A 26‑year‑old patient came to an outpatient urology clinic due to a lesion on the ventral surface of his penis. The patient has been observing the lesion for many years. The reason for his visit to the clinic was difficulty in having sexual intercourse due to the size of the lesion making the coitus impossible. On physical examination an, oval lesion was palpable on the ventral surface of the penis, lateral to the perineal raphe at one‑third of the organ length (Figure 1A). The lower edge of the lesion was visible at the border of the penile skin and the scrotum. The lesion was painless and moveable on palpation.
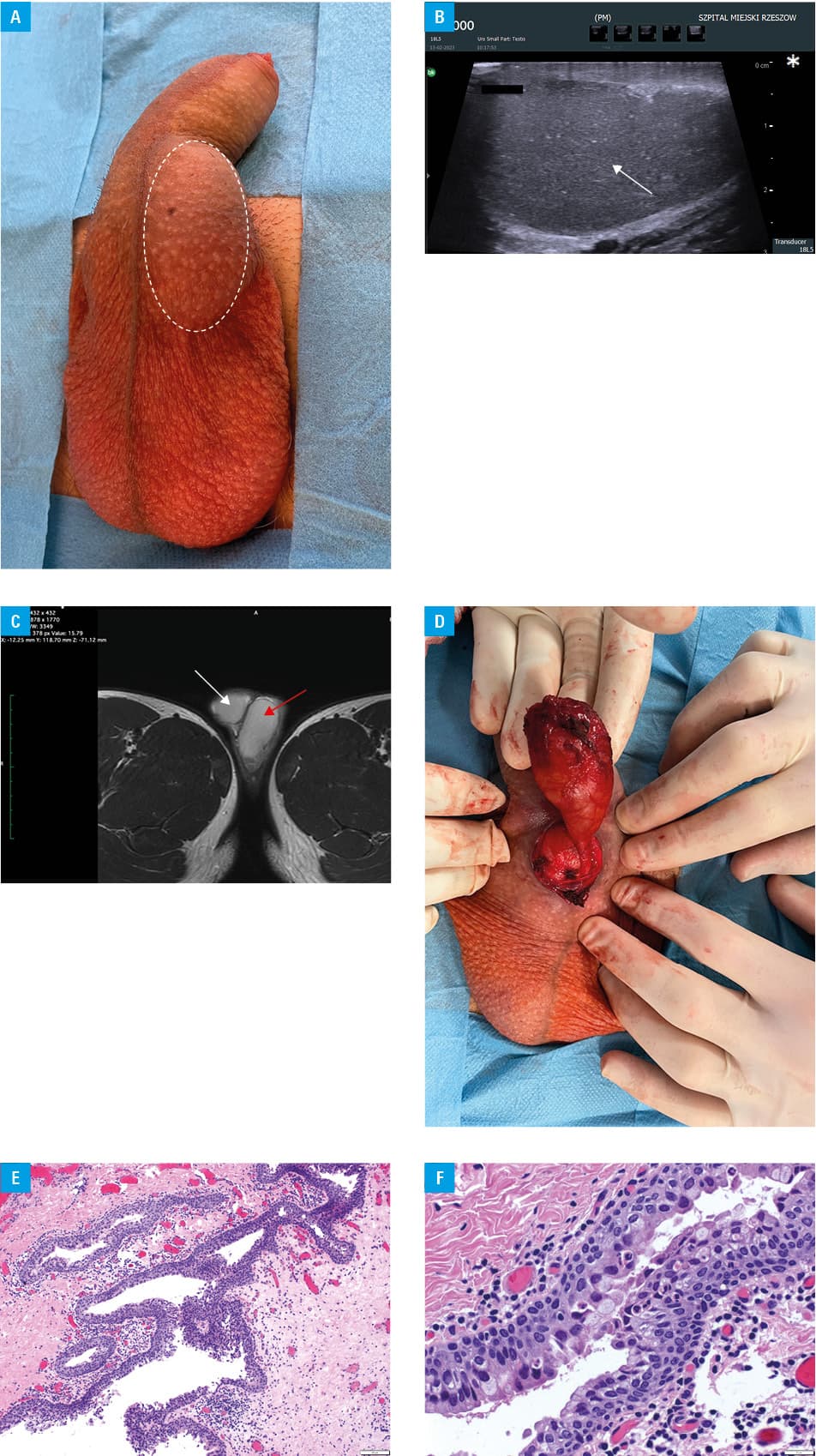
Ultrasound showed an oval structure with homogeneous echogenicity comparable to a testicular structure with a sparse marginal vascular flow (Figure 1B). Due to the ultrasound image of the lesion suggesting triorchidism, magnetic resonance imaging (MRI) of the scrotum was performed. An oval lesion was also visualized on MRI, the structure of which hinted at the presence of a third testis (Figure 1C). The patient was scheduled for revision surgery of the lesion. During the procedure, an oval‑shaped structure located between the penile skin and the penile tunica albuginea was dissected; the lesion had no visible vascular supply, with a blind‑ended duct (Figure 1D). Intraoperatively, the decision was made to remove the lesion. The entire lesion was sent for histopathologic examination. The procedure was carried out without complications. Histopathologic examination shown a median raphe cyst (Figure 1E and 1F). The patient was followed‑up for 3 months. The excision site healed without any residual effect. There were no issues related to sexual activity.
The median raphe cyst is a rare benign congenital lesion that develops in men on the median line, anywhere from the external urethral orifice to the perineum. The penile shaft is the most common location at presentation, regardless of the age of the patient.1 A majority of the cysts do not reach a size greater than 1 cm.2 The lesion is reported by parents in childhood, or appears later in the second or third decade of life, due to the onset of symptoms during micturition or sexual intercourse, but also for cosmetic reasons. A differential diagnosis that a clinician should bear in mind includes: glomus tumor, dermoid cyst, pilonidal cyst, epidermal inclusion cyst, and urethral diverticulum.3There are a few potential explanations for the origin of these cysts. Embryologic defective closure of the central part of the urethra may be one of them. Another explanation is abnormal development of the ectopic periurethral glands of Littré. The third theory is anomalous germination, and later separation, of the urethral columnar epithelium from the urethra. Excision and subsequent primary closure remain the treatment of choice, and yield cosmetically acceptable results.4 Observation is a possible option when the cyst is small with no clinical manifestation to the patient. Cases of spontaneous cyst resolution have also been reported.5
- Amaranathan A, Sinhasan SP, Dasiah SD. Median raphe cysts of the prepucial skin, with triple histological linings: a case report and review of the literature. J Clin Diagn Res. 2013; 7: 1466‑1468. | Crossref
- Navalón‑Monllor V, Ordoño‑Saiz MV, Ordoño‑Domínguez F, et al. Median raphe cysts in men. Presentation of our experience and literature review. Actas Urol Esp. 2017; 41: 205‑209. | Crossref
- Alphones S, Phansalkar M, Manoharan P. Median raphe cyst of the penis: a startling diagnosis for the unaccustomed clinician. Urol Ann. 2019; 11: 314‑316. | Crossref
- Matsuyama S, Matsui F, Yazawa K, et al. Long‑term follow‑up of median raphe cysts and parameatal urethral cysts in male children. Urology. 2017; 101: 99‑103. | Crossref
- Syed MMA, Amatya B, Sitaula S. Median raphe cyst of the penis: a case report and review of the literature. J Med Case Rep. 2019; 13: 214. | Crossref
ARTICLE INFORMATION