromyalgia and has been translated into multiple languages. Yet, it has not been adapted into Polish, nor has it been validated in the context of axial spondyloarthritis.
Objectives: This study aimed to create a Polish version of the FiRST, evaluate its psychometric properties, and conduct its validation among patients with axial spondyloarthritis.
Patients and methods: We translated and performed a cross‑cultural adaptation of the FiRST into Polish, followed by its validation in a cohort of 174 patients with axial spondyloarthritis. For criterion validity, we employed the 2016 American College of Rheumatology fibromyalgia diagnostic criteria as the gold standard for fibromyalgia diagnosis.
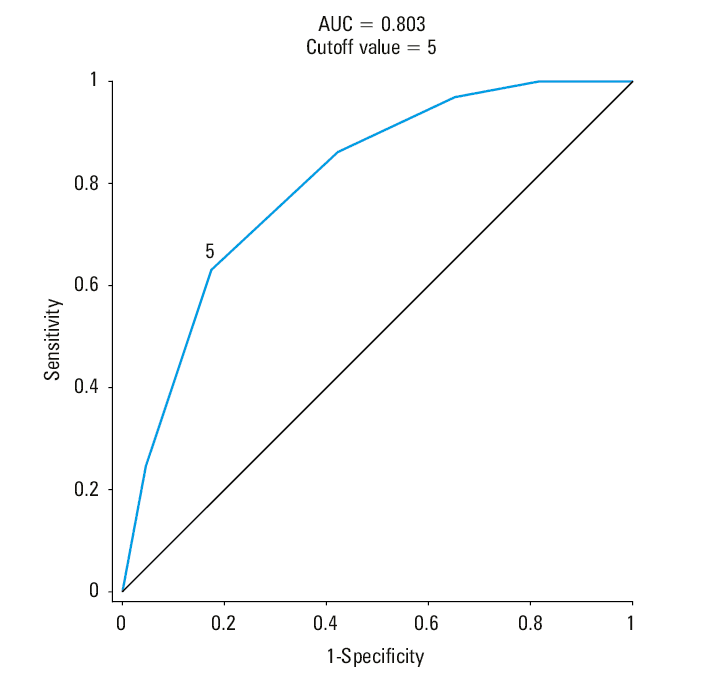
Results: The Polish version of the FiRST demonstrated marginally acceptable internal consistency with the Cronbach α coefficient of 0.644, but exhibited high test‑retest reliability, with a global score correlation coefficient of 0.75 (P <0.001). Receiver operating characteristic analysis indicated a good performance of the translated questionnaire (area under the curve of 0.803). The accuracy of the derived cutoff value for the global score (5+ points, consistent with the original instrument) was 75.3%, featuring higher specificity (82.6%) than sensitivity (63.1%), and a fair level of diagnostic agreement, as indicated by the Cohen κ coefficient of 0.46.
Conclusions: Our study provided a validated Polish version of the FiRST. Although it may not be an ideal tool for screening in axial spondyloarthritis cases and should be used cautiously in research, it proves to be a useful instrument in daily clinical settings.
What's new?
Fibromyalgia Rapid Screening Tool (FiRST) is a user‑friendly screening test for fibromyalgia. However, until now, the Polish version of the FiRST has not been available. Our study is the first to introduce and validate the Polish version of the FiRST, demonstrating that the translation maintains strong psychometric properties. Additionally, although the FiRST is frequently used in research involving patients with axial spondyloarthritis, it has not been formally validated in this group. Our research indicates that the diagnostic efficacy of the FiRST in patients with axial spondyloarthropathy is limited, primarily due to its relatively low sensitivity.
