Introduction
Air pollution significantly affects the health of human populations worldwide. The negative effects of air pollutants on airway epithelium are associated with oxidative stress (OS), proinflammatory response, and impaired innate immune reactions. The concentration and composition of particulate matter (PM) vary due to many natural and anthropogenic factors, including local or regional sources, meteorological conditions, and geographic location. The potential adverse health effects of PM are related to a particle’s size and its chemical, physical, and biological properties, as well as associated organic and nonorganic load. PM is classified based on its aerodynamic diameter, with PM10 (aerodynamic diameter <10 µm), PM2.5 (aerodynamic diameter <2.5 µm), and PM1 (aerodynamic diameter <1 µm) being the most commonly monitored fractions.
The relationship between proinflammatory effects of specific PM constituents on human epithelial cells remains inadequately explained. Due to the complex structure of airway epithelium and multitude of interactions within it, exposure to PM can adversely affect tissue in various ways. For instance, air pollution impairs mucociliary clearance by disrupting the structure and function of cilia. Studies have shown that exposure to pollutants, such as nitric dioxide, cigarette smoke, and other oxidants, can result in reduction of their number, their shortening, or reduced beating frequency, even in healthy individuals.1,2 OS, accompanied by inflammation, is recognized as the primary pathway of PM‑induced toxicity and adverse health effects attributed to the presence of OS‑inducing polyaromatic hydrocarbons and transition metals.3 While antioxidants have a therapeutic potential, in vitro studies suggest that, depending on the type of a damage factor, some antioxidants can exacerbate OS, highlighting their dual role. Although it has been hypothesized that antioxidants and anti‑inflammatory agents could mitigate respiratory and cardiovascular effects of air pollution by downregulating OS and inflammation,4 official recommendations do not endorse antioxidant supplementation due to insufficient evidence of its efficacy in counteracting air pollution’s detrimental effects on respiratory health.5 Furthermore, a detailed mechanism underlying the potential protective action of antioxidants or anti‑inflammatory agents on PM‑exposed airway epithelium remains unclear. The aim of this in vitro study was to investigate the effect of 2 antioxidant agents, hyaluronic acid (HA) and docosahexaenoic acid (DHA), on the inflammatory response of nasal epithelial cells from healthy individuals following the exposure to cigarette smoke extract (CSE) or PM2.5 treatment.
Materials and methods
Epithelial cells were obtained through nasal brushing (Cytobrush Plus GT, CooperSurgical, Trumbull, Connecticut, United States) from a cohort of healthy, nonsmoking individuals (n = 10) with a negative history of chronic lung diseases, absence of respiratory symptoms, normal spirometry results, and no respiratory tract infection within 3 months prior to sample collection. The study protocol was approved by the Ethical Committee of the Medical University of Warsaw (KB/12/2023) and all participants provided informed consent. Characteristics of the study participants are presented in Supplementary material, Table S1. As previously described, the isolated cells were cultured at air‑liquid interface.6 Research cigarettes 1R6F with filter (Kentucky Tobacco Research and Development Center at the University of Kentucky) were used for CSE preparation, according to the procedure outlined in a previous publication.7 Urban PM was collected in Zabrze, Gliwice, and Żory during the heating season and provided by the Silesian University of Technology. The particles were isolated from high‑purity quartz (SiO2) microfiber filters (QM‑A, Whatman, Little Chalfont, United Kingdom), and prepared as previously described.8
The levels of all stimulators were selected based on cytotoxicity results (Supplementary material, Figure S1). Nasal epithelial cells, both untreated and treated with 100 µg/ml of PM2.5 or 5% CSE were further stimulated with 3 µM of DHA (cis‑4.7.10.13.16.19‑docosahexaenoic acid; Sigma‑Aldrich, Saint Louis, Missouri, United States) or 100 µg/ml of HA sodium salt (Sigma‑Aldrich) for 24 hours. mRNA expression levels of ALHD3A1, IL‑1β, IL‑6, IL‑8, MMP7, MMP9, MUC5AC, TGF-β, TNF-α were evaluated with quantitative polymerase chain reaction. Transepithelial electrical resistance was measured using a Millicell ERS‑2 Voltohmmeter (Merck Millipore, Burlington, Massachusetts, United States). Cytokine levels in cell supernatants were analyzed using a cytometric bead assay (Human Inflammatory Cytokine Cytometric Bead Array, Becton Dickinson, BD Biosciences, San Jose, California, United States). Detailed methodological procedures are provided in Supplementary material.
