Selective androgen receptor modulator abuse–induced heart failure: catastrophic effects of RAD-140 (Testolone)

 CC BY 4.0
CC BY 4.0
Selective androgen receptor modulator abuse–induced heart failure: catastrophic effects of RAD-140 (Testolone)
Although implementation of androgenic steroid hormones may be beneficial in numerous medical conditions, their therapeutic utilization is often limited by possible adverse effects.1,2 To overcome the restrictions arising from global activation of androgen receptors, selective androgen receptor modulators (SARMs) are being developed. SARMs are a class of tissue‑selective receptor ligands that have similar anabolic properties to anabolic steroids, but with reduced side effects.3 Moreover, due to their anabolic action, they are gaining popularity among athletes and bodybuilders.4 We report a rare case of a young man in whom SARM abuse resulted in catastrophic clinical condition with severe heart failure (HF).
A 22‑year‑old man who has been training weightlifting was admitted to a hospital with symptoms of severe HF (New York Heart Association [NYHA] class III) with tachypnea and severe leg edema. The patient did not have any risk factors for HF and his medical history was unremarkable. Exertional dyspnea had worsened over the last 3 months. Chest X‑ray showed pulmonary edema and heart enlargement. On electrocardiography, sinus rhythm of 75 bpm with signs of left ventricular [LV] hypertrophy and inverted T waves in leads V1–V6 were observed. Laboratory tests showed an elevated level N‑terminal pro–B-type natriuretic peptide (4482 pg/ml; reference range, 0–125 pg/ml).
The patient admitted to SARM (RAD‑140; Testolone) abuse over the last 6 months. The drug was self‑administered in cycles of 8 weeks, without any intervals between the cycles.
Echocardiography showed LV end‑diastolic diameter (LVEDD) enlargement (82 mm) with a reduced LV ejection fraction (LVEF) of 15% and global hypokinesis (Figure 1A). Cardiac magnetic resonance imaging confirmed LVEDD enlargement with global hypokinesis and signs of subepicardial and mid‑wall LV fibrosis, possibly corresponding to toxic or postinflammatory myocardial damage (Figure 1B–1D).5
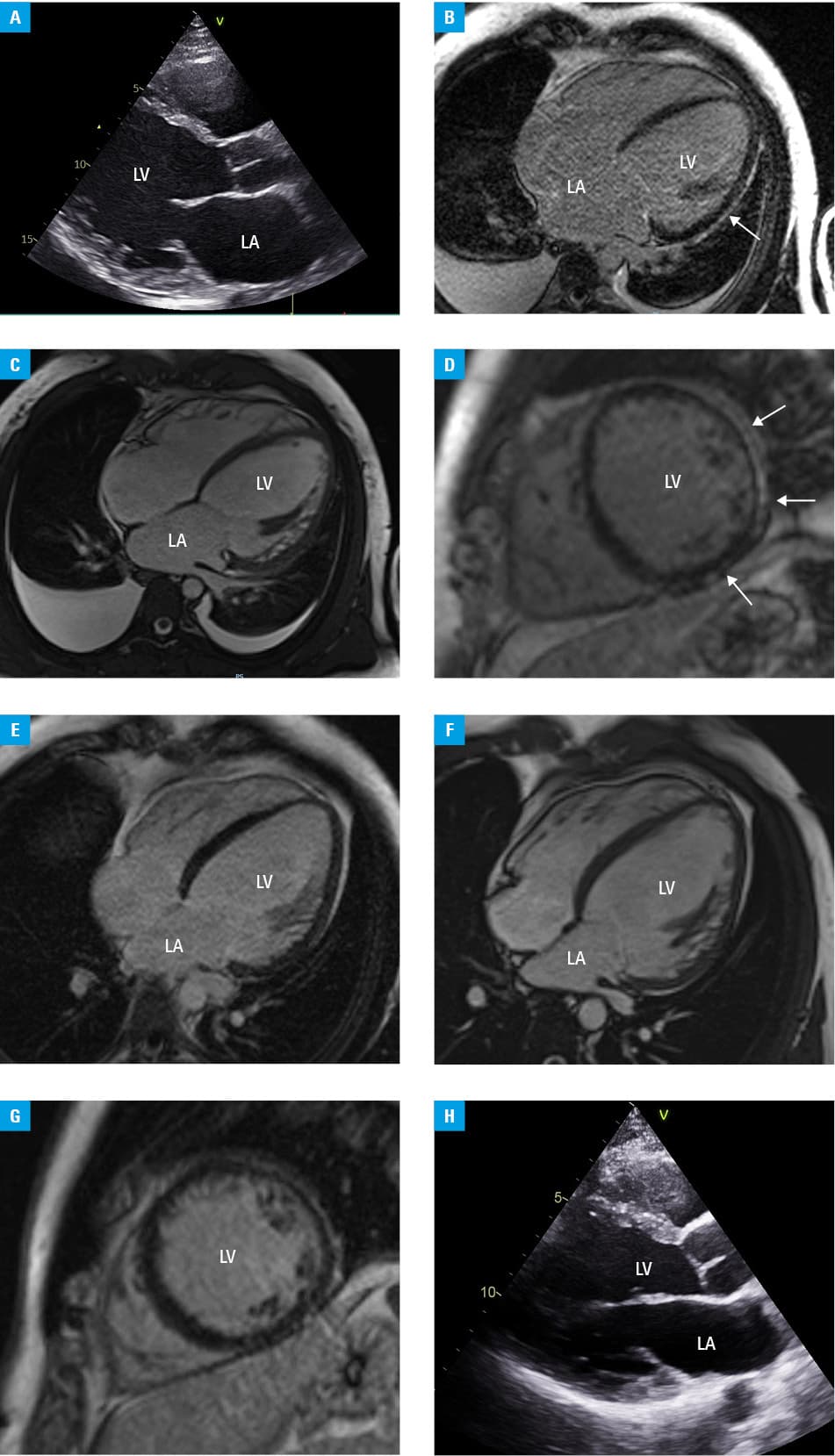
Adequate modern pharmacologic treatment of HF was implemented, and the patient was recommended to stop SARM abuse. A rapid uptitration strategy was adopted, and the patient reached the maximum optimal angiotensin receptor / neprilysin inhibitor dose 1 month after discharge. At the 2‑month follow‑up, his clinical condition improved, HF symptoms reduced to NYHA class I/II, and LVEF increased by up to 25%. Optimal pharmacotherapy was continued. At the 5‑month follow‑up, further improvement was noted, with reduction of LVEDD to 68 mm and LVEF increase to 35% (Figure 1E–1G). After 9 months, a reduction of LVEDD to 67 mm and an increase of LVEF to 40% were observed (Figure 1H).
We report a peculiar case, where excessive use of SARMs led to a severe HF. However, it seems that clinical improvement is achievable following SARM discontinuation and optimal medical treatment implementation. This report highlights the potentially disastrous consequences of SARM intake and underscores the importance of cautionary advice against their usage.
- Crawford J, Prado CMM, Johnston MA, et al. Study design and rationale for the phase 3 clinical development program of enobosarm, a selective androgen receptor modulator, for the prevention and treatment of muscle wasting in cancer patients (POWER trials). Curr Oncol Rep. 2016; 18: 1‑11. | Crossref
- Skorupska K, Skorupski W, Gąsiorowski M, et al. Disastrous effects of anabolic steroids abuse: a peculiar case of heart failure and toxic hepatitis in a young bodybuilder. Pol Arch Intern Med. 2022; 132: 16355. | Crossref
- Christiansen AR, Lipshultz LI, Hotaling JM, et al. Selective androgen receptor modulators: the future of androgen therapy? Transl Androl Urol. 2020; 9: 135‑148. | Crossref
- Van Wagoner RM, Eichner A, Bhasin S, et al. Chemical composition and labeling of substances marketed as selective androgen receptor modulators and sold via the Internet. JAMA. 2017; 318: 2004‑2010. | Crossref
- Klotzka A, Kufel‑Grabowska J, Zembala M, et al. Is anthracycline‑induced heart failure reversible? Kardiol Pol. 2020; 78: 1295‑1296. | Crossref
ARTICLE INFORMATION