Introduction
Fibromyalgia (FM) is a condition characterized by chronic widespread pain accompanied by fatigue as well as sleep, cognitive, and mood disorders. FM is a common comorbidity in axial spondyloarthritis (axSpA). According to various estimates, it occurs in 13% to 60% of patients with axSpA, depending on the classification / diagnostic criteria used.1 When studies with different criteria were combined, a meta‑analysis showed FM prevalence of 16.4% in axSpA.2 According to another meta‑analysis, FM in axSpA is more prevalent in women (women to men ratio 3:2) and those without human leukocyte antigen (HLA)-B27 antigen (only 45% of patients with FM are HLA‑B27–positive).3 The impact of FM on the life of patients with axSpA is significant. As compared with patients without FM, those with FM show significantly higher disease activity, worse physical functioning, and lower quality of life as measured by the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), the Bath Ankylosing Spondylitis Functional Index (BASFI), and the Ankylosing Spondylitis Quality of Life scale, respectively.1,3 The diagnosis of FM also increases the risk (odds ratio [OR], 4; 95% CI, 1.2–13.1) of a diagnostic delay of axSpA.4 The influence of FM on treatment response (including to biologics) remains unclear, as studies show both a worse response in axSpA patients with FM vs without FM5,6 and a comparable one.7 Nevertheless, the coexistence of FM may distort assessment of the true effectiveness of biologics (which is currently based on patient‑reported outcome measures [PROMs]), resulting in faster drug switching.8,9
A diagnosis of FM is based on diagnostic criteria. The 2016 American College of Rheumatology (ACR) diagnostic criteria10 are a usable tool for diagnosing FM in axSpA patients.11 Unfortunately, in everyday clinical practice, there is often no time to diagnose FM using this rather complicated instrument. However, in 2010, an FM screening tool for patients with diffuse pain was developed, that is, Fibromyalgia Rapid Screening Tool (FiRST).12 It is a PROM consisting of 6 questions to which the patients answer “yes” or “no.” Positive answers to 5 or more questions allow for FM diagnosis. In a development study12, the FiRST showed sensitivity of 90.5% and specificity of 85.7% (area under the curve [AUC] of 0.93) in diagnosing FM (according to the 1990 ACR criteria), while also showing good consistency of the test over time (intraclass correlation coefficient, 0.87). As of today, the FiRST has been translated and validated into several languages, showing good psychometric properties.13-18 However, there is no Polish language version of the tool. Moreover, although the FiRST is often used in studies in axSpA patients to determine the prevalence of FM,19-24 it has actually never been validated in this group of patients. We found only 1 study with axSpA patients that used the FiRST and the 1990 ACR classification criteria at the same time, and which showed a rather poor agreement between the screening test and the classification criteria (κ coefficient = 0.35).5 Therefore, our aim was to prepare a Polish translation of the FiRST screening tool and analyze its psychometric properties in axSpA patients in terms of reliability, factor structure, and validity.
Patients and methods
Translation
The translation and cross‑cultural adaptation process began after obtaining permission from the Mapi Research Trust, and was performed according to the Mapi’s linguistic validation manual and good clinical practice25 in 3 steps including forward translation, backward translation, and patient testing. The English version of the FiRST was translated into Polish by 2 specialists who are native Polish speakers fluent in English, a rheumatologist and a clinical psychologist. After reaching a consensus within the research team, the Polish version was backtranslated by a bilingual (Polish and English) translator who was independent of the research team and did not have access to the original questionnaire. The backtranslated version was compared with the source instrument, showing no conceptual discrepancies between both versions. Pilot testing (cognitive interviews) of the Polish version with 10 axSpA patients (with and without FM) confirmed clarity, and no further adaptations of the translation were required. The Polish version of the FiRST was proofread and the results were reported to the Mapi Research Trust. The final Polish version of FiRST (Supplementary material, Questionnaire) was then administered to all recruited patients in a paper form. While there is no consensus on the required sample size to validate the psychometric properties of questionnaires,26,27 Terwee et al28 suggest a sample size of 7 times the number of items in the questionnaire and a minimum of 100 subjects. In our study, we therefore established a minimum sample size of 100 patients.
Patients
The study was conducted at the Department of Rheumatology, National Institute of Geriatrics, Rheumatology, and Rehabilitation in Warsaw, Poland, between July 2022 and July 2023. It included patients with axSpA (regardless of peripheral involvement). The inclusion criteria were axSpA diagnosis according to the 2010 Assessment of Spondyloarthritis International Society (ASAS) criteria29 and age of at least 18 years. The patients were classified as having ankylosing spondylitis (AS), if they met the modified New York criteria,20 as having psoriatic arthritis (PsA), if they met the classification for psoriatic arthritis criteria,29 or as having nonradiographic spondyloarthritis (nrSpA), if they met only the ASAS criteria.30 The exclusion criterion was any diagnosed mental illness other than depression or anxiety disorders. The study protocol was approved by the hospital bioethics committee (KBT‑3/1/2021). All participants signed their informed consent for inclusion in the study. The study was conducted according to the Declaration of Helsinki.