Statistical analysis
Statistical analysis was performed with GraphPad Prism (version 9.3.1; San Diego, California, United States). The Mann–Whitney test was applied for pairwise comparisons. Resulting P values were corrected with the Benjamini–Hochberg algorithm. Results are presented as median and interquartile range. Differences were considered significant at P values lower than or equal to 0.05.
Results
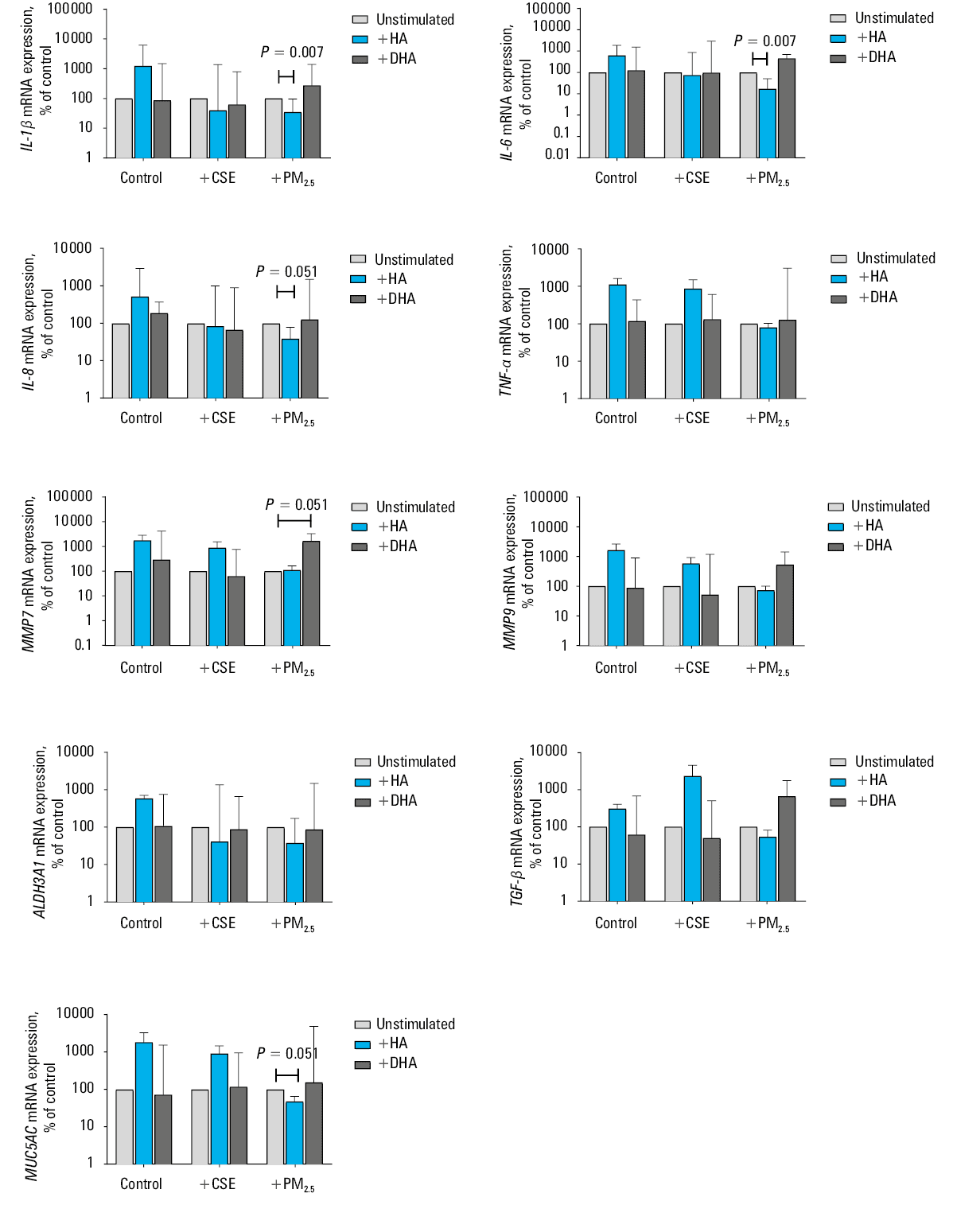
Treatment with HA or DHA did not alter mRNA expression of investigated markers in CSE- stimulated nasal epithelial cells (Figure 1). Downregulation of IL‑1β (P = 0.007), IL‑6 (P = 0.007), IL‑8 (borderline significance; P = 0.051), and MUC5AC (borderline significance; P = 0.051) was observed after HA treatment in nasal epithelial cells exposed to PM2.5 (Figure 1). DHA supplementation increased MMP7 mRNA expression (borderline significance; P = 0.051) in epithelial cells stimulated with PM2.5. No significant changes in transepithelial electrical resistance or cytokine protein level were found in the investigated groups (Supplementary material, Figures S2 and S3).
Discussion
Investigation of agents supporting the epithelial defense against air pollution is crucial. Antioxidants, which inhibit the formation of free radicals or participate in their transformation into inactive oxygen species, play an important role in counteracting the damage caused by reactive oxygen species. In this study, we evaluated the potential effect of 2 antioxidant agents in reducing the negative effect of air pollution on the respiratory tract. We report a novel finding that HA might support respiratory epithelium in antipollution defense. On the contrary, DHA did not exhibit such qualities in our evaluation.
The efficacy of antioxidant supplementation in mitigating the effects of air pollution has been explored in previous human studies. Several randomized, double‑blinded, placebo‑controlled studies showed that nutrients, such as vitamin C, vitamin E, vitamin D, and omega‑3 polyunsaturated fatty acids (n‑3 PUFAs), may exert protective effects against air pollution in healthy populations. These studies have utilized experimental designs involving administration of supplements with outcomes including assessments of lung function, bronchial airway reactivity, inflammatory response, and levels of OS biomarkers measured in various samples, such as plasma, serum, urine, sputum, and bronchoalveolar lavage fluid.9 The reported results are conflicting. As some of the studies showed negative outcomes, the protective effect of antioxidants against pathologic response to air pollution is not definitely evidenced. It has been suggested that therapy with inhaled antioxidants might be more effective than their oral administration one.10 However, it is important to acknowledge the inherent risks associated with any intervention due to very delicate balance between oxidation and antioxidation in cellular processes. Both low and high doses of antioxidants can be potentially harmful, emphasizing the need to determine optimal physiologic dosage. Antioxidants have been shown to impact various cellular responses, including oxidative, nitrosative, and dicarbonyl metabolism, as well as inflammatory pathways. Importantly, specific mechanisms underlying the potential protective action of antioxidants or anti‑inflammatory agents on airway epithelium exposed to PM are not well understood.
In this study, we evaluated the potential of DHA, an n‑3 PUFA, for supporting epithelial cells in their defense against air pollution. Previous reports have suggested that n‑3 PUFAs found in fish oil may mitigate OS induced by exposure to PM2.5 by activating endogenous antioxidants. A 4‑month supplementation of n‑3 PUFAs was found to significantly increase the activity of superoxide dismutase by 49%, elevate glutathione levels by 62%, and reduce lipoperoxidation by 72%.11 Additionally, in vitro studies demonstrated that PUFAs, including DHA, decreased mucus production in epithelial cells and improved the viscoelastic properties of mucus.11 Contrary to expectations, our study did not show any beneficial effects of DHA treatment on respiratory epithelial cells exposed to toxic substances. This suggests that PUFAs are not useful in counteracting detrimental effects of PM2.5 on the respiratory tract.
Interestingly, DHA supplementation increased MMP7 mRNA expression in epithelial cells stimulated with PM2.5. This phenomenon might be explained in several ways. The function of MMP7 is linked to many biological processes, for example, wound repair and fibrosis, inflammation, and neutrophil accumulation, but also to innate immune response. Increased MMP7 expression in epithelial cells exposed to PM2.5 after DHA treatment might suggest acceleration of inflammatory response by PUFA in this model. MMP7 participates in the shedding of syndecans from cell surface and regulates the chemokine (eg, IL‑8) influx leading to, for instance, local neutrophil accumulation.12 On the other hand, MMP7 modulates innate immunity by activating antimicrobial peptides (α-defensin) after lipopolysaccharides stimulation.13 As the levels of antimicrobial peptides were shown to change as part of defense mechanism against pollution,14 the observed upregulation of MMP7 expression in the epithelium treated with PM2.5 might be linked to antimicrobial proprieties of DHA. Of note, we did not measure the tissue inhibitor of metalloproteinases 2 expression, and without monitoring a balance between protease / antiprotease expression and activity, definitive conclusions cannot be drawn. Verification of these hypotheses needs in vitro human studies.
In contrast to DHA, HA, another agent with antioxidant capacity used in this study, seemed to support epithelial cells in their response after stimulation with PM2.5. In addition to its antioxidant properties, HA plays a crucial role in regulating fluid balance in the lung interstitium due to its anti‑inflammatory and water‑binding capacities. Administration of HA via aerosol or tracheal instillation has been shown to reduce inflammation, thereby protecting the airways from hyper‑reactivity and remodeling of the bronchial parenchyma. OS is associated with hyaluronan fragmentation, mediated by induction of hyaluronidase 2, hyaluronan‑degrading enzyme in human bronchial epithelial cells.15 Our study results indicate a significant anti‑inflammatory effect of HA in nasal epithelial cells after treatment with PM2.5. HA reduced mRNA expression of key inflammatory cytokines (IL‑1β, IL‑6, IL‑8) as well as MUC5AC in epithelial cells folllowing stimulation with air pollutants. Notably, this effect was found in cultures treated with PM2.5 only, and was not observed in CSE‑treated cells, suggesting a specific targeting of HA in counteracting the harmful effects of air pollution on the respiratory system. We suggest that this observation might be linked to Toll‑like receptor 4 (TLR4) signaling. Many authors reported that the immune response of epithelial cells on both airborne pollutants and cigarette smoking is mediated by TLR4.16 TLRs are immune sensors that recognize pathogen‑associated molecular patterns of microorganisms and other toxicant stimuli. It has been reported that air pollution increases MUC5AC and MUC5B expression via the TLR4‑mediated activation of extracelullar signal‑regulated kinase 1 and 2, p38 mitogen‑activated protein kinase, and nuclear factor kappa‑light‑chain‑enhancer of activated B cells signaling pathways in human airway epithelial cells.16 PM2.5 suspension contains particles larger than CSE, often undissolved in water, with attached biological components, such as bacterial endotoxins; for this reason, lipopolysaccharides might be a more potent TLR4 activator. It is well documented that HA is a ligand for TLR4 and can signal through TLR4, in opposite to DHA, for which such effect was not found.17 We suggest that via binding to TLR4 in epithelial cells treated with PM2.5, HA decreases the pool of TLR4 and downregulates the inflammatory response mediated by this receptor.
Several studies have shown the effectiveness and safety of HA administered intranasally or by inhalation in upper or lower airway disease. The protective effect of HA in the airways is linked to high‑molecular‑weight HA. The delivery of aerosolized exogenous high‑molecular‑weight HA had anti‑inflammatory effect, protecting against bronchial hyperreactivity, remodeling, and disrupting the biofilm associated with chronic infections.18 Indeed, the most common way of administration was nebulization with 0.3% HA sodium salt. Treatment with inhaled HA decreased the duration of acute respiratory failure during exacerbation of chronic obstructive pulmonary disease and was associated with improved lung function.19 On the other hand, when HA was delivered using a dry powder inhaler, it was dominantly deposited in the upper respiratory tract, where it exerted a protective effect on the respiratory mucosa.20 The results of our study suggest a possible beneficial action of HA in anti‑pollution defense of airway epithelium when delivered in lower doses (0.01%), preferably as an aerosol. However, this is a preliminary in vitro study—evaluation of effective HA airway distribution as a potent antipollutant agent needs to be further investigated.
Limitations
This study utilized nasal epithelial cells as functional and easily obtainable surrogate for epithelial cells from the lower respiratory tract. However, for a more comprehensive characterization of the observed results, further evaluation with bronchial epithelial cells, preferably sourced from both healthy individuals and those with respiratory diseases, such as asthma and chronic obstructive pulmonary disease, should be conducted.
Conclusions
The observed anti‑inflammatory action of HA on respiratory epithelial cells suggests its potential utility in locally preventing the detrimental effects of air pollution.
- Smallman LA, Gregory J. Ultrastructural abnormalities of cilia in the human respiratory tract. Human Pathology. 1986; 17: 848‑855. | Crossref
- Helleday R, Huberman D, Blomberg A, et al. Nitrogen dioxide exposure impairs the frequency of the mucociliary activity in healthy subjects. Eur Respir J. 1995; 8: 1664‑1668. | Crossref
- Hirota JA, Hirota SA, Warner SM, et al. The airway epithelium nucleotide‑binding domain and leucine‑rich repeat protein 3 inflammasome is activated by urban particulate matter. J Allergy Clin Immunol. 2012; 129: 1116‑1125.e6. | Crossref
- Romieu I, Castro‑Giner F, Kunzli N, Sunyer J. Air pollution, oxidative stress and dietary supplementation: a review. Eur Respir J. 2008; 31: 179‑197. | Crossref
- Carlsten C, Salvi S, Wong GWK, Chung KF. Personal strategies to minimise effects of air pollution on respiratory health: advice for providers, patients and the public. Eur Respir J. 2020; 55: 1902056. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION