Percutaneous embolization of pulmonary arteriovenous malformation for the treatment of chronic hypoxemia in a patient with Osler–Weber–Rendu syndrome
1,3



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Percutaneous embolization of pulmonary arteriovenous malformation for the treatment of chronic hypoxemia in a patient with Osler–Weber–Rendu syndrome
Pulmonary arteriovenous malformations (PAVMs) or fistulae are abnormal connections between the pulmonary artery and pulmonary vein, bypassing normal capillary circulation and resulting in a right‑to‑left shunt, paradoxical embolization, hemoptysis, or even rupture with massive pulmonary bleeding.1 PAVMs commonly occur in individuals with hereditary hemorrhagic telangiectasia (HHT), also known as Osler–Weber–Rendu syndrome.2
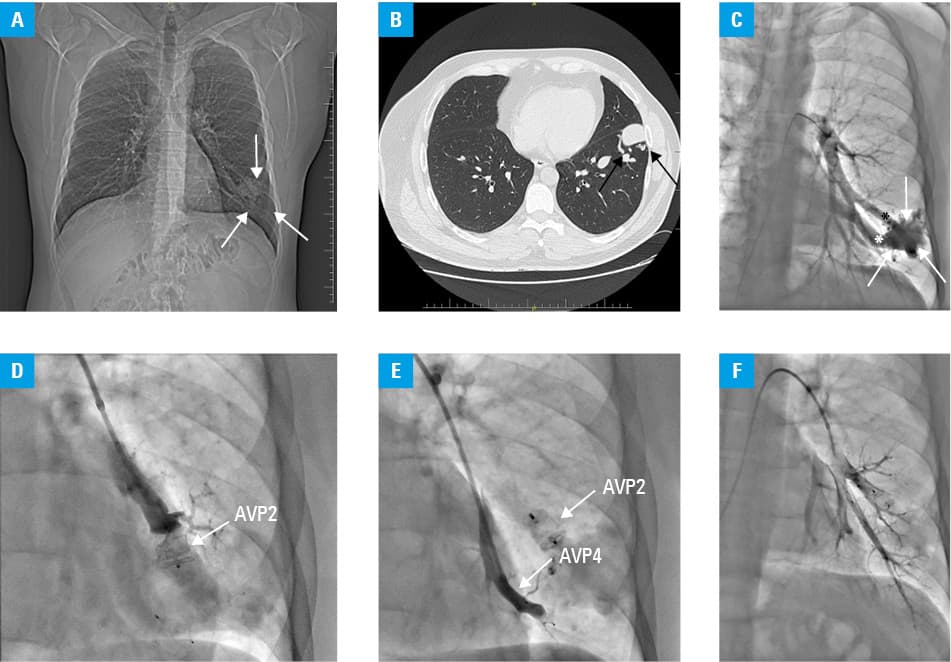
We report a case of a 37‑year‑old man with HHT diagnosed based on the consensus criteria,3 and a positive family history of this condition, who was referred to our center due to chronic hypoxemia and exercise intolerance. Repeated chest X‑rays have been showing a solitary nodule, 4 cm in size, in the left lower lobe (Figure 1A) since the patient was 19 years old. Computed tomography showed a bulbous, sac‑like structure located in the left anterior basal segment (Figure 1B). On admission, the patient was hemodynamically stable with oxygen saturation (SpO2) of 85%. He presented with characteristic telangiectasia on the lips and oral mucosa, and complained of recurrent epistaxis. Laboratory test results showed polycythemia with a hemoglobin level of 18.5 g/dl (reference range, 14–18 g/dl). Echocardiography was unremarkable. He walked 620 meters in the 6‑minute walking test (6MWT), with substantial desaturation to 78%. A neurological consultation was requested due to an episode of transient diplopia that occurred a few months before the admission. The consulting neurologist emphasized the risk of paradoxical embolization, which was further substantiated by small cerebrovascular lesions seen on the brain magnetic resonance imaging (MRI). Prior to angiography, right heart catheterization was conducted and no features of pulmonary hypertension were detected. Conventional pulmonary angiography confirmed a solitary PAVM with 2 feeding pulmonary arteries filling it in with the contrast medium and rapidly emptying it via draining veins into the left pulmonary vein (Figure 1C). Decision on PAVM embolization was made considering the feeding arteries’ diameter of 2 mm or less, chronic hypoxemia, and lesions on brain MRI. Using the right femoral access, 2 vascular occluders, Amplatzer Vascular Plug 2 (AVP2) (Abbott, Green Oaks, Illinois, United States) sized 12 mm × 7 mm and AVP4 sized 8 mm × 13.5 mm, were introduced and implanted directly into both feeding arteries, successfully closing the malformation (Figure 1D–1F). No complications occurred. Immediately after the procedure, SpO2 improved to 96%–99%. Next day, the patient walked 680 m in the 6MWT. No desaturation was observed. In the 30‑day follow‑up, the patient reported improvement in exercise tolerance, no hypoxemia, reduction of mucosal telangiectasia, and lower frequency of epistaxis.
Although uncommon in the general population, PAVMs are an important consideration in the differential diagnosis of hypoxemia, pulmonary nodules, or hemoptysis, and should also be considered in patients presenting with paradoxical embolization, including cryptogenic stroke, as minimally invasive therapies may be feasible for their treatment.
- Waligóra M, Stępniewski J, Kopeć G. Severe refractory arterial blood desaturation in the course of acute pulmonary embolism successfully reversed with catheter‑directed therapy. Pol Arch Intern Med. 2023; 133: 16537. | Crossref
- Nakayama M, Nawa T, Chonan T, et al. Prevalence of pulmonary arteriovenous malformations as estimated by low‑dose thoracic CT screening. Intern Med. 2012; 51: 1677‑1681. | Crossref
- Faughnan ME, Mager JJ, Hetts SW, et al. Second international guidelines for the diagnosis and management of hereditary hemorrhagic telangiectasia. Ann Intern Med. 2020; 173: 989‑1001.
ARTICLE INFORMATION