Outcomes in patients with definite and possible infective endocarditis related to a cardiac implantable electronic device
Key words: definite and possible lead-related infective endocarditis, diagnostic criteria, long-term survival, risk factors, transvenous lead extraction

 CC BY 4.0
CC BY 4.0
Outcomes in patients with definite and possible infective endocarditis related to a cardiac implantable electronic device
Introduction: Diagnosing lead‑related infective endocarditis (LRIE) often poses a substantial challenge. Current diagnostic criteria include definite and possible LRIE.
Objectives: The aim of this study was to compare the outcomes of patients with definite and possible LRIE undergoing transvenous lead extraction (TLE) procedures.
Patients and methods: A retrospective analysis of data from 3782 patients undergoing TLE between 2006 and 2023 was performed. The study included 838 patients with definite and possible LRIE, whose clinical data on short- and long‑term survival were evaluated.
Results: The comparison of clinical data showed more frequent occurrences of vegetations (81.58% vs 37.21%; P <0.001), positive blood cultures (66.12% vs 51.64%; P <0.001), and septic pulmonary embolism (40.14% vs 13.78%; P <0.001) in the patients with definite LRIE. Long‑term mortality of patients with definite and possible LRIE (median [interquartile range] follow‑up, 4.61 [1.04–9.4] and 5.06 [2.07–8.75] years, respectively) was 61.14% and 49.29% (P <0.001). Predictors of mortality in patients with definite LRIE included: advanced age, low left ventricular ejection fraction (LVEF), comorbidities, septic pulmonary embolism, positive blood culture, and presence of an abandoned lead. In possible LRIE, only the influence of advanced age, low LVEF, and comorbidities was demonstrated. There was no documented evidence of a direct impact of a delayed diagnosis on the long‑term survival of patients after TLE.
Conclusions: The study showed better survival in patients with possible LRIE than with definite LRIE, which confirms the need to extend the diagnostic criteria. Introducing appropriate treatment at an early stage of infection improves the prognosis.
What's new?
Lead‑related infective endocarditis (LRIE) is the most dangerous infection of a cardiac implantable electronic device and one that is associated with high mortality rates. It requires prompt detection and management. Diagnosing LRIE is often difficult due to nonspecific symptoms, and early detection is important, so that the patient can be sooner qualified for transvenous lead extraction and begin adequate antibiotic therapy. This study is the first to assess the impact of expanded diagnostic criteria on the diagnosis and prognosis of patients with LRIE. The study included a large patient group and prolonged follow‑up. A comparison of clinical data and risk factors for death in patients with definite and possible LRIE showed that detecting the infection at an earlier stage through the use of extended diagnostic criteria may improve the long‑term survival of patients receiving appropriate treatment.
Introduction
Infections in patients with cardiac implantable electronic devices (CIEDs) are a serious complication associated with an unfavorable prognosis. The prevalence of infectious complications showed by retrospective studies was 0.5%–4.4%,1,2 while current prospective studies put it at 0.3%–2.3%.3-5 The most dangerous type of infection in people with CIED is lead‑related infective endocarditis (LRIE). LRIE may occur with or without pocket infection, lead, or tricuspid valve‑related vegetations. Diagnosing LRIE, especially without pocket infection, often poses a challenge due to uncharacteristic symptoms that make it difficult to quickly introduce appropriate treatment. Diagnostic problems have contributed to a search for new LRIE‑specific criteria. Subsequent guidelines of the European Society of Cardiology (ESC)6,7 and the European Heart Rhythm Association (EHRA)8 suggested expanding the Duke criteria to include local pocket infection, septic pulmonary embolism (SPE), and positive lead cultures, as well as results of new imaging testing (18F‑fluorodeoxyglucose‑positron emission tomography / computed tomography [18F‑FDG‑PET/CT], white blood cell single‑photon emission CT / CT [WBC SPECT/CT]). Moreover, in the ESC guidelines6,7 infective endocarditis was divided into definite and possible. The introduction of the term “possible LRIE” should facilitate detection of this insidious disease and increase referrals for transvenous lead extraction (TLE). So far, the literature does not include any analyses of patients diagnosed with possible infective endocarditis. This study’s aim was to compare diagnostics, treatment, and long‑term survival in patients undergoing TLE due to definite and possible LRIE.