Validation study
The FiRST reliability was assessed using 2 methods: internal consistency and absolute stability. Internal consistency of the Polish version of the FiRST was analyzed by calculating the Cronbach α coefficient. One week after the first administration, test‑retest reliability of the questionnaire was assessed in a randomly selected group of patients via the online questionnaire. This stage followed the consensus‑based standards for the selection of health measurement instrument recommendations for test‑retest assessment.31 Reliability of each item was assessed by calculating the Cohen κ coefficient, and the global score was assessed by calculating the Spearman correlation coefficient.
The factor structure of the FiRST was examined using the exploratory factor analysis, that is, principal component analysis with the Varimax (orthogonal) rotation and maximum likelihood procedure. The sampling adequacy was detected with the Kaiser–Meyer–Olkin test and the Bartlet test of sphericity. Two criteria for the factor detection were used: eigenvalue (>1) and scree plot.
Several methods of validity estimation were employed. For the criterion validity, we used the 2016 ACR FM diagnostic criteria as the gold standard for diagnosing FM. Receiver operator characteristic (ROC) analysis was performed. The AUC and the Youden index (to identify the most relevant cutoff value) were calculated. The sensitivity, specificity, and accuracy (diagnostic agreement percent) values of the FiRST were calculated for each of the 6 items, and for the global score using the obtained cutoff value. Additionally, positive predictive value (PPV) and negative predictive value (NPV) were calculated from FM prevalence in our study and obtained specificity and sensitivity of the global score. The diagnostic agreement between the diagnoses based on the 2016 ACR criteria and the FiRST global score (using the obtained cutoff point) were assessed by calculating the Cohen κ coefficient.
We tested the construct validity by assessing various clinical outcomes, including FM indicators (widespread pain index [WPI], symptom severity scale [SSS]), pain (numeric rating scale [NRS]), anxiety (Generalized Anxiety Disorder 7]), depression (Patient Health Questionnaire‑9 [PHQ9]), fatigue (Multidimensional Fatigue Scale [MFI Total]), sleep disorders (Jenkins Sleep Scale [JSS]), axSpA disease activity (BASDAI, Ankylosing Spondylitis Disease Activity Score [ASDAS]), and disability [BASFI]). The correlation coefficients between each clinical outcome and the FiRST were calculated, and the differences between patients with and without a FM diagnosis based on the 2016 ACR FM diagnostic criteria and the FiRST test were measured.
Statistical analysis
Compliance of the data with normal distribution was assessed using the Shapiro–Wilk test. Variables with normal distribution were presented as mean (SD), those without normal distribution as median and min‑max range, and qualitative variables as number and percentage. In a subgroup analysis, when a variable did not follow the normal distribution in any of the examined subgroups, it was presented as median (min‑max range). The correlation was determined using the Spearman rank correlation coefficient for non‑normally distributed variables. Significance of the observed differences between the groups was assessed using the t test for the variables with normal distribution, the Mann–Whitney test for the variables with non‑normal distribution, and the χ2 test for categorical variables (or the Fisher exact test for expected frequencies below 5). Statistical analysis was performed using Statistica 13.3 software (StatSoft Polska, Kraków, Poland). A P value below 0.05 was deemed significant.
Results
Patient characteristics
The study involved 174 patients with axSpA (95 with AS, 54 with nrSpA, and 25 with PsA). Among all patients, 65 (37.4%) were diagnosed with FM according to the 2016 ACR diagnostic criteria. Patient characteristics are presented in Table 1. There were significant differences between the patients with and without FM. The first group included more women (64.6% vs 45%; P = 0.01), the patients were older (median, 44 vs 39 years [min‑max, 18–73 vs 19–74]; P = 0.02), less frequent HLA‑B27–positive (63.1% vs 81.4%; P = 0.008), and had higher BASDAI (median, 6.5 vs 4.2 [min‑max, 2.7–10 vs 0–9.6]; P <0.001), ASDAS (mean [SD], 3.37 vs 2.62 [1.1 vs 1.3]; P <0.001), BASFI (median, 6.7 vs 2.9 [min‑max, 0.5–9.8 vs 0–8.9]; P <0.001), MFI total (mean [SD], 73.4 vs 55.6 [12.4 vs 16.4]; P <0.001), JSS (median, 10 vs 4.5 [min‑max, 0–20 vs 0–20]; P <0.001), and PHQ9 (median, 10 vs 6.5 [min‑max, 0–23 vs 0–16]; P <0.001) scores. Importantly, the groups did not differ in the treatment they received (mostly nonsteroid anti‑inflammatory drugs, with only a minority on biologic / targeted synthetic disease‑modifying antirheumatic drugs [b/tsDMARDs]).
Parameter | FM (n = 65) | No FM (n = 109) | P value | |
Data are presented as number and percentage or median and min‑max range unless stated otherwise.
a Patients were classified as having or not having peripheral joint involvement by the attending physician.
Abbreviations: AS, ankylosing spondylitis; ASDAS, Ankylosing Spondylitis Disease Activity Score; axSpA, axial spondyloarthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BMI, body mass index; b/tsDMARDs, biologic / targeted synthetic disease‑modifying antirheumatic drugs; cDMARDs, conventional disease‑modifying antirheumatic drugs; FM, fibromyalgia; GAD‑7, Generalized Anxiety Disorder 7; JSS, Jenkins Sleep Scale; MFI, Multidimensional Fatigue Scale; nrSpA, nonradiographic spondyloarthritis; NSAIDs, nonsteroidal anti‑inflammatory drugs; PHQ9, Patient Health Questionnaire‑9; PsA, psoriatic arthritis | ||||
Age, y | 44 (18–73) | 39 (19–74) | 0.02 | |
Women | 42 (64.6) | 49 (45) | 0.01 | |
BMI, kg/m2 | 25.9 (17.3–42.3) | 24.5 (16–39.5) | 0.14 | |
HLA‑B27–positive | 41 (63.1) | 83 (81.4) | 0.008 | |
axSpA diagnosis | AS | 33 (50.8) | 62 (56.9) | 0.43 |
nrSpA | 21 (32) | 33 (30.3) | 0.78 | |
PsA | 11 (16.9) | 14 (12.8) | 0.47 | |
ASAS criteria, radiologic arm | 54 (83.1) | 85 (81.7) | 0.56 | |
Peripheral joint involvementa | 42 (64.6) | 68 (66) | 0.77 | |
Enthesitis | 27 (41.5) | 35 (34) | 0.21 | |
Treatment | NSAIDs | 46 (70.8) | 68 (62.4) | 0.26 |
cDMARDs | 14 (21.5) | 27 (24.8) | 0.63 | |
b/tsDMARDs | 7 (10.8) | 21 (19.3) | 0.14 | |
Antidepressants | 10 (15.4) | 9 (8.3) | 0.14 | |
Coanalgesics | 9 (13.8) | 10 (9.2) | 0.34 | |
axSpA activity, BASDAI | 6.5 (2.7–10) | 4.2 (0–9.6) | <0.001 | |
axSpA activity, ASDAS, mean (SD) | 3.37 (1.11) | 2.62 (1.31) | <0.001 | |
Functional limitation, BASFI | 6.7 (0.5–9.8) | 2.9 (0–8.9) | <0.001 | |
Fatigue, MFI Total, mean (SD) | 73.4 (12.4) | 55.6 (16.4) | <0.001 | |
Sleep disturbance, JSS | 10 (0–20) | 4.5 (0–20) | <0.001 | |
Depression, PHQ9 | 10 (0–23) | 6.5 (0–16) | <0.001 | |
Anxiety, GAD7, mean (SD) | 10.4 (5) | 8.2 (4.9) | 0.06 | |
Psychometric properties
To verify the factor structure of the FiRST, we performed the exploratory factor analysis. The basic assumptions of the factor analysis were met. Sampling adequacy measured by the Kaiser–Meyer–Olkin test was 0.667 and was satisfactory (recommended above 0.5). The value of the determinant of the correlation matrix (showing the strength of correlations between items) was 0.289 (recommended close to 0). Both analyses of the structure based on eigenvalues and scree plots showed that 2 factors could be extracted. Factor analysis with the Varimax rotation demonstrated that 2 factors explained 56.4% of the total variance. The first one, explaining 33.7% of the total variance, was created by items 1, 2, and 6 of the FiRST questionnaire (α coefficient equal to 0.69). The second, explaining 22.7% of the total variance, was created by items 3 and 4 of the FiRST questionnaire with α coefficient equal to 0.36 (Table 2). Item 5 of the questionnaire was not included in any of the isolated factors. The results suggest a more complex structure of the FiRST questionnaire, but due to a lack of sufficient clarity and poor internal consistency of the subscales, we decided to treat it as a unidimensional tool in further analysis.
Parameter | Factor 1 | Factor 2 |
FiRST Item 2 | 0.898 | 0.105 |
FiRST Item 6 | 0.893 | 0.109 |
FiRST Item 1 | 0.514 | 0.193 |
FiRST Item 4 | –0.005 | 0.84 |
FiRST Item 3 | 0.184 | 0.624 |
FiRST Item 5 | 0.349 | 0.452 |
The Polish version of the FiRST showed a borderline internal consistency with the Cronbach α coefficient of 0.644. As shown in Supplementary material, Table S1, removal of any item does not improve the α coefficient. The test‑retest reliability was assessed in 80 randomly selected axSpA patients after 1 week. The test‑retest reliability for each item varied with the Cohen κ coefficient between 0.48 to 0.76 (Supplementary material, Table S2), while the global score showed a good Spearman correlation coefficient of 0.75 (P <0.001).
The ROC analysis showed the same global score cutoff point (≥5 points) for the Polish version of the FiRST as in the original instrument, with good performance of the translated questionnaire (AUC = 0.803; Figure 1). The accuracy of the obtained cutoff value of the global score was 75.3%, with better specificity (82.6%) than sensitivity (63.1%); PPV was 68.3% and NPV was 78.9%. The sensitivity, specificity, and accuracy for each of the 6 items are shown in Supplementary material, Table S3. The diagnostic agreement between the 2016 ACR criteria and the FiRST global score showed a fair Cohen κ coefficient of 0.46. The patients with false‑negative diagnosis did not differ from true‑positive patients, except for lower PHQ9 scores (Supplementary material, Table S4). However, false‑positive patients had higher BASDAI, BASFI, MFI Total, JSS, and PHQ9 scores than the true‑negative individuals (Supplementary material, Table S5).
The FiRST global score showed good convergence with the WPI (ρ = 0.6; P <0.001), SSS (ρ = 0.62; P <0.001), and NRS (ρ = 0.49; P <0.001), as presented in Supplementary material, Table S6. However, we could not assess discriminant validity, as the patients with and without FM significantly differed in the disease activity, functional limitations, fatigue, depression, sleep disorders, and anxiety (based on both the 2016 ACR diagnostic criteria as shown in Table 1 and the FiRST as shown in Supplementary material, Table S5).
Discussion
The FiRST was originally developed in French and English and has been translated according to the Mapi Research Trust website into Arabic, German, Greek, Portuguese, Spanish, Turkish, and Ukrainian.32 The linguistic validation (with results available in English) was performed for Arabic,15 Greek,17 Portuguese,16 Spanish,13,14 and Turkish18 versions. In comparison with other language versions, the Polish version of the FiRST showed slightly lower internal consistency (Cronbach α of 0.644 vs 0.7–0.787)13,15,17 and comparable test‑retest reliability (ρ = 0.75 vs 0.76–0.875).15,18 The criterion validity of the Polish version of FiRST was comparably good (AUC = 0.803 vs 0.76–0.9).13,14,16,17 However, there were significant differences in the specificity and sensitivity between our and the other language versions. In the other versions, the specificity was lower (55%–87.4%) than the sensitivity (83.8%–92.3%),13,14,16-18 while in our case, the specificity was higher (82.6%) than the sensitivity (63.1%). This discrepancy was most likely due to different groups of patients in which the validations were carried out (axSpA in our case vs patients with chronic pain in the remaining studies). To determine whether the observed difference in specificity and sensitivity is attributable to different patient groups or the translation itself, additional research with the Polish version of the FiRST in different patient groups is required. In the axSpA group, FM is associated with higher disease activity,1,3,32-36 limited functioning,1,3,32-36 greater severity of fatigue,34,35 depression,32-34 and sleep disorders.34,36 These results were replicated by our study. Therefore, we were unable to assess the discriminant validity of the Polish version of the FiRST.
The results of the exploratory factor analysis provided new insight into the structure of the tool. Unlike previous studies, our findings suggest that it might not be unidimensional but may include specific components. Their interpretation seems consistent with the understanding of FM and available diagnostic criteria. The isolated first factor created by items 1, 2, and 6 of the FiRST questionnaire corresponds to the WPI and SSS of the ACR diagnostic criteria. The isolated second factor created by items 3 and 4 of the FiRST questionnaire corresponds to the neuropathic nature of the pain experienced by patients with FM. Item 5, which is not included in any of the identified factors, is the most nonspecific, as it concerns various psychosomatic ailments and symptoms in patients with FM. However, item loadings within individual factors showed considerable variation and the potential subscales did not achieve sufficient internal consistency. Thus, at this stage of the validation, we can still consider the FiRST questionnaire as a unidimensional tool. Further studies with confirmatory factor analysis in a larger sample are needed.
In our study, 37.4% of the patients with axSpA were diagnosed with FM, which is consistent with literature data. Although the FiRST showed good accuracy for screening purposes, the accuracy does not appear to be sufficient for scientific purposes. If the FiRST were used to diagnose FM in our study, out of 174 patients with axSpA 24 would be left with undiagnosed FM, while 19 would be incorrectly diagnosed with FM. The factors that mainly resulted in the false‑negative diagnosis of FM in the FiRST in axSpA patients were questions regarding pain in the whole body (item 1), other psychosomatic ailments (item 5), and the neuropathic nature of the symptoms (item 3). Among the patients with FM undiagnosed by the FiRST, the above questions were answered negatively by 75%, 66.6%, and 62.5% of respondents, respectively. The factor that resulted in the false‑positive diagnosis of FM in the FiRST in the patients with axSpA was the presence of pain in at least 4 out of 5 body regions. Among the respondents with falsely diagnosed FM based on the FiRST, 100% of patients did not meet this criterion. The above results show that the 2016 ACR diagnostic criteria determine the widespread pain much more precisely than the FiRST in patients with axSpA, and not all patients with axSpA and FM experience pain of the neuropathic nature (which is not included in the ACR criteria) or other psychosomatic ailments (which contribute little to meeting the 2016 ACR criteria). These results suggest that the limited sensitivity and, to a lesser extent, specificity of the FiRST are probably due to differences in the perception of FM‑related symptoms in patients with axSpA, as compared with other patients with chronic widespread pain. What seems disturbing, is the widespread use of the FiRST for diagnosing FM in axSpA patients in scientific research.19-24 In studies with large patient groups, it may be tempting to use a short and simple PROM rather than a full clinical assessment. However, the FiRST has not yet been validated properly in axSpA patients. Apart from ours, there is only 1 study that briefly validated the use of the FiRST in the axSpA group. It checked the diagnostic agreement in patients with axSpA between the FiRST and 1990 ACR classification criteria, showing a rather poor agreement with κ coefficient of 0.35.5 The issue of diagnostic agreement between The FiRST and diagnostic criteria in patients with axSpA therefore requires further research (preferably based on the original language versions to exclude the influence of translation on the results).
Strengths and limitations
Our study provides the first validated translation of the FiRST into Polish. The strength of the study is its extensive validation, taking into account internal consistency, absolute stability, criterion, and construct validity. Given the comparable psychometric properties of the Polish language version with other language versions of the FiRST, in our opinion, the Polish version may tentatively be used in everyday clinical practice in patients with axSpA. Our study’s both a strength and a limitation is the fact that it focuses on a narrow group of patients with axSpA. The study is the first reliable validation of the FiRST among patients with axSpA. Its results, when confirmed in axSpA patients using other language versions of the FiRST, may significantly limit the use of the FiRST in research studies. Still, a specific group of axSpA patients necessitates a cautious approach to generalizing the use of the Polish translation of the FiRST in other patient groups. Our results require confirmation in subsequent studies among patients with chronic widespread pain, as well as other inflammatory joint diseases, which we plan to perform. Until then, the Polish version of the FiRST should not be used in patients other than those with axSpA. Another limitation is the fact that the study involved axSpA patients with high disease activity, most of whom were not treated with b/tsDMARDs (most patients were awaiting qualification for b/tsDMARD treatment in the therapeutic program of the National Health Fund). It needs to be verified whether the performance of the FiRST is comparable among patients with low disease activity and / or in remission.
Conclusions
The FiRST questionnaire is a quick, easy‑to‑use screening tool that can be used in daily clinical practice. Given the good NPV of the Polish version of the instrument, the FiRST in the axSpA group can be used to screen for the exclusion of FM during everyday clinical practice. However, if FM is suspected based on the FiRST, because of lower PPV and observed significant differences between false‑positive patients and true‑negative patients, full assessment should be performed using the 2016 ACR diagnostic criteria to confirm FM diagnosis (Figure 2). Additionally, in our opinion, the use of the FiRST should be avoided in research studies in patients with axSpA until further studies validating its use are available.
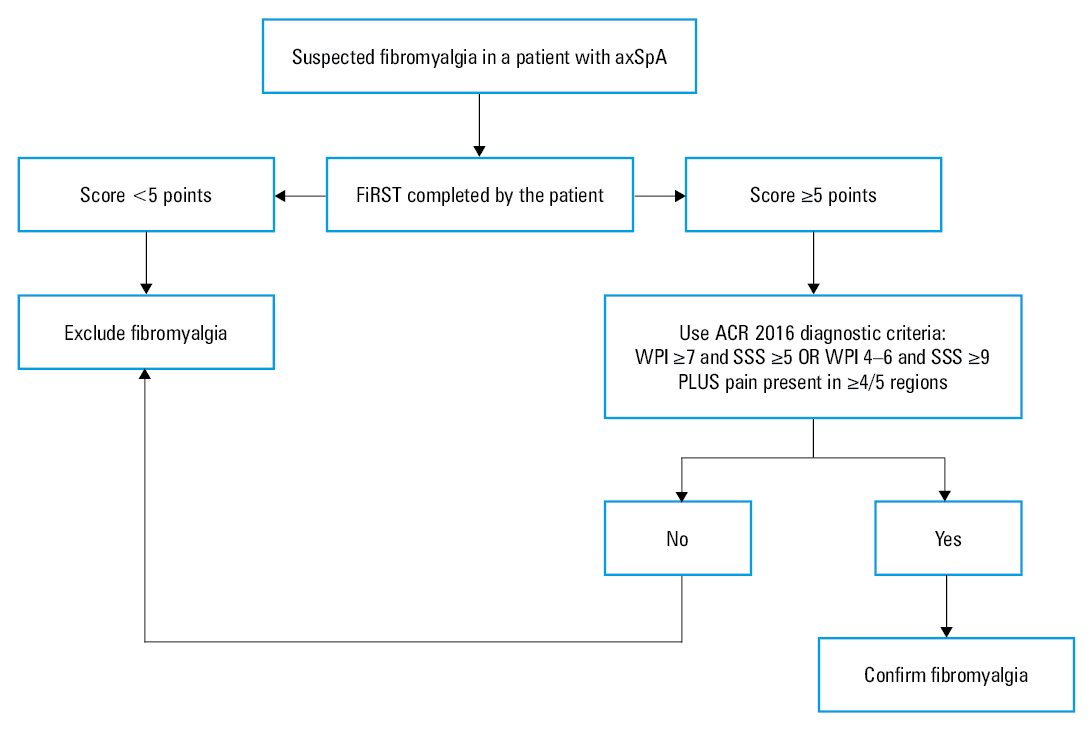
Abbreviations: ACR, American College of Rheumatology; FiRST, Fibromyalgia Rapid Screening Tool; SSS, symptom severity scale; WPI, widespread pain index
- Alunno A, Carubbi F, Stones S, et al. The impact of fibromyalgia in spondyloarthritis: from classification criteria to outcome measures. Front Med (Lausanne). 2018; 5: 290. | Crossref
- Jones GT, Mallawaarachchi B, Shim J, et al. The prevalence of fibromyalgia in axial spondyloarthritis. Rheumatol Int. 2020; 40: 1581‑1591. | Crossref
- Son SM, Kim DS, Lee JS. Fibromyalgia in axial spondyloarthritis: a meta‑analysis. J Clin Rheumatol. 2022; 28: E222‑E227. | Crossref
- Parada‑Arias L, Vargas JF, Ahcar NS, et al. Factors associated with diagnostic delay of axial spondyloarthritis in Colombian patients. J Clin Rheumatol. 2022; 28: 126‑131. | Crossref
- Moltó A, Etcheto A, Gossec L, et al. Evaluation of the impact of concomitant fibromyalgia on TNF alpha blockers’ effectiveness in axial spondyloarthritis: results of a prospective, multicentre study. Ann Rheum Dis. 2018; 77: 533‑540. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION