Periprocedural management of patients on a direct oral anticoagulant undergoing elective gastrointestinal endoscopy
Key words: direct oral anticoagulant, endoscopy, gastrointestinal bleeding, thromboembolism

 CC BY 4.0
CC BY 4.0
Periprocedural management of patients on a direct oral anticoagulant undergoing elective gastrointestinal endoscopy
This narrative review summarizes the current body of literature regarding periprocedural management of direct oral anticoagulant (DOAC)-treated patients undergoing digestive endoscopy since the publication of the 2022 American College of Gastroenterology – Canadian Association of Gastroenterology guidelines. We provide a detailed analysis of the thromboembolic risk, endoscopic procedure–specific bleeding risks, contemporary intraprocedural techniques to reduce the bleeding risk, and a summary of periprocedural DOAC guidelines developed by major gastrointestinal societies, including recommendations on procedure risk stratification. Despite data heterogeneity, the overall trend of the current literature supports the contemporary practice of a minimal DOAC interruption without the need for heparin bridging.
Introduction and background information about direct oral anticoagulants: indications and general pharmacotherapeutic considerations
Antithrombotics have been prescribed increasingly often,1 in particular due to expansion of indications for the use of direct oral anticoagulants (DOACs), which include direct thrombin (dabigatran) and factor Xa inhibitors (eg, rivaroxaban, apixaban, and edoxaban).2 DOACs are increasingly favored over vitamin K antagonists (VKAs) for most patients with atrial fibrillation (AF; except for those with moderate‑severe mitral stenosis and mechanical heart valves), in the initial and long‑term treatment of venous thromboembolism (VTE), and in the prevention of TE disease among individuals undergoing hip or knee arthroplasty.3-5 In the patients requiring dual antithrombotic therapy as a default strategy (anticoagulant and antiplatelet agents), the American College of Cardiology (ACC) recommends DOACs over VKAs.6 DOACs have been associated with an increased risk of gastrointestinal bleeding (GIB) when compared with warfarin7,8; however, the risk can be decreased with the use of proton pump inhibitors, especially in higher‑risk subgroups.6,9-11
Thrombotic risk is the highest in individuals with a mechanical heart valve, AF, or a past TE event. If these patients experience a transient ischemic attack, cerebrovascular event, or TE, elective digestive endoscopy should be postponed for the first 3 months following the event.12 In contradistinction, anticoagulated patients at a moderate or low risk of experiencing a TE event can undergo elective GI endoscopy after weighing the bleeding risks related to continued antithrombotic treatment against the risk of a TE event as a result of its interruption. Critical to such decision making is an understanding of the pharmacokinetics of DOACs, including the rapid drop in anticoagulant activity 24 hours after therapy interruption and its rapid onset within 12 hours after ingestion of a single dose upon resumption, which is affected by renal function, especially among patients on dabigatran.13 As a result, in contrast to initial published experience, current recommendations discourage the use of periprocedural heparin bridging therapy (HBT) in patients in whom temporary interruption of a DOAC is indicated.12-14 Any final decision about DOAC interruption should include appropriate considerations, weighing patient and provider preferences, for a cardiovascular vs a GIB event.12
Methodology
This narrative review discusses evidence from studies performed after publication of the ACC – Canadian Association of Gastroenterology (ACG‑CAG) guidelines on the management of DOAC‑treated patients undergoing digestive endoscopy.12 The current body of literature is constrained by several significant limitations. Notably, there is a paucity of randomized controlled trials (RCTs), and thus a significant risk of biases in the reported results (eg, patient selection, information bias in the available data that may be limited by patient recall, loss to follow‑up, etc.). The existing studies also exhibit considerable heterogeneity in design and outcome definitions, particularly concerning interruption protocols that changed in time, and postprocedural bleeding definitions. These variations complicate the synthesis of findings and interstudy comparability. Additionally, as most studies were conducted in Asia, this geographic concentration may limit the generalizability of the findings to different populations with regards to potential genetic variations, as well as differing anticoagulation protocols—in particular to adjust the international normalized ratio.4,15 Futhermore, disparity among comparative anticoagulation studies included unclear co‑administration of antiplatelet agents in many. An additional confounder is related to the level of precision with which the therapeutic range of warfarin was controlled, as it poses a great challenge in clinical practice. As compared with patients in real‑world clinical settings, individuals treated with warfarin in more supervised settings are much more likely to be strictly monitored, which may lead to a lower risk of GIB.16
Thromboembolic risk
While numerous studies have examined bleeding outcomes in the GI periprocedural context, few have specifically addressed the TE risks associated with DOAC interruption. This review summarizes key findings from recent studies on this topic, including the impact of different interruption protocols. These insights are crucial for optimizing patient care and guiding clinical decisions in the periprocedural setting. We do not refer to meta‑analyses that included a significant proportion of patients on DOACs being bridged, because they analyzed studies performed up to 2020 that no longer reflect the current standard of practice of no HBT for these patients, as mentioned above.
The postcolonoscopy TE risk in patients on DOACs was reported in a recent retrospective cohort study of 247 patients from Hong Kong.17 The 30‑day incidence of a TE event among the patients undergoing DOAC interruption was 0.87%. One of the patients died of myocardial infarction within 4 days of a 6‑day interruption despite heparin bridging. The second patient experienced pulmonary embolism within 7 days following a 3‑day interruption.
In a 4:1 propensity‑matched retrospective analysis of 13 393 Japanese patients undergoing low‑risk biopsies, Konish et al18 compared individuals on uninterrupted DOAC therapy with those not receiving DOACs. The authors reported a stroke rate of 0.07% that did not differ significantly between the groups (odds ratio [OR], 1; 95% CI, 0.21–4.71).
In another study of 1602 anticoagulated patients (598 on a DOAC) who underwent both high- (46.6%, most commonly hot snare polypectomy [HSP] in 41.8%) and low‑risk GI procedures, the 90‑day TE incidence rates did not differ significantly between anticoagulation agents (VKA 1.3% vs DOAC 1.5%; adjusted OR, 0.9; 95% CI, 0.34–2.38), with bridging performed in 17.5% of the DOAC patients.19 The interruption protocol resulted in mean pre- and postprocedural DOAC withholding times of 50.1 and 25.5 hours, respectively.
A large‑scale multicenter Japanese study spanning 11 years investigated patients on various types of DOACs or warfarin undergoing colorectal endoscopic submucosal dissection (ESD).20 The patients on DOACs followed HBT protocols until 2017, after which the DOAC was withheld only on the day of the procedure and resumed 1 day after ESD. All patients were hospitalized for 3 days following the procedure. Among the DOAC patients, the rate of TE events was 0.29% (3/1019), with 2 events occurring 2 days and 1 event occurring 3 days post‑ESD.
In conclusion, although the studies varied in their use of HBT, which is no longer recommended, the periprocedural thrombotic risk for patients on DOACs ranged from 0.07% to 1.5%.
In a meta‑analysis of 17 studies (5 RCTs) assessing principally the removal of polyps up to 1 cm in size, the authors identified the TE risk as similar among patients using and not using periprocedural antithrombotic agents (OR, 1.24; 95% CI, 0.42–3.68).21
Procedural bleeding risk classification
The GI procedural bleeding risk classifications vary across guidelines developed by major societies. A summary of these is shown in Table 1.
Low risk | High risk | Ultrahigh riska |
a Category created by APAGE‑APSDE
b All polypectomies are considered high‑risk by BSG‑ESGE. All polypectomies of polyps ≤2 cm are considered high‑risk by APAGE‑APSDE. ACG‑CAG considers all polypectomies of polyps <1 cm as low‑risk.
c Therapeutic balloon‑assisted enteroscopy is considered high‑risk by ACG‑CAG.
d Classified as low‑risk by ACG‑CAG
Abbreviations: ACG‑CAG, American College of Gastroenterology – Canadian Association of Gastroenterology; APAGE‑APSDE, Asian Pacific Association of Gastroenterology – Asian Pacific Society for Digestive Endoscopy; BSG‑ESGE, British Society of Gastroenterology – European Society of Gastrointestinal Endoscopy; EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection; ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasound; PEG/PEJ, percutaneous endoscopic gastrostomy / jejunostomy | ||
Gastroscopy, sigmoidoscopy, colonoscopy, enteroscopy
Diagnostic push- or device‑assisted enteroscopy | Gastroscopy, sigmoidoscopy, colonoscopy, enteroscopyc
| Gastroscopy, sigmoidoscopy, colonoscopy
|
Solely diagnostic procedures are considered low‑risk
| ERCP
| |
EUS
| EUS
| |
Videocapsule endoscopy | ||
Direct oral anticoagulant administration protocol studies
The following studies present novel evidence on a contemporary periprocedural DOAC administration protocol for patients undergoing GI procedures, and are in keeping with contemporary guidelines.
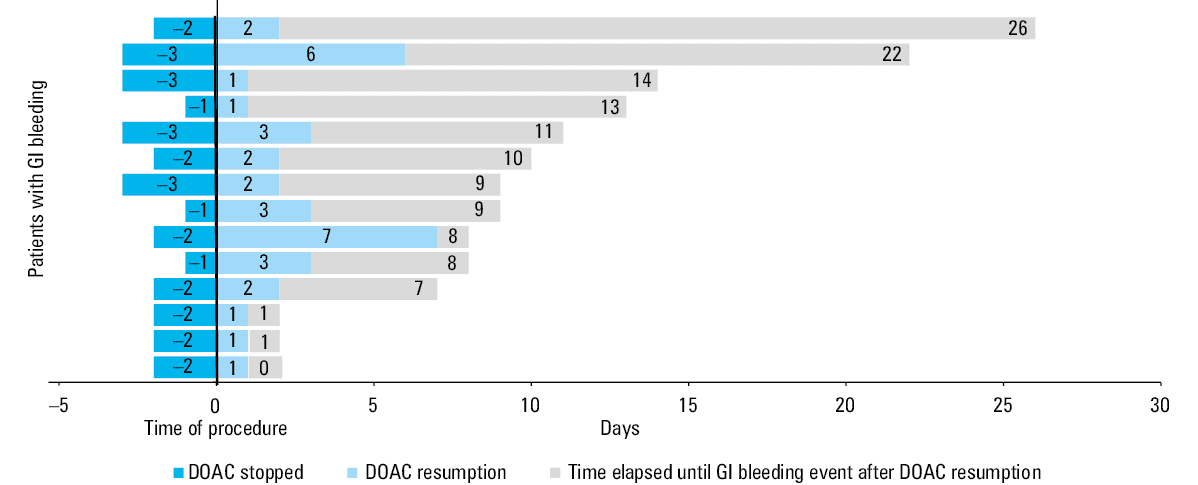
Analysis of the GI subgroup of the PAUSE (Periprocedural Anticoagulation Use for Surgery Evaluation) cohort was the first true prospective study of a representative group of DOAC patients at varying risks of thrombosis scheduled to undergo common endoscopic GI procedures.22 These patients (n = 556) were assigned to a standardized management scheme with defined outcomes and 30‑day follow‑up. The mean (SD) total duration of DOAC interruption was 3.9 (1.6) days. Four patients experienced arterial TE (0.7%; 95% CI, 0.3%–1.8%) within a mean (SD) of 24.2 (5.9) days of DOAC interruption. GIB occurred in 2.5% (95% CI, 1.4%–4.2%) of the participants within 11.1 (8.1) days (range, 0.6–25.5 days) of endoscopy, with major GIB occurring in 0.9% (95% CI, 0.4%–2.1%). Three patients died (0.5%; 95% CI, 0.2%–1.6%) after the endoscopy (range for time of death, 15.6–22.3 days postprocedure). The authors concluded that the use of a contemporary standardized periprocedural management strategy (Figure 1) in patients with AF undergoing DOAC therapy interruption for elective digestive endoscopy resulted in low rates of arterial TE and major bleeding. This study provides essential insights into the safety and efficacy of DOAC management strategies during endoscopic procedures.
Two additional studies provide supplemental information concerning interruption protocols. One of them is a prospective, observational study that compared the risk of postpolypectomy bleeding (PPB) over 2 weeks following cold snare polypectomy (CSP) of polyps up to 1 cm in size in patients who continued DOAC therapy (n = 204) vs those in whom DOACs were withheld on the day of the procedure (n = 264).23 Immediate PPB occurred more often in the DOAC continued group than in the DOAC withheld group (25.5% [95% CI, 15.1%–39.6%] vs 6.1% [95% CI, 1.9%–15%]; P <0.008) with more clip placements in the patients who continued anticoagulation (31.9% vs 9.1%; P <0.005). Delayed bleeding occurred only in the DOAC continued group (8.5% [95% CI, 2.8%–20.5%] vs 0% [95% CI, 0%–6.6%]; P <0.001). The authors thus recommended a policy of withholding DOACs only on the day of colonoscopy in routine clinical practice.
In a post‑hoc analysis of 437 anticoagulated patients (108 on a DOAC) who were included in a randomized trial assessing the role of clips in preventing postpolypectomy complications, 3 individuals experienced a TE event within 90 days.24 In all 3, the anticoagulant was restarted more than 2 days postprocedure (16% of the DOAC patients). However, the exact timing of the TE event as well as the proportion of patients who were on a DOAC vs a VKA were not specified.
These findings further emphasize the importance of tailored anticoagulation management around the time of endoscopic procedures to minimize the TE vs bleeding risks.
Endoscopic modalities to decrease the risk of delayed postprocedural gastrointestinal bleeding
Patients on antithrombotics undergoing digestive endoscopy are at a risk for both intraprocedural (immediate) and delayed GIB, defined variably as up to the ensuing 30 days.22 This is a broad topic that exceeds the scope of the current review. However, a brief discussion of some available strategies is warranted to facilitate interpretation of any confounding effects these may have on hemorrhagic outcomes.
HSP for removing colonic polyps up to 1cm in size presents a slightly higher complete resection rate than a cold snare technique. However, it is associated with longer procedure time and lower intraprocedural but higher delayed bleeding rate, especially in patients taking anticoagulants.25,26 Indeed, CSP has been shown in randomized trials to yield a lower delayed bleeding rate than conventional polypectomy, despite continuation of anticoagulants.21,27,28 This difference has been linked to fewer injured arteries in the submucosal layer with the cold snare technique,27 and is especially pertinent because delayed bleeding often occurs once antithrombotics have been restarted.22 Additional endoscopic techniques that have resulted in decreased rates of delayed postprocedural bleeding include prophylactic clipping of large endoscopic mucosal resection (EMR) defects in the colon (especially on the right side)29 as well as therapeutic and preventive application of a self‑assembling peptide that acts as a hemostatic agent, protecting from recurrent postprocedural bleeding following EMR and ESD.30 A limitation of these meta‑analyses is the low prevalence of antithrombotic use in the study populations. Finally, in a small prospective study of 20 patients receiving antithrombotic therapy, endoscopic hand suturing appeared to be effective in the prevention of postgastric ESD bleeding in high‑risk patients.31
Postprocedural bleeding
Recent studies have provided valuable updated insights into the outcomes associated with different anticoagulation management strategies in various procedural contexts. The following sections present findings from retrospective analyses, prospective cohorts, and meta‑analyses highlighting key considerations for clinical practice in managing anticoagulated patients undergoing GI interventions. We have stratified the studies according to types of interventions. We have focused the discussion principally on delayed bleeding, as immediate intraprocedural bleeding is usually successfully managed at the time of the index procedure and has been reported in a very inconsistent fashion.
Reports including a mix of different endoscopic procedural risks
A prospective cohort of 6716 patients undergoing low‑risk procedures (gastric or colonic biopsies and / or CSP of polyps ≤1cm) demonstrated that the 2‑week risk of delayed bleeding was low despite continuation of antithrombotic therapy.32 There were 3 cases of delayed bleeding (0.51%) among 594 patients entering the study on an antithrombotic. Immediate bleeding was more common than delayed bleeding, noted in 7 cases. No bleeds were observed in the patients on antithrombotics undergoing gastroscopy.
A large cohort of 6765 outpatients undergoing procedures associated with various risks of delayed bleeding revealed no significant differences in postprocedural bleeding rates between the DOAC (n = 1587) and warfarin (n = 5178) groups.33
In a retrospective analysis of 1602 anticoagulated patients (including 598 on a DOAC) undergoing high- (46.6%, most commonly HSP [41.8%]) and low‑risk GI procedures, mean DOAC withholding times pre- and postprocedure were 50.1 and 25.5 hours, respectively.19 Similar incidences of 30‑day endoscopic‑related GI bleeding were noted (VKA, 6.2% vs DOAC, 6.7%), with bridging performed during high‑risk procedures in 91.9% of VKA and 17.5% of DOAC patients. No significant differences in bleeding were noted following high‑risk procedures (VKA, 11% vs DOAC, 12.6%). Among the patients undergoing high‑risk procedures (n = 747), delayed anticoagulation resumption (<24 vs >24 hours) did not reduce bleeding rates.
A network meta‑analysis of 8 cohort studies of patients undergoing endoscopic procedures associated with disparate bleeding risks (870 on DOACs and 1176 on warfarin) showed no significant differences between the groups. However, there was a strong trend toward more frequent post–endoscopic resection delayed bleeding in patients on VKAs, as compared with those on DOACs (OR, 1.29; 95% CI, 0.99–1.69).34 The rank probabilities for the types of DOACs demonstrated that the safest drug was dabigatran.
Interestingly, a recent larger meta‑analysis of 30 studies (only 1 RCT) (DOAC, n = 5786; warfarin, n = 14 293) noted lower overall bleeding rates for DOACs (across‑group ranges, 0.63%–28.6%; OR, 0.87; 95% CI, 0.68–0.91) than for warfarin following endoscopic resection (ESD, EMR, HSP, or CSP).35 These results were robust across multiple subgroup analyses and after adjustment for possible confounding variables in meta‑regression.
These studies grouping different procedural risk interventions suggest that DOACs may be associated with less frequent postprocedural delayed bleeding than warfarin.
Biopsies
In a 4:1 propensity‑matched retrospective analysis of 13 393 Japanese patients undergoing GI endoscopic biopsies (excluding bilio‑pancreatic procedures), no significant difference was noted with respect to postprocedural hemorrhage among patients on DOACs (none of whom underwent DOAC interruption), as compared with controls not receiving DOACs; however, the sample size does not exclude a small increase in risk (OR, 1.52; 95% CI, 0.96–2.41).18 Although outcome definitions were unclear, this suggests that uninterrupted DOAC therapy may not substantially increase the risk of bleeding in low‑risk procedures, and is compatible with current guideline recommendations.
Polypectomy and endoscopic mucosal resection
A study by Takeuchi et al28 was published before the time frame outlined in our search inclusion criteria; however, due to its significance as the only contemporary RCT published on the topic, we decided to include it in this review. Of note, we only present the study data related to patients who continued DOACs periprocedurally. The authors compared outcomes between continuous administration of anticoagulants with CSP (CA + CSP) and periprocedural heparin bridging with HSP (HB + HSP) following removal of subcentimeter colorectal polyps. In the CA + CSP group, the patients on a DOAC continued their usual anticoagulant therapy before and after polypectomy. The procedure for patients receiving DOACs in this group was scheduled after 3:00 PM to avoid peak DOAC levels 2 to 6 hours after oral administration. Among the 55 DOAC‑treated patients in the CA + CSP group, 4 (7.3% [95% CI, 0.4%–14.1%]) experienced a major bleed; 2 of them were on rivaroxaban. No TE events occurred. In that trial, most cases of postprocedural bleeding in the CA + CSP group in the patients receiving DOACs occurred 1 day after polypectomy, suggesting that resuming DOAC therapy the next day was too soon. Therefore, a 1‑day suspension of DOAC therapy after polypectomy was considered safer, in keeping with the PAUSE‑GI suggestions.22
In a retrospective study of 154 patients undergoing polypectomy, 3 out of 149 participants (2.01%) who temporarily stopped DOAC therapy experienced bleeding (OR, 6.12; 95% CI, 1.24–24.1) within 30 days.17 None of the 5 patients who continued DOACs experienced bleeding, but any definitive conclusions are limited by the small sample size of this study.
A prospective observational study that compared continued DOAC therapy (n = 204) vs same‑day interruption (n = 264) with regard to the frequency of PPB following low‑risk polypectomy (polyp size <1cm) showed that immediate PPB was significantly more frequent in the DOAC continued group than in the patients who withheld DOACs on the day of the procedure (25.5% [95% CI, 15.1%–39.6%] vs 6.1% [95% CI, 1.9%–15%]; P <0.008).23 The patients who continued DOAC therapy more often required hemostatic clip placement (31.9% vs 9.1%; P <0.005). Delayed bleeding occurred significantly more frequently in the DOAC continued group (8.5% [95% CI, 2.8%–20.5%] vs 0% [95% CI, 0%–6.6%]; P <0.001). Thus, the authors recommended a protocol of withholding DOACs on the day of colonoscopy in routine clinical practice.
Kim et al36 retrospectively analyzed patients undergoing CSP, EMR, or ESD, including 131 individuals on DOACs and 270 patients on clopidogrel. DOACs were discontinued a mean (SD) of 2.8 (1.7) days before and restarted 1.6 (2.9) days after polypectomy. According to the per‑patient analysis, the delayed PPB rate was 3.1% (95% CI, 0.13%–6.07%) in the DOAC group and 3% (95% CI, 0.97%–5.3%) in the clopidogrel group. DOACs did not increase the risk of delayed PPB as compared with clopidogrel (OR, 0.93; 95% CI, 0.44–1.98).
Three studies have more specifically commented on differences between DOAC molecules. A retrospective cohort study analyzed 242 patients undergoing a 1‑day interruption DOAC protocol, 113 patients on continuous warfarin, and 5062 on no anticoagulants, undergoing EMR, CSP, or HSP.37 Antiplatelet co‑administration in the anticoagulated patients was common (25%). Postprocedural bleeding at 30 days was more frequent in the anticoagulated patients (DOAC, 8.7%; warfarin, 8.%; nonanticoagulated, 1.2%), more so in the patients undergoing removal of more than 3 polyps. The patients taking rivaroxaban had more bleeds than those on edoxaban (14.8% [9/61] vs 1.8% [1/56], respectively; P <0.05).
Lau et al38 performed a regional retrospective propensity‑matched cohort study assessing 3887 patients receiving an anticoagulant who underwent colonoscopy or sigmoidoscopy with polypectomy. Overall, apixaban use was associated with a lower risk of TE and PPB than the use of warfarin and other DOACs. In a subgroup analysis, apixaban use was associated with a lower PPB risk in patients aged 70 years or older and those with right‑sided colonic polyps.
In a cohort of 1546 patients on DOACs, propensity‑matched in a 1:1 ratio with patients on a VKA, the 30‑day PPB rate was greater in the DOAC group (hazard ratio [HR], 1.97; 95% CI, 1.16–3.33).39 The highest risk of DOAC‑related PPB was noted with rivaroxaban. However, no differences were noted in subgroup analysis that assessed bleeding requiring blood transfusions, which suggests that DOAC use only increased the risk for minor GIB after polypectomy. The hazard risk of PPB in patients treated with DOACs increased when the anticoagulant therapy was combined with antiplatelet medication use.
Two recent meta‑analyses have summarized the literature on bleeding risks following colonic polypectomy in DOAC patients. The first one included 12 studies involving 621 279 participants undergoing CSP or HSP, and showed a higher risk of PPB within 4 weeks among the patients using DOACs than among those without anticoagulation (OR, 6.17; 95% CI, 3.08–12.4).40 A similar result occurred when DOACs were stopped 24 hours before polypectomy (OR, 8.66; 95% CI, 4.59–16.3). The authors suggest these findings provide support for the European Society of Gastrointestinal Endoscopy (ESGE) guidelines14 stating that DOACs should be stopped 48 hours ahead of polypectomy. In that study, a higher PPB risk was detected in the DOAC group than in the warfarin group (9.2% vs 7.2%; P = 0.572). Interestingly, dabigatran showed a lower PPB rate than warfarin (OR, 0.582; 95% CI, 0.34–0.994).
A second meta‑analysis of 17 studies (5 RCTs), assessing principally the removal of polyps up to 1 cm in size in patients undergoing CSP and treated or not treated with periprocedural antithrombotic agents, yielded pooled rates of delayed and immediate bleeding of 1.6% and 10.5%, respectively.21 Both immediate (OR, 5.85; 95% CI, 3.84–8.89) and delayed bleeding (OR, 4.02; 95% CI, 1.98–8.17) were significantly higher in the patients using periprocedural antithrombotic agents than in the nonusers. Although both antiplatelet agents and anticoagulants increased the risk of delayed bleeding, the risks associated with the use of DOACs (2.5%) or multiple agents (3.9%) were particularly high. As compared with their counterparts, patients with diminutive polyps and uncomplicated lesions not requiring hemoclipping had lower risks of delayed bleeding (pooled estimates of 0.4% and 0.18%, respectively).
In summary, DOACs should be at least withheld on the day of polypectomy / EMR, with an increased risk noted among patients on concurrent clopidogrel. DOACs as a group appear to cause more delayed bleeding than VKAs, except for dabigatran, which may be associated with a lower risk. Rivaroxaban may cause more bleeding in this context than other DOACs.
Endoscopic ultrasound–guided tissue acquisition
We could not find any contemporary articles addressing periprocedural risks associated with endoscopic ultrasound (EUS)-guided tissue acquisition among patients on DOACs that fulfilled the search inclusion criteria for this review.
Endoscopic ultrasound–guided biliary drainage
The only recent study assessing intra- or postprocedural bleeding following EUS‑guided biliary drainage included 154 controls and 41 patients on antithrombotics, with only 8 patients on a DOAC (stopped for 2 days and restarted the day following the procedure, or uninterrupted).41 None of the DOAC patients experienced bleeding. Overall, use of an antithrombotic was not a significant risk factor for bleeding (OR, 2.96; 95% CI, 0.56–14) in contrast to a longer procedure time (>20 minutes). However, the small sample size of patients using DOACs limits any robust conclusions.
Endoscopic retrograde cholangiopancreatography
A study by Muro et al42 investigated the incidence of immediate and delayed postsphincterotomy bleeding in patients treated with continuous DOAC therapy (n = 31; 4 also on antiplatelets) or HBT (n = 31). The total rate of bleeding was lower in the patients who continued DOACs than in the HBT group (0% vs 12.9%; P = 0.016).
Masuda et al43 retrospectively analyzed 524 patients who underwent a sphincterotomy. Forty‑two were on a DOAC (12 also taking antiplatelet agents), while 482 were on no antithrombotic. The DOAC was interrupted for up to 1 day in 17 patients (40%) and for more than 1 day in 25 patients (60%). HBT was used in 12 out of 42 participants (29%). Bleeding occurred in 6 patients (14%; immediate in 2 and delayed in 4). In the patients who interrupted DOACs for up to 1 day, bleeding occurred in 5 cases. Multivariable analysis showed that bleeding was more frequent in the patients on a DOAC (OR, 3.95; 95% CI, 1.37–11.4), those with a low platelet count (OR, 6.74; 95% CI, 2.1–21.6), and patients over 80 years old (OR, 3.36; 1.17–9.65). Overall, these data support society recommendations of stopping a DOAC at least 2 days before endoscopic sphincterotomy, which should be considered a high‑risk procedure12-14 (Table 1).
Percutaneous endoscopic gastrostomy
In a cohort of 33 patients on DOACs stopped for 3 days before percutaneous endoscopic gastrostomy (PEG), 3 patients (9.09%) bled.44 The bleeding rate did not differ significantly when DOACs were compared with other antithrombotic drugs. All patients who experienced bleeding were controlled with adrenaline injections. None of them required transfusions, and no decrease in hemoglobin level was observed in any case.
In another study of 24 patients on uninterrupted DOAC monotherapy undergoing PEG, no patient developed postprocedural bleeding.45 The small number of patients in these studies limits reliable conclusions.
Endoscopic submucosal dissection
The following sections summarize findings from several key studies that explore the incidence of postprocedural bleeding in patients undergoing esophageal (including peroral endoscopic myotomy [POEM]), gastric, and colonic ESD. These procedures are considered high‑risk by the CAG‑ACG and the British Society of Gastroenterology – ESGE guidelines.12,14 Interestingly, the Asian Pacific Association of Gastroenterology – Asian Pacific Society for Digestive Endoscopy created a separate “ultrahigh‑risk” category to classify these procedures13 (Table 1).
In a study assessing risk factors for delayed bleeding among 109 patients on a DOAC undergoing ESD resection of lesions in the esophagus, stomach, or colon, the incidence of delayed bleeding was 12.8% (95% CI, 7.2%–20.6%). In the multivariable analysis, risk factors for post‑ESD bleeding were older age (OR, 1.19; 95% CI, 1.02–1.39) and high anticoagulant ability analyzed by the factor Xa activity at trough and time to peak drug concentration (OR, 6.056; 95% CI, 1.09–33.5).46
Most studies have assessed organ‑specific ESD procedures, and these are listed below.
Esophagus
Endoscopic resection
In a cohort of 16 DOAC‑treated patients undergoing esophageal ESD (n = 14) and EMR (n = 2), DOACs were stopped on the day of the procedure and restarted the next day.47 Delayed bleeding was noted in 13% (95% CI, 1.6%–38%) of the patients, a significantly higher rate than that in the group not taking antithrombotic drugs (0.3% [95% CI, 0.1%–1%]; P = 0.003).
Peroral endoscopic myotomy
In an international study that included 19 patients on a DOAC undergoing POEM (HBT in 4 cases, with anticoagulation stopped 12–48 hours prior to the procedure in all), 1 patient (5.3% [95% CI, 0%–16.1%]) developed bleeding 12 days later but required no hemostatic therapy.48
Gastric
Ono et al49 compared 23 patients on factor Xa inhibitors undergoing gastric ESD and 156 patients on no antithrombotic. The patients did not take the DOAC on the morning of the procedure, and the drug was restarted the next day (approximate mean total interruption time, 36 hours). Some patients received HBT post‑ESD. A total of 7 patients (30.4%; OR, 5.7; 95% CI, 1.4–23.7, as compared with controls) experienced bleeding within 30 days (median time to bleed, 5 days; 2 patients on HBT and 1 receiving clopidogrel). The rate of inhibited thrombin generation, a measure of anticoagulation activity in these patients, was greater in those who bled (18.6% vs 3.8%; P = 0.046).
In a recent meta‑analysis of 7 studies (DOAC, n = 405; warfarin, n = 491; controls, n = 15 206) that investigated bleeding associated with DOAC use after gastric ESD, delayed bleeding was more frequent among the DOAC users than among the patients on no antithrombotic therapy (17% vs 3.4%; OR, 5.72; 95% CI, 4.33–7.54) but comparable to that observed in the patients on warfarin (17% vs 20%; OR, 0.83; 95% CI, 0.59–1.18).50
Two research groups have attempted to identify scoring models (Safe ESD Management Using the Risk Analysis of Post‑Bleeding in Patients with Antithrombotic Therapy [SAMURAI] and Bleeding after ESD Trend from Japan [BEST‑J]) that predict bleeding after a gastric ESD procedure.51,52 The models exhibited modest‑good prediction accuracy (C statistics of 0.77 and 0.7, respectively). DOAC use was a risk factor identified in both models (ORs of 8.16–10.45).
Colonic
A retrospective Japanese single‑center study assessed 412 patients (286 off antithrombotics, 26 on warfarin, and 25 on a DOAC) undergoing colorectal ESD.53 The DOAC patients either received HBT or followed a 2‑day interruption protocol (DOAC stopped 1 day pre- and resumed 1 day post‑ESD). Delayed bleeding was noted in 16% of the DOAC patients (1 with HBT), which, due to the small sample size, translated into arithmetically but not significantly greater risk than that noted in patients on no antithrombotics (6.6%) or warfarin (7.7%). The delayed bleeding rate among the patients following the DOAC interruption protocol was 14.3%, occurring within 4 days. No transfusions were required in any patient.
A multicenter prospective interventional uncontrolled study assessed postprocedural bleeding in patients undergoing prophylactic clip closure after colorectal ESD in patients on anticoagulant therapy.54 Only 1 of 33 DOAC patients received HBT, with all others following solely a DOAC interruption protocol on the day of ESD (it is unclear if any participants were also on antiplatelet agents). Bleeding occurred in 2 patients (5.9% [95% CI, 1.1%–17.4%]), with no cases of major hemorrhage.
Yoshida et al20 analyzed cases of delayed bleeding after colorectal ESD in patients on DOACs or warfarin. The former were bridged with heparin until 2017, after which time the DOAC was withheld only on the day of the procedure and resumed 1 day after. All patients were hospitalized for 3 days following the procedure. Delayed bleeding rates did not differ between the DOAC (n = 1019) and warfarin (n = 459) users (9.32% vs 11.8%; P >0.05), and bleeding was more common among the DOAC and warfarin patients receiving HBT (15.3% vs 8.44%; P <0.001). Delayed bleeding was significantly more frequent among dabigatran users than among patients treated with apixaban, edoxaban, and rivaroxaban (OR, 0.5; 95% CI, 0.26–0.94; OR, 0.37; 95% CI, 0.2–0.7; and OR, 0.34; 95% CI, 0.18–0.65, respectively). Only rivaroxaban use was associated with significantly lower delayed bleeding than warfarin use (OR, 0.58; 95% CI, 0.35–0.96). In a multivariable analysis, HBT (OR, 2.18; 95% CI, 1.27–3.73), rectal location of the lesions (OR, 2.01; 95% CI, 1.28–3.16), and procedure time greater than or equal to 55 minutes (OR, 2.43; 95% CI, 1.49–3.95) were significant risk factors for delayed bleeding in the DOAC group.
A provocative retrospective, 2‑center Japanese study investigated continuous use of antithrombotic medications during the periprocedural period in patients undergoing colorectal ESD.55 The authors’ rationale was that many patients may not require intervention for delayed bleeding even when it does occur. This propensity score matched study analyzed 148 patients (74 treated and 74 not treated with antithrombotics). All participants were admitted for the procedure and discharged on post‑ESD day 6 or 7. Delayed bleeding within 30 days was noted in 7 of 22 DOAC patients (32%). All of them had successful hemostasis following the bleeding episode or required no intervention. Low‑dose aspirin, warfarin, or DOAC use (OR, 10.78; 95% CI, 3.32–35.05) were all independent risk factors for post‑ESD bleeding.
In summary, delayed bleeding rates following gastric ESD among patients undergoing standard DOAC management interruption protocols range from 9% to 16%, with few cases of major hemorrhage, and rise when the DOAC is not withheld. Co‑administration of antiplatelet agents increases the bleeding risk.
Double‑balloon enteroscopy
We were unable to identify any current articles on the bleeding risks associated with double‑balloon enteroscopy in patients taking DOACs that met the inclusion criteria for our review.
Guidelines and proposed algorithm
Development of standardized, evidence‑based protocols for the periprocedural management of patients receiving DOACs has posed challenges for medical societies worldwide. In the absence of high‑quality evidence, clinicians have often relied on diverging expert opinions to guide their practices. Consequently, there have been significant disparities in management algorithms over the past decade. Notably, the use of HBT, once recommended, is now widely discouraged for patients undergoing digestive endoscopy, based on 2 recent pivotal RCTs.56,57 The landmark PAUSE study,58 along with a subanalysis focused on GI endoscopy procedures,22have provided robust evidence supporting the contemporary practice of minimizing DOAC interruption. All major GI societies have adopted this approach, with slight variations in practical implementation. Table 2 summarizes the current interruption protocols proposed by major societies.12-14
Risk level | ACG‑CAG | BSG‑ESGE | APAGE‑APSDE | |||
Interruption | Resumption | Interruption | Resumption | Interruption | Resumption | |
a For patients on dabigatran with a creatinine clearance <50 ng/ml or estimated glomerular filtration rate <50 ml/min/1.73 m2
b Depends on hemorrhagic and thrombotic risk, consider extending interval for ESD
c Category created by APAGE‑APSDE
Abbreviations: see Table 1 | ||||||
Low‑risk procedure | 1 or 2a days preprocedure | Following day | Morning of the procedure | 2–3 days postprocedureb | No cessation | – |
High- / ultrahigh‑riskc procedure | 2 days preprocedure | When hemostasis is achieved | 3 or 5c days preprocedure | <3 days postprocedure OR when hemostasis is achieved | ≥2 days preprocedure | When hemostasis is achieved |
Special considerations
Although a vast majority of patients on DOACs do not require HBT, such an approach may be considered in individuals at a very high risk of a TE event. The European Society of Cardiology guidelines59 identify these patients as belonging to the following groups: 1) those with a mechanical aortic valve and any thromboembolic risk factor, 2) individuals with an old‑generation mechanical aortic valve, and 3) patients with a mechanical mitral or tricuspid valve. In addition, bridging with heparin may be considered in 1) patients taking a DOAC who have experienced a recent (<3 months) TE event (stroke, systemic embolism, or VTE); or 2) those who experienced a TE event during previous interruption of DOAC therapy. Finally, postoperative thromboprophylaxis with low‑molecular‑weight heparin should be considered in patients in whom DOAC therapy cannot be quickly restarted as planned (see the PAUSE‑GI protocol). In such patients, monitoring of anti–factor Xa activity and dose adjustment to a target level of 0.5–1 U/ml may be considered.
The periprocedural DOAC management in very elderly patients, in particular, requires pharmacovigilance and an individualized holistic approach. Octogenarians and nonagenarians are at an increased risk for both TE and bleeding adverse events due to comorbid conditions coupled with pharmacokinetic and pharmacodynamic alterations.60 These risks are further compounded by polypharmacy and a lack of specific RCTs and guidelines addressing this patient population. DOACs are preferred over VKAs in these individuals because they exhibit fewer drug–drug interactions and are less dependent on changes in body mass and renal function (except for dabigatran), as long as the creatinine clearance remains above 15 ml/min, below which they are contraindicated.60 Furthermore, DOACs are easier to comply with in the setting of cognitive impairment and have even been linked to decreased cognitive decline.60 These agents are also preferred in the context of frailty and the risk of falls. The reader is referred to an excellent recent review on the topic for a more detailed discussion of an optimal management approach.60
Future directions
The management of DOACs in the GI periprocedural setting requires further clarifications as to differences in bleeding rates associated with the use of individual DOACs and in comparison with VKAs. A better understanding of the natural history of both delayed PPB and TE events as well as further development of intraprocedural interventions are to be expected which may alter guideline recommendations. Ideally, high‑quality evidence in the form of RCT‑based findings should be generated.
Conclusions
The present study summarizes the current body of literature regarding the periprocedural management of DOACs in patients undergoing digestive endoscopy since the publication of the 2022 ACG‑CAG guidelines. We provided a detailed analysis of the TE risk, procedure‑specific bleeding risks, contemporary techniques to reduce the bleeding risk, and a summary of guidelines addressing periprocedural DOAC use, including procedure risk stratification developed by major GI societies. While there exists heterogeneity in the data, the overall trend of the current literature supports the contemporary practice of a minimal DOAC interruption.
- Joy M, Williams J, Emanuel S, et al. Trends in direct oral anticoagulant (DOAC) prescribing in English primary care (2014‑2019). Heart. 2023; 109: 195‑201. | Crossref
- Cabral KP. Pharmacology of the new target‑specific oral anticoagulants. J Thromb Thrombolysis. 2013; 36: 133‑140. | Crossref
- Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest. 2018; 154: 1121‑1201. | Crossref
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology / American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019; 140: e125‑e151. | Crossref
- Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021; 160: e545‑e608. | Crossref
ARTICLE INFORMATION