Patients and methods
Study cohort
A retrospective analysis of a computer database of 3782 patients undergoing TLE at 3 high‑volume centers was conducted by 1 key operator (AK) between March 2006 and January 2023. The study included 838 patients undergoing TLE for LRIE classified as definite and possible. A comparative analysis investigated clinical data, TLE procedural data, and short- and long‑term survival of patients with possible and definite LRIE. As many as 410 of 622 patients (65.92%) with definite LRIE and 152 of 216 patients (70.37%) with possible LRIE were referred to TLE from other hospitals, sometimes in remote areas of Poland. Therefore, the authors had no influence on the duration and accuracy of the original diagnostic process. Written informed consent was obtained from all patients involved in the study.
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study protocol and consent to publication were approved by the Bioethics Committee at the Regional Chamber of Physicians in Lublin (288/2018/KB/VII).
Definitions
LRIE was defined according to the 2015 and 2023 ESC guidelines for management of infective endocarditis and the EHRA consensus document,6-8 as an infection involving leads, cardiac valve leaflets, or endocardial surface. The diagnosis of LRIE was made based on the 2019 International CIED Infection Criteria.8 The major criteria included: 1) microbiologic assays (blood cultures positive for typical microorganisms found in CIED infection and / or IE, microorganisms consistent with IE from 2 separate blood cultures, or microorganisms consistent with IE from persistently positive blood cultures) and; 2) imaging positive for CIED infections and / or IE (echocardiogram including intracardiac echocardiography) including: clinical pocket / generator infection, lead vegetation, valve IE, vegetations, abscess, pseudoaneurysm, intracardiac fistula, valvular perforation or aneurysm, new partial dehiscence of the prosthetic valve, and 18F‑FDG‑PET/CT or radiolabeled WBC SPECT/CT de‑tection of abnormal activity at pocket / generator site, along the leads or at the valve site, and definite paravalvular leakage on cardiac CT.
Minor Duke criteria included: 1) predisposition, such as predisposing heart condition (eg, new onset tricuspid valve regurgitation), or use of injected drugs; 2) fever above 38 ˚C; 3) vascular phenomena (including those detected only on imaging), such as major arterial emboli, septic pulmonary embolism, infectious (mycotic) aneurysms, intracranial hemorrhage, conjunctival hemorrhages, and Janeway lesions; 4) microbiologic evidence in the form of a positive blood culture which does not meet a major criterion, as noted above, or serologic evidence of an active infection with an organism consistent with IE, culture of material obtained from the pocket or the leads (extracted via the noninfected pocket). Definite LRIE was diagnosed if 2 major criteria or 1 major and 3 minor criteria were met. Possible LRIE was diagnosed when the presence of 1 major and 1 minor criterion or 3 minor criteria was confirmed.
Pocket infection is defined as an infection limited to the generator pocket with local signs of inflammation, such as erythema, elevated temperature, and enhanced mobility, sometimes with threatened erosion or dehiscence of the wound and purulent drainage, exposed generator or proximal leads.6-8
TLE was defined according to the Heart Rhythm Society and EHRA statements,8-10 as a procedure where at least 1 lead removal required equipment not typically employed during lead implantation or at least 1 lead was implanted for more than 1 year.
Intracardiac abrasion of the leads was defined as damage to the outer lead tube (isolation) in the intracardiac section (15–20 cm from the tip of the lead).11
Management
All patients with LRIE underwent TLE and antibiotic therapy. TLE was performed within 7 days since the diagnosis. Following the procedure, the patients returned to their referring centers, and continued their antibiotic therapy there for 4 to 6 weeks, as recommended.
Statistical analysis
Continuous data, due to their nonparametric distribution, are presented as a median with interquartile range (IQR). Categorical data are presented as number and percentage and were compared with the nonparametric Mann–Whitney test and the Pearson χ2 test or the χ2 test with Yates correction, respectively. Death risk factors were estimated using multivariable linear regression. Data with P value below 0.05 obtained in the Mann–Whitney test and the χ2 test were included in the regression analysis. To present survival after TLE, the Kaplan–Meier curves were plotted. The differences in their shape were assessed using the log‑rank test. Statistical significance was established as P value below 0.05. The statystical analysis was performed with Statistica package version 13.3 (TIBCO Software Inc., Palo Alto, California, United States).
Results
Ultimately, 838 patients with LRIE were analyzed, including 622 individuals with definitive LRIE diagnosis and 216 with possible LRIE. The analysis of clinical data for patients with definite and possible LRIE showed that renal failure was more frequent in the definite LRIE group, and antiplatelet therapy was used more often in these patients. Vegetations and positive blood cultures, especially of Staphylococcus aureus, were also more common in the patients with definite LRIE. The patients with possible LRIE had higher prevalence of pocket infection (64.81% vs 51.29%; P <0.001). A comparative analysis of minor Duke criteria showed higher prevalence of SPE, fever, and shivers in the patients with definite LRIE. Similarly, all laboratory inflammatory parameters showed higher values in these patients. The first symptoms of LRIE were most oftenly nonspecific and included recurrent fevers of initially unknown etiology and recurrent pneumonia—a manifestation of SPE. For this reason, the time from the onset of the first symptoms to diagnosis was long, that is, on average 3 months for definite LRIE and 2 months for possible LRIE. A detailed comparative analysis of the time from the onset of the first symptoms to diagnosis of definite and possible LRIE is presented in the Supplementary material, Table S1.
In some patients, diagnostic difficulties are also indicated by the number of hospitalizations related to atypical manifestations (fever of unknown origin, recurrent pneumonia, anemia). Our analysis showed that more than 1 hospitalization was recorded in as many as 232 patients (37.3%) with definite LRIE and 64 patients (29.63%) with possible LRIE, and 3 or more hospitalizations in 76 individuals (12.06%) with definite LRIE and 18 cases (8.33%) with possible LRIE. Also, the number of hospitalizations due to LRIE symptoms (per 1 patient) in retrospective assessment was 1.6 in the definite LRIE group and 1.38 in the possible LRIE group. The median (IQR) in both groups was 1 (1–2), but the analysis demonstrated that in 25% of patients with definitive and possible LRIE (155 patients with definitive LRIE and 54 pateints with possible LRIE) it took, respectively, at least 6 and 5 months from the onset of the first symptoms of LRIE to TLE (Table 1).
Parameter | Definite LRIE | Possible LRIE | P value | ||
Assessed patients, na | Value, n (%) | Assessed patients, na | Value, n (%) | ||
Data are reported as median (interquartile range) or number (percentage).
a Number of patients with complete data
SI conversion factors: to convert hemoglobin to g/l, multiply by 10.
Abbreviations: BMI, body mass index; CoNS, coagulase‑negative Staphylococci; CRP, C‑reactive protein; ESR, erythrocyte sedimentation rate; LRIE, lead‑related infective endocarditis; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; SPE, septic pulmonary embolism; TLE, transvenous lead extraction | |||||
Age at TLE, y | 622 | 71 (61–78) | 216 | 71 (60–79) | 0.88 |
Age at the first system implantation, y | 622 | 63 (54–71) | 216 | 63 (53–72) | 0.9 |
Women | 622 | 184 (29.58) | 216 | 67 (31.02) | 0.76 |
BMI, kg/m2 | 606 | 28 (25.28–29.72) | 210 | 27.73 (24.45–29.87) | 0.51 |
LVEF, % | 618 | 50 (35–60) | 215 | 50 (35–60) | 0.56 |
NYHA functional class | 622 | 2 (1–2) | 216 | 2 (1–2) | 0.73 |
Prosthetic or biological valve present | 622 | 41 (6.59) | 216 | 15 (6.94) | 0.98 |
Permanent atrial fibrillation | 622 | 142 (22.83) | 216 | 63 (29.17) | 0.08 |
Chronic anticoagulation | 622 | 233 (37.46) | 216 | 92 (42.59) | 0.21 |
Chronic antiplatelet therapy | 622 | 274 (44.05) | 216 | 76 (35.19) | 0.03 |
Diabetes mellitus | 622 | 174 (27.97) | 216 | 54 (25) | 0.45 |
Chronic kidney disease | 614 | 206 (33.55) | 213 | 53 (24.88) | 0.02 |
Charlson comorbidity index, points | 622 | 5 (3–9) | 216 | 4 (3–9) | 0.24 |
Major Duke criteria | |||||
Vegetations | 619 | 505 (81.58) | 215 | 80 (37.21) | <0.001 |
Vegetations connected with a lead | 505 | 427 (84.55) | 80 | 67 (83.75) | 0.99 |
Median vegetation size, cm2 | 500 | 0.64 (0.25–1.61) | 77 | 0.5 (0.21–1.5) | 0.12 |
Pocket infection | 622 | 319 (51.29) | 216 | 140 (64.81) | <0.001 |
Positive blood culture | 614 | 406 (66.12) | 213 | 110 (51.64) | <0.001 |
Staphylococcus aureus | 614 | 101 (16.45) | 213 | 14 (6.57) | <0.001 |
Staphylococcus epidermidis | 614 | 153 (24.92) | 213 | 53 (24.88) | 0.94 |
CoNS | 614 | 30 (4.89) | 213 | 7 (3.29) | 0.44 |
Other staphylococci | 614 | 58 (9.45) | 213 | 24 (11.27) | 0.53 |
Streptococci | 614 | 7 (1.14) | 213 | 0 | 0.26 |
Other bacteria | 614 | 57 (9.28) | 213 | 12 (5.63) | 0.1 |
Negative blood culture | 614 | 139 (22.64) | 213 | 48 (22.54) | 0.89 |
Unknown result of blood culture | 614 | 69 (11.24) | 213 | 55 (26.29) | <0.001 |
Antibiotic therapy before blood culture | 553 | 418 (75.59) | 197 | 107 (54.31) | <0.001 |
Minor Duke criteria | |||||
SPE | 553 | 222 (40.14) | 196 | 27 (13.78) | <0.001 |
Positive culture from the lead | 512 | 258 (50.39) | 182 | 90 (49.45) | 0.9 |
Fever / shivers | 553 | 375 (67.81) | 198 | 78 (39.39) | <0.001 |
Laboratory parameters | |||||
Anemia (Hb <12 g/dl) | 611 | 329 (53.85) | 210 | 91 (43.33) | 0.01 |
CRP, mg/l | 606 | 30 (14–54.5) | 208 | 13.6 (3.5–40) | <0.001 |
ESR, mm | 239 | 30 (41) | 98 | 19.5 (9–43.5) | 0.01 |
Procalcitonin, ng/ml | 247 | 0.16 (0.07–1.06) | 59 | 0.1 (0.04–0.16) | <0.001 |
Time from the onset of first symptoms to LRIE diagnosis | |||||
Time, mo | 622 | 3 (1–6) | 216 | 2 (1–5) | 0.01 |
Number of hospitalizations for LRIE symptoms [mean per 1 patient] | 622 | 1 (1–2) [1.6] | 216 | 1 (1–2) [1.38] | 0.02 |
Intracardiac abrasion of the lead was observed more often in the patients with definite LRIE (29.42% vs 18.52%; P <0.001). Analysis of the remaining CIED‑related factors did not show any significant differences between the possible and definite LRIE groups (Table 2).
Parameter | Definite LRIE | Possible LRIE | P value | |||
Assessed patients, na | Value | Assessed patients, na | Value | |||
Data are reported as median (interquartile range) or number (percentage)
a Number of patients with complete data
Abbreviations: CIED, cardiac implantable electronic device; CRT, cardiac resynchronization therapy; ICD, implantable cardioverter‑defibrillator; others, see Table 1 | ||||||
Number of leads | 622 | 2 (2–2) | 216 | 2 (2–2) | 0.37 | |
Sum of dwell time of leads in a single patient, y | 622 | 11.5 (5.33–21.67) | 216 | 13.67 (6–21.33) | 0.13 | |
Dwell time of the oldest extracted lead in the patient, y | 622 | 6.5 (3.17–10.92) | 216 | 7 (3.33–10.5) | 0.53 | |
Device therapy | Pacemaker | 622 | 420 (67.52) | 216 | 141 (65.28) | 0.92 |
ICD | 135 (21.7) | 44 (20.37) | 0.35 | |||
CRT | 67 (10.78) | 31 (14.35) | 0.36 | |||
Presence of abandoned lead | 622 | 109 (17.52) | 216 | 32 (14.81) | 0.42 | |
Intracardiac abrasion of the lead | 622 | 183 (29.42) | 216 | 40 (18.52) | <0.001 | |
Excessive loop of the lead | 622 | 38 (6.11) | 216 | 10 (4.63) | 0.53 | |
Previous CIED‑related procedures | 622 | 2 (1–3) | 216 | 2 (1–3) | 0.13 | |
Time interval since the last procedure prior to TLE, mo | 622 | 24 (9–51) | 216 | 20 (8–50) | 0.21 | |
Early reintervention (latest CIED‑related procedure <2 months before) | 622 | 35 (5.63) | 216 | 11 (5.09) | 0.9 | |
Procedural success of TLE | 622 | 587 (94.37) | 216 | 207 (95.76) | 0.9 | |
Clinical success of TLE | 622 | 589 (94.69) | 216 | 209 (96.76) | 0.29 | |
Major complications of TLE | 622 | 11 (1.77) | 216 | 5 (2.31) | 0.83 | |
Minor complications of TLE | 616 | 53 (8.6) | 215 | 19 (8.84) | 0.97 | |
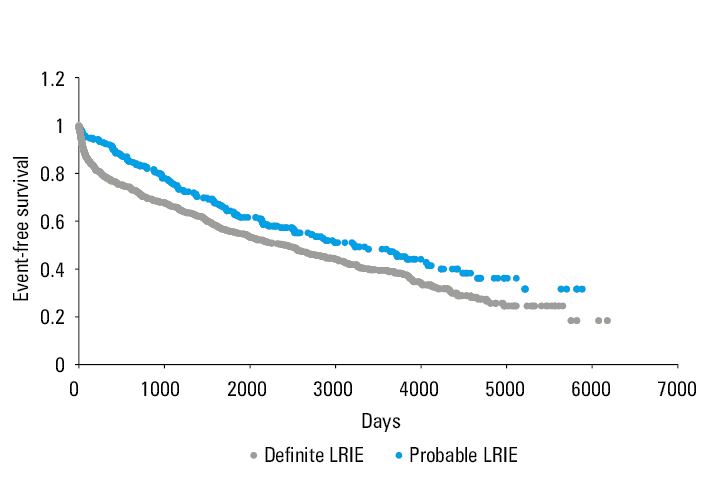
In‑hospital mortality of patients with definite and possible LRIE was comparable (P = 0.17). Thirty‑day, 1‑year, 3‑year, and long‑term survival was better in the patients with probable LRIE (median [IQR] follow‑up, 5.06 [2.07–8.75] years) than for definite LRIE (median [IQR] follow‑up, 4.61 [1.04–9.4] years; P <0.001) (Table 3, Figure 1).
Parameter | Definite LRIE | Possible LRIE | P value | ||||
Assessed patients, na | Alive, n (%) | Dead, n (%) | Assessed patients, na | Alive, n (%) | Dead, n (%) | ||
a Number of patients with complete data
b Median (interquartile range) follow‑up, 4.66 (1.01–9.41) years for definite LRIE and 5.67 (2.6–8.98) years for probable LRIE (P = 0.036).
Abbreviations: see Table 1. | |||||||
In‑hospital mortality (up to 7 days after TLE) | 615 | 604 (98.21) | 11 (1.89) | 211 | 210 (99.53) | 1 (0.47) | 0.17 |
30‑day mortality after TLE | 615 | 577 (93.82) | 38 (6.18) | 211 | 206 (97.63) | 5 (2.37) | 0.03 |
1‑year mortality after TLE | 602 | 465 (77.24) | 137 (22.76) | 186 | 169 (90.86) | 17 (9.14) | <0.001 |
3‑year mortality after TLE | 585 | 381 (65.13) | 204 (34.87) | 177 | 128 (72.31) | 49 (27.69) | <0.001 |
Long‑term mortality after TLEb | 615 | 239 (38.86) | 376 (61.14) | 211 | 107 (50.71) | 104 (49.29) | <0.001 |
Multivariable analysis identified the following prognostic factors of long‑term mortality in the patients with definite LRIE: age at TLE, decreased LVEF, higher Charlson comorbidity index, SPE, positive blood culture, and presence of abandoned lead (Table 4).
Long‑term mortality after TLE | Univariable analysis | Multivariable analysis | |||||
Assessed patients, na | Alive, n (%) | Assessed patients, na | Dead, n (%) | P value | OR (95% CI) | P value | |
Age at TLE, y | 240 | 58.5 (46–68) | 376 | 65 (57–72.5) | <0.001 | 1.049 (1.027–1.071) | <0.001 |
Women | 240 | 84 (35) | 376 | 98 (26.1) | 0.02 | 0.697 (0.411–1.180) | 0.18 |
LVEF, % | 239 | 56 (44.5–60.5) | 375 | 47.5 (30–58) | <0.001 | 0.97 (0.952–0.987) | 0.001 |
Charlson comorbidity index, points | 240 | 4 (2–6) | 376 | 5 (4–10) | <0.001 | 1.105 (1.026–1.189) | 0.008 |
Time from the first symptom to LRIE diagnosis, mo | 240 | 2 (1–6) | 376 | 3 (1–6) | 0.09 | – | – |
Presence of vegetation | 238 | 204 (85.71) | 373 | 297 (79.62) | 0.056 | – | – |
Lead‑connected vegetation | 177 | 171 (96.6) | 273 | 256 (93.8) | 0.27 | – | – |
Median size of vegetations, cm2 | 201 | 0.55 (0.25–1.53) | 296 | 0.71 (0.25–1.61) | 0.68 | – | – |
Pocket infection | 240 | 135 (56.3) | 376 | 183 (48.7) | 0.01 | 0.851 (0.51–1.422) | 0.54 |
Staphylococcus aureus | 238 | 34 (14.3) | 376 | 67 (17.8) | 0.3 | – | – |
Staphylococccus epidermidis | 238 | 60 (25.2) | 376 | 93 (24.7) | 0.97 | – | – |
CoNS | 238 | 5 (2.1) | 376 | 25 (6.6) | 0.02 | 2.374 (0.733–7.689) | 0.15 |
Other staphylococci | 238 | 16 (6.72) | 376 | 42 (11.12) | 0.09 | – | – |
Streptococci | 238 | 5 (2.1) | 376 | 2 (0.5) | 0.16 | – | – |
Other bacteria | 238 | 18 (7.56) | 376 | 39 (10.37) | 0.3 | – | – |
Negative blood culture | 238 | 68 (28.6) | 376 | 71 (18.9) | <0.001 | – | – |
SPE | 206 | 68 (33) | 347 | 154 (44.4) | 0.01 | 1.66 (1.006–2.741) | 0.047 |
Positive culture from the lead | 203 | 94 (46.3) | 309 | 164 (53.1) | 0.16 | – | – |
Positive blood culture | 238 | 138 (55.46) | 376 | 268 (71.28) | <0.001 | 1.629 (1.011–2.626) | 0.04 |
Anemia (Hb<12 g/dl) | 236 | 106 (44.9) | 375 | 223 (59.5) | <0.001 | 1.207 (0.717–2.034) | 0.48 |
CRP, mg/l | 235 | 27.8 (8–86.49) | 371 | 39 (14.11–100.2) | 0.007 | 1.016 (0.981–1.053) | 0.37 |
Number of leads | 240 | 2 (2–2) | 376 | 2 (2–3) | 0.14 | – | – |
HV lead | 240 | 69 (28.8) | 376 | 133 (35.4) | 0.1 | – | – |
CS lead | 240 | 23 (9.6) | 376 | 62 (16.5) | 0.02 | 1.362 (0.636–2.917) | 0.43 |
Presence of abandoned lead | 240 | 31 (12.9) | 376 | 78 (20.7) | 0.02 | 2.814 (1.469–5.392) | 0.002 |
Abrasion of the lead | 240 | 71(29.6) | 376 | 111 (29.5) | 0.94 | – | – |
Number of previous CIED‑related procedures | 240 | 2 (1–2) | 376 | 2 (1–3) | 0.67 | – | – |
Full procedural success of TLE | 240 | 227 (94.6) | 376 | 356 (94.7) | 0.9 | – | – |
Major complications of TLE | 240 | 1 (0.4) | 376 | 10 (2.7) | 0.08 | – | – |
Minor complications of TLE | 240 | 16 (6.7) | 376 | 37 (9.8) | 0.22 | – | – |
According to a multivariable analysis, independent factors for long‑term survival of patients with possible LRIE were: age at TLE, low LVEF, and comorbidities (Table 5).
Long‑term mortality after TLE | Univariable analysis | Multivariable analysis | |||||
Assessed patients, na | Alive, n (%) | Assessed patients, na | Dead, n (%) | P value | OR (95% CI) | P value | |
Age at TLE, y | 108 | 58.5 (47–68) | 107 | 67 (57.5–75.5) | <0.001 | 1.042 (1.012–1.072) | 0.006 |
Women | 108 | 39 (36.1) | 107 | 28 (26.2) | 0.15 | ||
LVEF, % | 107 | 55 (42–60) | 107 | 49.6 (30–57.5) | <0.001 | 0.963 (0.941–0.986) | 0.001 |
Charlson comorbidity index, points | 108 | 3.5 (2–5) | 107 | 5 (4–10) | <0.001 | 1.116 (1.007–1.238) | 0.04 |
Time from the first symptom to LRIE diagnosis, mo | 108 | 2 (1–5) | 107 | 2 (1–5) | 0.69 | – | – |
Presence of vegetation | 104 | 38 (36.54) | 105 | 42 (40) | 0.71 | – | – |
Lead‑connected vegetation | 38 | 30 (78.95) | 42 | 37 (88.1) | 0.42 | – | – |
Median size of vegetations, cm2 | 35 | 0.48 (0.21–1.45) | 41 | 0.6 (0.25–1.6) | 0.36 | – | – |
Pocket infection | 108 | 72 (66.7) | 107 | 67 (62.6) | 0.53 | – | – |
Staphylococcus aureus | 106 | 5 (4.7) | 107 | 9 (8.4) | 0.42 | – | – |
Staphylococcus epidermidis | 106 | 27 (25.5) | 107 | 26 ( 24.3) | 0.97 | – | – |
CoNS | 106 | 3 (2.8) | 107 | 4 (2.7) | 0.99 | – | – |
Other staphylococci | 106 | 14 (13.21) | 107 | 10 (9.35) | 0.50 | – | – |
Streptococci | 106 | 0 | 107 | 0 | – | – | |
Other bacteria | 106 | 4 (3.77) | 107 | 8 (7.5) | 0.38 | – | – |
Negative blood culture | 106 | 20 (18.9) | 107 | 28 (26.2) | 0.27 | – | – |
SPE | 92 | 10 (10.9) | 104 | 17(16.3) | 0.37 | – | – |
Positive culture from the lead | 92 | 46 (50) | 90 | 44 (48.9) | 0.10 | – | – |
Positive blood culture | 106 | 53 (50) | 107 | 57 (53.27) | 0.90 | – | – |
Anemia (Hb <12 g/dl) | 104 | 37 (35.6) | 106 | 54 (50.9) | 0.04 | 1.542 (0.764–3.111) | 0.22 |
CRP, mg/l | 102 | 10.65 (2.81–29.2) | 106 | 17.6 (6.8–55.7) | 0.001 | 1.065 (0.986–1.151) | 0.11 |
Number of extracted leads | 108 | 2 (2–2) | 107 | 2 (2–3) | 0.89 | – | – |
HV lead | 109 | 28 (25.9) | 107 | 36 (33.6) | 0.27 | – | – |
CS lead | 108 | 16 (14.8) | 107 | 17 (15.9) | 0.98 | – | – |
Presence of abandoned lead | 108 | 17 (15.7) | 107 | 15 (14) | 0.87 | – | – |
Abrasion of the lead | 108 | 18 (16.7) | 107 | 22 (20.6) | 0.58 | – | – |
Number of previous CIED‑related procedures in patient | 108 | 2 (1–3) | 107 | 2 (1–3) | 0.12 | – | – |
Full procedural success of TLE | 108 | 102 (94.4) | 107 | 106 (99.1) | 0.13 | – | – |
Major complications of TLE | 108 | 5 (4.6) | 107 | 0 | 0.07 | – | – |
Minor complications of TLE | 108 | 7 (6.5) | 107 | 12 (11.2) | 0.33 | – | – |
Comparison of long‑term survival of patients with definite and probable LRIE depending on the time from the onset of the first symptoms to diagnosis showed no difference in mortality after TLE (Supplementary material, Figure S1 and S2).
Discussion
Despite constant developments in diagnostics and therapy, CIED infections, especially LRIE, continue to be associated with high mortality. In 19 studies that included 100 or more patients with follow‑up up to 5.5 years, all‑cause mortality after CIED infections was as high as 35%.12-21 All studies that included only patients with LRIE reported high mortality of 24.5%–29%, with a maximum of a year of follow‑up.13,20,22 Moreover, 8 studies reporting in‑hospital or 30‑day mortality showed that mortality increased in subsequent observation periods and ranged from 2%–15%13-21 to 24%–29% at 6 months,13,22-24 9%–35% at 1 year,14,19,20,25-28 and 6%–37% at 2 years or longer.14-16,29-33 In our study, the 1‑year and 3‑year mortality equaled 8.1% and 22.3% for patients with possible LRIE, and 22.3% and 33.1% for definite LRIE, and was comparable to literature data. Long‑term follow‑up (5.55 years and 6.05 years for definite and possible LRIE, respectively) showed very high mortality of 61.14% for definite LRIE and 49.29% for possible LRIE. This high mortality rate was probably due to the advanced age of the patients (median age at TLE was 71 years [IQR, 61–58]) and high Charlson index (median, 4 [IQR, 3–9]). There are few publications on long‑term survival of patients with CIED‑related infections, and they are based on small study cohorts. According to a recent study,31 the mortality rate of 191 patients undergoing TLE (50% infectious indications) during 6.5‑year follow‑up was 33%. Another study, which analyzed a cohort of 125 patients with CIED infections, showed a mortality rate of 24% after 41 months of follow‑up,32 and 1 more study with mean follow‑up of 4.1 years demonstrated a 37% mortality rate in 82 patients with CIED‑related infections undergoing TLE.33 The risk factors for death in the long‑term follow‑up in the above studies31-33 were age at TLE, anemia, atrial fibrillation, presence of vegetation, positive blood cultures, and high comorbidity index. Our analysis identified similar factors. The main predictors of long‑term mortality in patients with definite LRIE were age at TLE, decreased LVEF, high Charlson comorbidity index, positive blood cultures, SPE, and presence of an abandoned lead. However, in patients with possible LRIE, only the influence of age, low LVEF, and comorbidities was confirmed. Our analysis showed that patients with possible LRIE had lower long‑term mortality than those with definite LRIE. This is probably related to the use of extended diagnostic criteria, enabling initiation of treatment at an earlier stage (before systemic expansion of the infection), and the more frequent co‑occurrence of pocket infections in this group. The course of infection in our patients with definite LRIE was more severe and featured vegetations, more often more dangerous pathogens, and high values of inflammatory parameters. In this group of patients, abandoned leads and intracardiac abrasion of the leads were also observed more frequently, which indicates a chronic intracardiac infection.
The multivariable analysis showed that the poorer survival of patients with definite LRIE is probably related to the greater extent of the infectious process than in the patients with possible LRIE. Previous studies have mainly confirmed the influence of age and comorbidities on the long‑term prognosis of patients with LRIE, but emphasized that early diagnosis limits formation of vegetation and systemic infection spread thanks to earlier TLE and initiation of appropriate antibiotic therapy.31-34
The often insidious course of the disease, manifested by relapses of fever or recurrent pneumonia in the absence of vegetations visible on echocardiography, significantly delays a correct diagnosis. Ineffective antibiotic therapy also adversely affects long‑term treatment results.36 We noticed a significant delay (up to several months) in diagnosing LRIE 10 years ago, when the diagnostic criteria for LRIE were more strictly adhered to, and valuable time was wasted searching for other causes of fever. This study did not demonstrate a direct impact of delayed diagnosis on the long‑term survival of patients after TLE, and this is probably related to the introduction of less stringent criteria for diagnosing possible LRIE.
Limitations
This is a retrospective, 3‑center study based on patient data entered into a computer database. The patients were referred for TLE from different hospitals across the country, and it was not possible to obtain complete data for all individuals. As many as 65.92% patients with definite LRIE and 70.37% of those with probable LRIE were referred for TLE from other hospitals, and we had no influence over the accuracy of the first diagnostic decisions. We also had no influence over timing of the diagnosis and treatment before the patient was referred for TLE. Although after TLE the patients received recommendations regarding medical treatment and the time of repeated CIED implantation, we were unable to verify if and how these recommendations were implemented.
Conclusions
Long‑term mortality of patients with LRIE is still high, but early diagnosis using extended criteria contributes to improved long‑term survival. Risk factors for mortality in patients with definite LRIE included factors indicating a severe course of infection, while in the case of possible LRIE the distant survival after TLE was related only to old age and multimorbidity. The study did not demonstrate a direct impact of delayed diagnosis on the long‑term survival of patients after TLE, but documented that implementing adequate LRIE therapy at an early stage of the spread of an infection improves the long‑term prognosis.
- Clementy N, Carion PL, de Leotoing L, et al. Infections and associated costs following cardiovascular implantable electronic device implantations: a nationwide cohort study. Europace. 2018; 20: 1974‑1980. | Crossref
- Ludwig S, Theis C, Brown B, et al. Incidence and costs of cardiac device infections: retrospective analysis using German health claims data. J Comp Eff Res. 2018; 7: 483‑492. | Crossref
- Tarakji KG, Mittal S, Kennergren C, et al. Antibacterial envelope to prevent cardiac implantable device infection. N Engl J Med. 2019; 380: 1895‑1905. | Crossref
- Birnie DH, Wang J, Alings M, et al. Risk factors for infections involving cardiac implanted electronic devices. J Am Coll Cardiol. 2019; 74: 2845‑2854. | Crossref
- Krahn AD, Longtin Y, Philippon F, et al. Prevention of arrhythmia device infection trial: the PADIT trial. J Am Coll Cardiol. 2018; 72: 3098‑3109.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION