The role of multimodal imaging in diffuse large B-cell lymphoma with primary cardiac involvement

 CC BY 4.0
CC BY 4.0
The role of multimodal imaging in diffuse large B-cell lymphoma with primary cardiac involvement
Diffuse large B‑cell lymphoma (DLBCL), the most common type of non‑Hodgkin lymphoma, often involves lymph nodes. Cardiac manifestation, particularly primary cardiac lymphoma, is extremely rare and might lead to heart failure. Only a few cases have been reported in the literature.1-4 Although the prognosis is unfavorable, multiple imaging methods might facilitate and accelerate the diagnostic process.
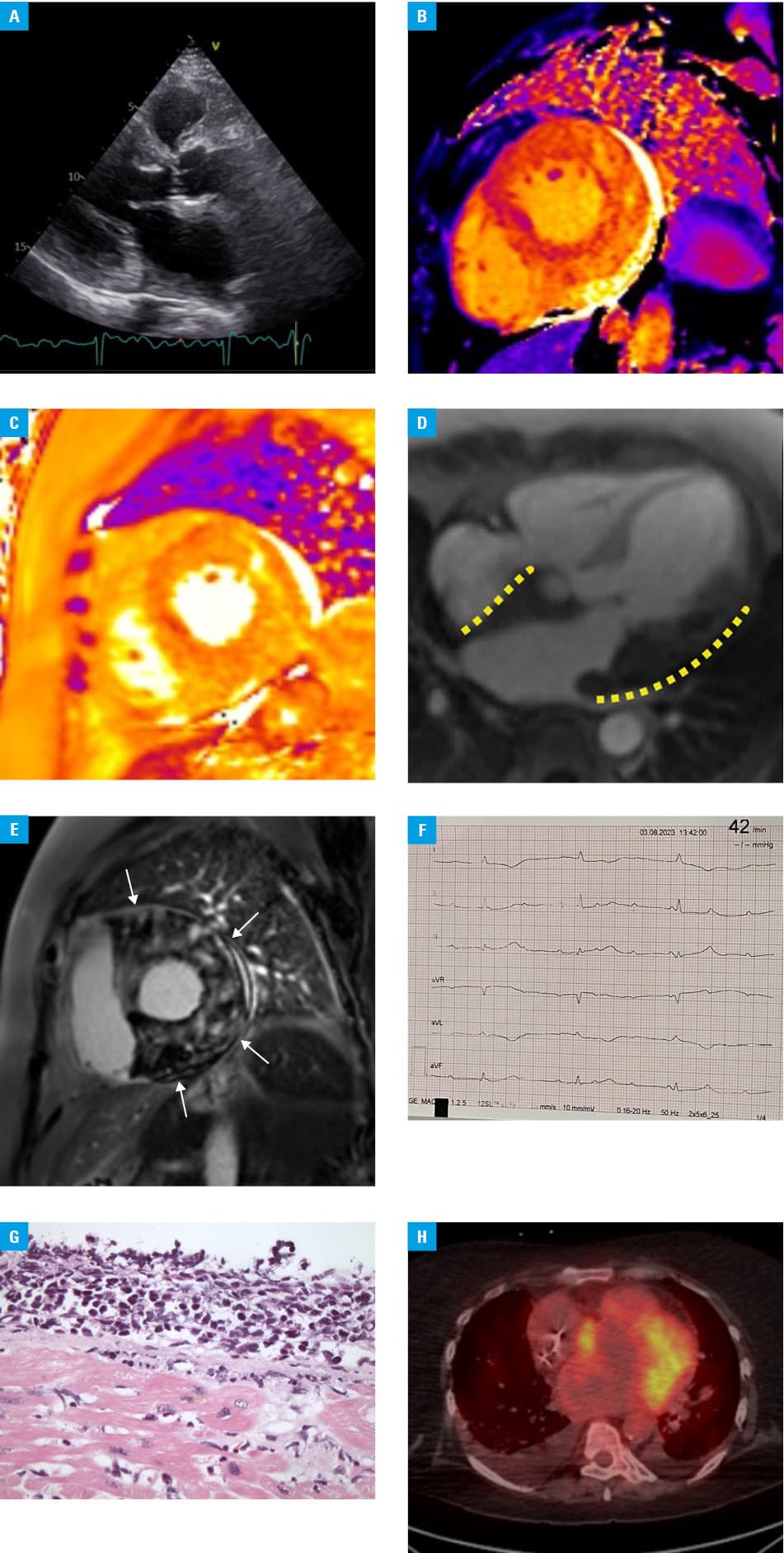
A 72‑year‑old woman with a suspicion of myocardial tumor was transferred to a tertiary cardiology center from a regional hospital, where she was treated for cardiac decompensation. The patient had type 2 diabetes mellitus, paroxysmal atrial fibrillation, arterial hypertension, and dermatomyositis treated with prednisone, but he did not attend appointments at a rheumatology clinic. Transthoracic echocardiography showed nondilated left ventricle (LV) with asymmetric hypertrophy (Figure 1A), regional wall motion abnormalities, mildly reduced ejection fraction (47%), and moderate mitral valve regurgitation. Laboratory workup showed increased levels of troponin I (277 pg/ml; reference range [RR], 0–16 pg/ml), N‑terminal pro‑B‑type natriuretic peptide (24 768 pg/ml; RR, 0–125 pg/ml), and inflammatory markers: C‑reactive protein (165 mg/l; RR, 0–5 mg/l) and procalcitonin (0.96 ng/ml; RR, 0–0.05 ng/ml). Cardiac magnetic resonance (CMR) imaging, including T1- and T2‑mapping, rest perfusion sequence, and late gadolinium enhancement sequence (Figure 1B–1E) raised a suspicion of a malignant tumor situated in the LV myocardium, part of the right ventricle, left atrial wall, and the ascending aorta. On the second day of hospitalization, endomyocardial biopsy of the involved LV regions was performed. A few hours after the procedure, the patient developed a third‑degree atrioventricular block (Figure 1F) and urgent temporary cardiac pacing was implanted, followed by permanent pacemaker implantation on the fourth day of hospitalization. Based on the histopathology report, DLBCL, not otherwise specified, nongerminal center B‑cell phenotype was identified (Figure 1G). Positron emission tomography (PET) showed increased metabolic activity in the cardiac muscle (Figure 1H), bone marrow of the sternum, and left femur, indicating an active malignancy and bone metastases.
The patient’s condition stabilized following treatment and she was transferred to a hematology department. Intravenous immunochemotherapy was implemented, including the R‑COMP regimen, consisting of rituximab, cyclophosphamide, vincristine, prednisone, and liposomal doxorubicin administered at standard therapeutic doses. Liposomal doxorubicin was chosen due to its favorable toxicity profile and better cardiac safety.5,6
During follow‑up, the patient required inotropic support due to progression of the underlying disease with further myocardial involvement. Therapeutic options were exhausted and the patient died 6 weeks after admission to our hospital.
Patients on long‑term immunosuppressive treatment should be systematically evaluated for potential proliferative processes. If any cardiac symptoms are present, echocardiographic assessment and cardiac imaging using advanced techniques, such as CMR or PET, should be performed as soon as possible. If a cardiac tumor is suspected, early endomyocardial biopsy may be necessary to establish a proper diagnosis, allowing dedicated treatment. This case emphasizes that the use of multimodal imaging allows for early identification of a problem, differential diagnosis, and proper staging of DLBCL.
- Qiang Y, Zeng K, Zhang B, et al. Atypical location of primary cardiac lymphoma in the left heart with atypical clinical presentation: a case report and literature review. Front Surg. 2023, 9: 1036519. | Crossref
- Csizmar CM, Sachs Z, Cayci Z, et al. Primary cardiac lymphoma: three case reports and a review of the literature. Open J Blood Dis. 2021; 11: 120‑132. | Crossref
- Tanking C, Ratanapo S. Diagnostic challenge in primary cardiac lymphoma: a case report. Eur Heart J Case Rep. 2020; 4: 1‑5. | Crossref
- Yousif P, Kotecha A, Thakur A, et al. A rare case of diffuse large B cell lymphoma presenting as a cardiac mass. Am J Case Rep. 2019; 20: 1821‑1825. | Crossref
- Rafiyath SM, Rasul M, Lee B, et al. Comparison of safety and toxicity of liposomal doxorubicin vs. conventional anthracyclines: a meta‑analysis. Exp Hematol Oncol. 2012; 1: 10. | Crossref
ARTICLE INFORMATION