Factor XI inhibition in cardiovascular disease
Key words: cardiovascular diseases, factor XI, hemorrhage, thrombosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Factor XI inhibition in cardiovascular disease
Cardiovascular disease remains the leading global cause of mortality, requiring effective antithrombotic strategies to prevent thromboembolic events. Currently available therapies are effective but have inherent bleeding risks which may limit or preclude their use, particularly in patients at the highest risk of bleeding. Factor XI (FXI) inhibitors are a promising new class of anticoagulants which may mitigate the risk of bleeding while maintaining efficacy. Further, they have the potential to provide effective anticoagulation in indications where direct oral anticoagulants (DOACs) are proven less effective than vitamin K antagonists (VKAs) or when DOACs are contraindicated. The development of FXI inhibitors was based on mechanistic considerations suggesting FXI’s role in thrombus formation without significantly affecting hemostasis, supported by epidemiological data and animal experiments. FXI inhibitors, including antisense oligonucleotides, monoclonal antibodies, and small‑molecule inhibitors, target different stages of FXI production or activation, offering a diversity of therapeutic options with differing onset and offset of action, drug interaction potential, and renal elimination. FXI inhibitors have shown potential benefits in phase II trials, demonstrating similar or reduced bleeding rates to existing agents, including DOACs. The early termination of AZALEA‑TIMI 71 (Safety and Tolerability of Abelacimab [MAA868] vs Rivaroxaban in Patients With Atrial Fibrillation) and OCEANIC‑AF (A Study to Learn How Well the Study Treatment Asundexian Works and How Safe it is Compared to Apixaban to Prevent Stroke or Systemic Embolism in People With Irregular and Often Rapid Heartbeat [Atrial Fibrillation], and at Risk for Stroke) trials underscores challenges in the selection of appropriate patient populations and anticoagulant class, agent, and dose. Ongoing phase III trials including OCEANIC‑STROKE (A Study to Test Asundexian for Preventing a Stroke Caused by a Clot in Participants After an Acute Ischemic Stroke or After a High‑risk Transient Ischemic Attack, a So‑called Mini Stroke) and LIBREXIA trials aim to further explore the efficacy of FXI inhibitors in stroke, acute coronary syndrome, and atrial fibrillation. In conclusion, FXI inhibitors hold promise as next‑generation anticoagulants, potentially addressing limitations of current therapies. Ongoing research is required to establish their place in clinical practice and address unresolved questions.
Introduction
Cardiovascular disease remains the leading cause of mortality worldwide, with the World Health Organization estimating 17.9 million attributable deaths each year. Anticoagulants are commonly used to prevent and treat thromboembolism but currently available agents, including heparins, fondaparinux, vitamin K antagonists (VKAs), and direct oral anticoagulants (DOACs) possess inherent bleeding risks which may limit or preclude their use in patients at the highest risk of bleeding. The development of a new class of anticoagulants that target factor XI (FXI) has been hailed as a potential solution to mitigate bleeding, while providing effective anticoagulation. In this paper, we examine the rationale for the development of anticoagulants that target FXI and their potential future role. Specifically, we review the agents currently under clinical investigation, the available evidence regarding their efficacy and safety, the implications of recent trial discontinuations, and unresolved issues.
Current anticoagulation therapy
Unfractionated heparin (UFH) and VKAs were the only anticoagulants available for clinical use until the 1980s. While effective, several issues limited their routine use. UFH requires frequent bloodwork and careful dose adjustment, and its administration may be complicated by heparin‑induced thrombocytopenia, which affects 0.5% to 1% of patients and can be both limb- and life‑threatening.1 VKA therapy requires regular laboratory monitoring, because it is susceptible to labile anticoagulation effects and is plagued by multiple drug‑drug and drug‑food interactions.
Alternatives to UFH, including low‑molecular‑weight heparins (LMWHs) and fondaparinux, were introduced in the 1990s and early 2000s. Their more predictable pharmacokinetics and fixed once or twice daily dosing led to widespread adoption. LMWH is also associated with a much lower risk of heparin‑induced thrombocytopenia than UFH.2 However, these agents did not reduce the risk of bleeding.
More recently, DOACs have become the preferred anticoagulants for multiple indications, including stroke prevention in atrial fibrillation (AF) and the prevention and treatment of venous thromboembolism (VTE). Their advantages over VKAs include convenient fixed once or twice daily oral dosing, a low propensity for drug‑drug and drug‑food interactions, and a lower risk of bleeding, especially intracranial hemorrhage.3 However, DOACs also have limitations. They are less effective than VKAs for several indications and are still associated with important bleeding risks.
Rationale for development of new anticoagulants
A new class of anticoagulants that overcome the limitations of existing agents, and in particular, the inferior efficacy of DOACs as compared with VKAs for selected indications without increasing bleeding would be highly desirable.
Limited efficacy of existing agents
VKAs remain more efficacious than DOACs for several indications (Table 1). In patients with mechanical aortic or mitral valves, the RE‑ALIGN trial (Randomized, Phase II Study to Evaluate the Safety and Pharmacokinetics of Oral Dabigatran Etexilate in Patients after Heart Valve Replacement) found that dabigatran was associated with a higher risk of thromboembolic and bleeding events than warfarin.4 On‑X valves were purported to reduce thrombogenicity in comparison with conventional bileaflet valves, but when apixaban was compared with warfarin in patients with previously implanted On‑X aortic valves in the PROACT‑XA trial (A Trial to Determine if Participants With an On‑X Aortic Valve Can be Maintained Safely on Apixaban), apixaban was associated with a higher incidence of valve thrombosis or valve‑related thromboembolism.5 Superiority of VKAs relative to DOACs was also demonstrated for stroke prevention in AF in patients with rheumatic heart disease. The INVICTUS (Investigation of rheumatic AF Treatment Using Vitamin K Antagonists, Rivaroxaban or Aspirin Studies, Non‑Inferiority) trial found that in comparison with rivaroxaban, VKAs reduced the composite end point of stroke, systemic embolism, myocardial infarction (MI), and all‑cause mortality.6 Also, in antiphospholipid syndrome, pooled data from 4 randomized trials found a 5‑fold increased risk of arterial thrombosis with DOACs as compared with VKAs.7 Therefore, VKAs remain the standard of care for patients with triple positive disease antiphospholipid antibody syndrome, or a history of previous arterial events. There have also been concerns regarding the efficacy of standard DOAC dosing for stroke prevention in AF in patients with upper extremes of body weight. A recent patient‑level meta‑analysis, which included data from the 4 pivotal phase III trials found DOACs to be inferior to warfarin in patients with body mass index greater than or equal to 40 kg/m2 with respect to all‑cause death and the net clinical outcome of stroke, systemic embolism, major bleeding, or death.8
Abbreviations: DOAC, direct oral anticoagulant |
DOACs proven to be less effective than warfarin |
Mechanical valves |
Rheumatic atrial fibrillation |
Antiphospholipid antibody syndrome (triple positive and / or previous arterial thrombosis) |
Upper extremes of body weight (eg >150 kg) |
Existing therapies associated with high (unacceptable) bleeding risk |
End‑stage renal disease |
Advanced liver disease |
High risk for life‑threatening bleeding (eg, severe thrombocytopenia, recent ischemic stroke, cerebral amyloid angiopathy, extracorporeal membrane oxygenation) |
Recurrent major bleeding |
Other contraindications to the use of DOACs |
Drug interactions (eg, selected anticonvulsants, chemotherapeutics, antiretrovirals, antifungals, rifampin) |
Pregnancy |
Breastfeeding |
High risk of bleeding
Despite their lower risks of bleeding as compared with VKAs, DOACs are relatively contraindicated in patients at the highest risk for bleeding. This includes patients with advanced liver disease, end‑stage renal disease, uncontrolled hypertension, severe thrombocytopenia, or cerebral amyloid angiopathy. Similarly, patients with a history of recurrent major bleeding or intracranial hemorrhage may not be suitable candidates for standard or even reduced doses of DOACs.
Patients with an indication for anticoagulation who also require concomitant antiplatelet therapy, for example, patients with AF who undergo coronary or peripheral revascularization, are at elevated bleeding risk, particularly in the acute setting.
Combined anticoagulant and antiplatelet therapy, or dual pathway inhibition (DPI) reduces the risk of thromboembolic events vs antiplatelet therapy alone in patients with acute and chronic cardiovascular disease. The ATLAS‑ACS (Rivaroxaban versus Placebo in Patients with Acute Coronary Syndromes) trial found that in patients with recent MI, the combination of rivaroxaban 2.5 mg twice daily and antiplatelet therapy compared with antiplatelet therapy alone reduced the risk of MI, stroke, or cardiovascular mortality.9 The VOYAGER‑PAD (Efficacy and Safety of Rivaroxaban in Reducing the Risk of Major Thrombotic Vascular Events in Subjects With Symptomatic Peripheral Artery Disease Undergoing Peripheral Revascularization Procedures of the Lower Extremities) trial demonstrated that, in patients with peripheral arterial disease after lower‑limb revascularization, the combination of rivaroxaban 2.5 mg twice daily and antiplatelet therapy compared with antiplatelet therapy alone reduced the rate of acute limb ischemia, amputation, MI, ischemic stroke, and cardiovascular mortality.10 However, both trials reported an increased risk of major bleeding, and in ATLAS‑ACS there was also an increase in intracranial hemorrhage risk.
In chronic cardiovascular disease, the COMPASS (Rivaroxaban for the Prevention of Major Cardiovascular Events in Coronary or Peripheral Artery Disease) trial found that DPI with low‑dose rivaroxaban and aspirin compared with aspirin alone also provided important benefits for the prevention of major adverse cardiovascular events but increased the risk of major bleeding, mainly from the gastrointestinal tract.11 As such, patients with acute and chronic cardiovascular disease at high bleeding risk receiving DPI may experience an attenuated net clinical benefit from this therapy.
Other areas of unmet need
Patients with contraindications to DOACs include those with significant drug‑drug interactions, including certain anticonvulsant medications, antiretroviral drugs, chemotherapeutic agents, antifungal drugs, as well as patients who are pregnant or breastfeeding.
Rationale for targeting factor XI
The rationale for targeting FXI is based on mechanistic considerations, epidemiologic data, and the results of experiments in animals.
Mechanistic considerations
Traumatic vessel injury results in binding of extravascular tissue factor (TF) exposed at the site of injury to factor VII (FVII), thereby activating coagulation and driving hemostasis. Plaque rupture exposes intravascular TF to bind FVII and thereby also activates coagulation, but the amount of thrombin generation is insufficient to sustain thrombus formation and requires amplification via FXI. Thrombin also amplifies factors V and VIII, and the relative importance of FXI amplification as compared with other factors is unknown. FXI can also be activated by activated factor XII (FXIIa) via the contact pathway. FXII activation occurs after exposure to naturally occurring negatively charged entities (eg, neutrophil extracellular traps, polyphosphates, nucleic acids, activated platelets) or negative charge accumulation on medical devices devoid of a protective layer of endothelial cells, including mechanical heart valves, vascular grafts, stents, catheters, and dialysis circuits.12,13
The relative importance of FXI amplification of thrombin generation in thrombus formation compared with hemostasis suggests that blocking thrombin amplification by targeting FXI could prevent pathologic thrombus formation after plaque rupture with little or no increase in bleeding. An additional potential benefit of FXI inhibition is to prevent thrombus formation on medical devices.
Epidemiologic data
First described in 1953 by Robert Rosenthal, inherited FXI deficiency (hemophilia C) is an autosomal dominant condition affecting up to 9% of Ashkenazi Jews.14,15 Cohort studies have demonstrated that persons with inherited FXI deficiency have lower rates of thrombosis than the general population, with little or no increase in bleeding. Affected patients may be at increased risk of mucosal bleeding16 but have lower risk of both VTE and stroke,17 although not MI.18 These observations provide an epidemiologic basis for FXI as a potentially safe and effective antithrombotic target.
Experiments in animals
Animal models demonstrate that factor XI inhibition reduces thrombosis rates. FXI‑deficient mice have decreased rates of spontaneous, chemically‑induced, and catheter‑provoked thrombosis without obvious hemostatic abnormalities.19
Review of factor XI inhibitor agents in clinical development
FXI inhibitor agents that have been evaluated in phase II or III clinical trials include antisense oligonucleotides (ASOs), monoclonal immunoglobulin (Ig) G antibodies, and small‑molecule inhibitors (Figure 1 and Table 2). Other agents still in early preclinical development include natural peptides and aptamers.
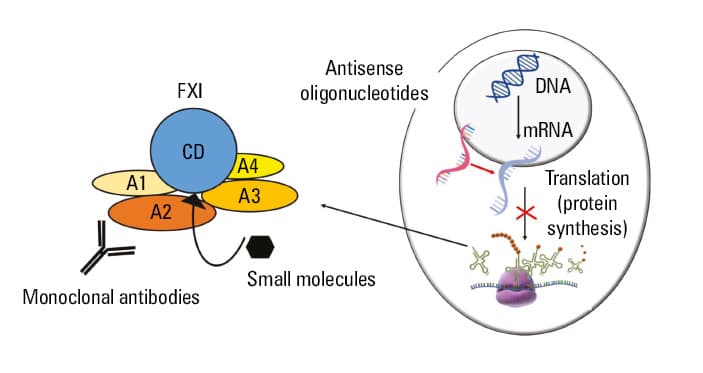
Abbreviations: A, apple domain; CD, catalytic domain
Class | Agent | Mechanism of action | Route and frequency of administration | Onset | Half‑life | Drug interactions | Renal excretion |
Abbreviations: F, factor; Ig, immunoglobulin; P‑GP, P‑glycoprotein | |||||||
Antisense oligonucleotides | IONIS‑FXI‑LRX (fesomersen) | Binding to mRNA in hepatocytes inhibiting FXI production | Subcutaneous (monthly) | Slow (1 week) | 10–20 days | No | No |
Monoclonal antibodies (IgG) | Abelacimab | Competitive inhibition of FXI activation by thrombin and FXIIa; also inhibition of FXIa | Intravenous or subcutaneous (monthly) | Intravenous: rapid (minutes or hours) Subcutaneous: slower (days) | 20–30 days | No | No |
Osocimab | Noncompetitive inhibition of FXIa | Intravenous or subcutaneous (monthly) | 30–44 days | ||||
Xisomab | Noncompetitive inhibition of FXI activation by FXIIa | Intravenous (single dose) | 11–121 hours | ||||
Small‑molecule inhibitors | Asundexian | Competitive inhibition of FXIa | Oral (daily) | Rapid (hours) | 14–21 hours | 3A4 and P‑GP substrates | Minimal |
Milvexian | Oral (twice daily) | 11–18 hours | |||||
Frunexian | Intravenous (continuous infusion) | Very rapid (minutes) | 70–90 minutes | No | |||
Antisense oligonucleotides
ASOs bind to mRNA in hepatocytes, preventing its translation into the FXI protein, thereby reducing FXI levels to mimic a state of inherited FXI deficiency. The prolonged duration of action of ASOs makes them particularly attractive in patients requiring a short course of anticoagulation (eg, for total hip or knee arthroplasty), as a single dose may cover the entire treatment duration. The second‑generation ASO, fesomersen, has an N‑acetyl galactosamine (GalNAc) conjugation promoting maximum drug delivery to hepatocytes resulting in a longer half‑life. The onset of action of ASOs, however, remains limited by their mechanism of action; time is required to achieve a state of FXI deficiency after arresting protein synthesis by mRNA inhibition (circulating FXI half‑life is 50 h).
Antibodies
Monoclonal IgG antibodies under development include abelacimab, osocimab, and xisomab. These agents competitively or noncompetitively inhibit FXI and / or FXIa and have a more rapid onset of action than ASOs enabling their use in acute indications.
Small‑molecule inhibitors
Asundexian and milvexian are low‑molecular‑weight chemical compounds that competitively inhibit FXIa. With a rapid onset of action and oral administration, they are potentially advantageous for patients with chronic indications for anticoagulation. Their shorter half‑life may be desirable in patients who are at high risk of bleeding or require urgent surgery.
Hemostatic agents and specific reversal agents in patients with factor XI inhibitor–associated bleeding
FXI inhibitors prolong activated partial thromboplastin time (aPTT) in a dose‑dependent manner.20 In patients treated with a FXI inhibitor who experience bleeding or require urgent surgery, clinicians may consider treatments to correct the aPTT or enhance hemostasis. In patients treated with an ASO, FXI replacement can correct the hemostatic defect. In patients treated with an antibody or small‑molecule inhibitor, FXI replacement is unlikely to be helpful but general hemostatic agents, such as prothrombin complex concentrates or recombinant factor VIIa (FVIIa), may provide benefits. In patients with inherited FXI deficiency, recombinant FVIIa has been shown to prevent bleeding complications and the need for perioperative blood products, even in severely deficient patients.21 Tranexamic acid appears to be a useful adjunctive agent, because FXI inhibitors may reduce activation of thrombin‑activatable fibrinolysis inhibitor leading to increased fibrinolysis.22 Defective fibrin clot structure has been identified as a possible contributor to bleeding in patients with FXI deficiency.23
Although it is relevant to consider the need for specific reversal agents for FXI inhibitors, no patient in any of the published phase II FXI inhibitor trials required administration of FXI concentrate or a general hemostatic agent, such as a prothrombin complex concentrate or recombinant FVIIa.
Phase II clinical trials of factor XI inhibitors
Promising proof‑of‑concept studies have been published for several FXI inhibiting agents, including ASOs, monoclonal antibodies, and small‑molecule inhibitors.24-31 Although none of the individual phase II trials were powered for efficacy, most showed similar bleeding rates as compared with placebo and lower bleeding rates as compared with active control (Table 3).
Drug | Trial | Indication | Patients, n | Intervention | Control | Primary outcome |
Abbreviations: ACS, acute coronary syndrome; BARC, Bleeding Academic Research Consortium; CRNMB, clinically relevant nonmajor bleeding; DVT, deep vein thrombosis; MACE, major adverse cardiovascular event; MB, major bleeding; MRI, magnetic resonance imaging; TKA, total knee arthroplasty; VTE, venous thromboembolism | ||||||
Fesomersen | FXI‑ASO TKA24 | VTE prevention after TKA | 293 | 200 or 300 mg subcutaneously | Enoxaparin 40 mg subcutaneously once daily | Reduction in VTE (on mandatory bilateral venography or symptomatic events) with 300 mg dose compared with control and numeric reduction in MB/CRNMB with 200 and 300 mg compared with control |
Osocimab | FOXTROT30 | VTE prevention after TKA | 787 | Various doses, intravenously | Enoxaparin 40 mg subcutaneously once daily or apixaban 2.5 mg orally twice daily | Reduction in VTE (on mandatory bilateral venography or symptomatic events) with 1.8 mg/kg preoperative dose and similar rate with 0.6, 1.2, and 1.8 mg/kg postoperative dose and similar or reduced MB/CRNMB |
Abelacimab | ANT‑005 TKA29 | VTE prevention after TKA | 409 | 30, 75, or 150 mg, intravenously | Enoxaparin 40 mg subcutaneously once daily | Reduction in VTE (on mandatory venography of surgical leg or symptomatic events) at 75 and 150 mg doses (similar at 30 mg dose) and no difference in MB/CRNMB |
Milvexian | AXIOMATIC‑TKR31 | VTE prevention after TKA | 1219 | 25, 50, or 200 mg orally once daily or 25, 50, 100, or 200 mg orally twice daily | Enoxaparin 40 mg subcutaneously once daily | Reduction in VTE (asymptomatic DVT, confirmed symptomatic VTE or death from any cause) at 200 mg daily and 100 and 200 mg twice daily dosing and no difference in bleeding |
AXIOMATIC‑SSP27 | Secondary stroke prevention | 2295 | 25 mg orally daily or 25, 50, 100, or 200 mg orally twice daily | Placebo | Similar new symptomatic ischemic stroke or new covert brain infarct on MRI (new symptomatic ischemic strokes numerically reduced at several doses) and numeric increase in MB at 50 mg twice daily and higher doses | |
Asundexian | PACIFIC‑AF25 | Stroke prevention in AF | 753 | 20 or 50 mg orally once daily | Apixaban 5 mg orally twice daily | Reduction in MB/CRNMB |
PACIFIC‑STROKE28 | Secondary stroke prevention | 1808 | 10, 20, or 50 mg orally once daily | Placebo | No dose‑response effect on composite of incident MRI‑detected covert brain infarcts and recurrent symptomatic ischemic stroke (numeric reduction in recurrent symptomatic stroke with asundexian 50 mg) and numeric increase in MB/CRNMB | |
PACIFIC‑AMI26 | Prevention of MACE post ACS | 1601 | 10, 20, or 50 mg orally once daily | Placebo | Dose‑dependent FXIa inhibition and similar risk of BARC type 2, 3, or 5 bleeding | |
Further insights into the potential for FXI inhibitors come from pooled phase II trial data. A meta‑analysis of 4 phase II trials of FXI inhibitors in patients undergoing total knee replacement (TKR) demonstrated superiority of FXI inhibitors over prophylactic doses of LMWH with respect to efficacy (relative risk [RR], 0.62; 95% CI, 0.49–0.79), with greater efficacy with higher doses (P interaction <0.001). FXI inhibitors were also associated with less bleeding (RR, 0.49; 95% CI, 0.31–0.77), although there was no apparent difference in safety between higher and lower doses (P interaction = 0.73). When data from 2 phase II trials comparing FXI inhibitors with apixaban after TKR or for stroke prevention in AF were pooled, results revealed no differences in efficacy or bleeding. Finally, when 3 phase II trials of small‑molecule inhibitors compared with placebo in patients with recent noncardioembolic stroke or MI were combined, there was no difference in the trial‑defined efficacy end point (RR, 1.02; 95% CI, 0.92–1.13) or major bleeding (RR, 1.21; 95% CI, 0.75–1.93), but there was an increase in clinically relevant nonmajor bleeding (RR, 1.25; 95% CI, 1.08–1.43).32
Latest clinical developments with factor XI inhibitors
In the past 6 months, 2 international, multicenter randomized trials comparing FXI inhibitor therapy with DOACs in patients with AF were terminated following recommendations of their respective data safety monitoring boards, for superior safety (AZALEA‑TIMI 71) and inferior efficacy (OCEANIC‑AF).
The phase II AZALEA‑TIMI 71 trial (presented; not yet published) compared 2 doses of a monoclonal IgG antibody abelacimab (150 mg and 90 mg subcutaneously once monthly) with rivaroxaban 20 mg daily in patients with AF and a CHA2DS2-VASc score equal to or above 4 or a CHA2DS2-VASc score equal to or above 3 and 1 or more risk factors for bleeding. The study included 1287 patients (median CHA2DS2-VASc score of 5, previous bleeding 7%, planned concomitant antiplatelet use 26%), and found that both doses of abelacimab reduced the primary end point of major or clinically relevant nonmajor bleeding (150 mg vs rivaroxaban, 2.7% vs 8.1%; hazard ratio [HR], 0.33; 95% CI, 0.19–0.55; P <0.001 and 90 mg vs rivaroxaban, 1.9% vs 8.1%; HR, 0.23; 95% CI, 0.13–0.42; P <0.001) as well as major bleeding (1% vs 3.7%; HR, 0.26; 95% CI, 0.11–0.61; P = 0.002 and 0.7% vs 3.7%; HR, 0.19; 95% CI, 0.07–0.5; P <0.001). There was no significant difference between groups with respect to the secondary end point of stroke or systemic embolism (abelacimab 150 mg vs rivaroxaban, 1.1% vs 1%; HR, 1.13; 95% CI, 0.41–3.12; P = 0.81 and abelacimab 90 mg vs rivaroxaban, 1.4% vs 1%; HR, 1.45; 95% CI, 0.55–3.8; P = 0.45). However, this outcome was exploratory and the low event rates leave the question of efficacy of abelacimab in AF unanswered.
The phase III OCEANIC‑AF trial (not yet presented or published) compared the small‑molecule inhibitor asundexian with apixaban in AF patients with a CHA2DS2-VASc score equal to or above 3 if male or equal to or above 4 if female, or a CHA2DS2-VASc score of 2 if male or 3 if female with additional enrichment criteria. After enrollment of 14 830 patients, the independent data monitoring committee recommended stopping the trial due to inferior efficacy of asundexian as compared with apixaban.
Possible explanations for early termination of the 2 factor XI inhibitor trials
Consideration of indications for FXI treatment, drug class, agent, and dosing issues may help to inform the interpretation of these results.
Treatment indications
The AZALEA‑TIMI 71 study was not powered to demonstrate efficacy of abelacimab, and although OCEANIC‑AF demonstrated that the small‑molecule inhibitor, asundexian, was less effective than apixaban, it may still be more effective than no anticoagulation for stroke prevention. If so, this would be consistent with the epidemiologic data suggesting that FXI deficiency is associated with a lower risk of stroke.
Drug classes and agents
Different drug classes or specific agents within a class may have different effects. ASOs prevent production of FXI, antibodies prevent activation of FXI and / or inhibit FXIa, and small‑molecule inhibitors inhibit FXIa. It is unclear which of these mechanisms is associated with greatest benefit.
Dosing
Determining the optimal dose of a new anticoagulant to test in a phase III trial is always challenging, because earlier‑phase trials are never powered for efficacy. Some have suggested that inadequate asundexian dosing in OCEANIC‑AF trial (50 mg daily) explains its inferior efficacy in comparison with apixaban. Asundexian dose selection was based on the results of phase II dose‑finding studies and the results of laboratory testing demonstrating 91% and 92% inhibition of FXIa activity at trough levels in phase II trials PACIFIC‑AMI (Study to Gather Information About the Proper Dosing and Safety of the Oral FXIa Inhibitor BAY 2433334 in Patients Following an Acute Heart Attack) and PACIFIC‑AF (Study to Gather Information About the Proper Dosing of the Oral FXIa Inhibitor BAY 2433334 and to Compare the Safety of the Study Drug to Apixaban, a Non‑vitamin K Oral Anticoagulant [NOAC] in Patients with Irregular Heartbeat [Atrial Fibrillation] that Can Lead to Heart‑related Complication), respectively.25,26 In the phase II AZALEA‑TIMI 71 trial, abelacimab 90 mg and 150 mg achieved 97% and 99% inhibition of FXI activity, respectively, suggesting that even higher levels of FXI inhibition do not compromise safety. However, the 2 drugs work through distinct mechanisms, and it is not possible to directly compare the assays, one of which measured FXIa activity, and the other which measured FXI activity using a novel assay with a kaolin trigger and fluorogenic substrate readout.
In summary, the AZALEA‑TIMI 71 and OCEANIC‑AF trials were both performed in patients with AF but they tested different drugs, dose selection was based on different laboratory assays, the comparator drugs were different, and perhaps most importantly, AZALEA‑TIMI 71 was a phase II safety trial that was not powered for efficacy, whereas OCEANIC‑AF was a phase III trial powered for efficacy.
Ongoing phase III trial programs
There are currently multiple ongoing phase III trial programs of FXI inhibitors, testing asundexian in stroke (OCEANIC‑STROKE); milvexian in MI, stroke, and AF (LIBREXIA trials); and abelacimab in AF (LILAC‑TIMI 76) and cancer‑associated thrombosis (ASTER [A Study Comparing Abelacimab to Apixaban in the Treatment of Cancer‑associated Venous Thromboembolism] and MAGNOLIA [A Multicenter, Randomized, Open‑label, Blinded Endpoint Evaluation, Phase 3 Study Comparing the Effect of Abelacimab vs. Dalteparin on Venous Thromboembolism {VTE} Recurrence and Bleeding in Patients With GI/GU Associated VTE]) (Table 4). The results of these trials will be pivotal in evaluation of FXI inhibitors as viable treatments for the prevention and treatment of thromboembolism.
Drug | Trial | Indication | Patients, n | Intervention | Control | Primary outcomes |
Abbreviations: CNS, central nervous system; CV, cardiovascular; ISTH, International Society of Thrombosis and Hemostasis; MI, myocardial infarction; PE, pulmonary embolism; others, see Table 3 | ||||||
Asundexian | OCEANIC‑STROKE (NCT05686070) | Secondary stroke prevention | 9300 | 50 mg orally once daily | Placebo | Time to first occurrence of ischemic stroke and time to first occurrence of ISTH MB |
Milvexian | LIBREXIA‑AF (NCT05757869) | Stroke prevention in AF patients | 15 500 | 100 mg orally twice daily | Apixaban | Time to first occurrence of composite end point of stroke and non‑CNS systemic embolism |
LIBREXIA‑ACS (NCT05754957) | Secondary MACE prevention following ACS | 16 000 | 25 mg orally twice daily | Placebo | Time to first occurrence of MACE (composite of CV death, MI, and ischemic stroke) | |
LIBREXIA‑STROKE (NCT05702034) | Secondary stroke prevention | 15 000 | 25 mg orally twice daily | Placebo | Time to first occurrence of ischemic stroke | |
Abelacimab | LILAC‑TIMI 76 (NCT05712200) | AF patients deemed unsuitable for oral anticoagulation | 1900 | 150 mg subcutaneously once monthly | Placebo | Time to first ischemic stroke or systemic embolism and time to the first occurrence of BARC type 3c/5 bleeding |
ASTER (NCT05171049) | Cancer‑associated VTE | 1655 | 150 mg single dose intravenously, then subcutaneously once monthly | Apixaban | Time to first event of centrally adjudicated VTE recurrence (new proximal DVT, new PE or fatal PE, including unexplained death for which PE cannot be ruled out) | |
MAGNOLIA (NCT05171075) | Gastrointestinal / genitourinary cancer‑associated VTE | 1020 | 150 mg single dose intravenously, then subcutaneously once monthly | Dalteparin 200 units/kg/day, followed by 150 units/kg/day | Time to first event of centrally adjudicated VTE recurrence (new proximal DVT, new PE, or fatal PE, including unexplained death for which PE cannot be ruled out) | |
Asundexian for prevention of recurrent stroke (OCEANIC‑STROKE)
The Independent Data Monitoring Committee which recommended stopping the asundexian trial for AF recommended continuation of the phase III OCEANIC‑STROKE trial. OCEANIC‑STROKE is recruiting 9300 patients to examine efficacy of asundexian 50 mg daily compared with placebo (on a background of standard antiplatelet therapy) for secondary prevention after noncardioembolic stroke or high‑risk transient ischemic attack (TIA).
Milvexian for stroke prevention in atrial fibrillation, prevention of recurrent ischemic stroke, and prevention of recurrent cardiac events (LIBREXIA program)
Three ongoing phase III trials, LIBREXIA‑AF, LIBREXIA‑STROKE, and LIBREXIA‑ACS, are examining the efficacy of another oral small‑molecule drug, milvexian.
LIBREXIA‑AF, which compares milvexian to apixaban for stroke prevention in AF, will be of particular interest, as an indirect comparator between milvexian (at a higher dose of 100 mg twice daily) and asundexian, given the termination of the OCEANIC‑AF, where asundexian was tested at a dose of 50 mg daily.
LIBREXIA‑STROKE compares milvexian 25 mg twice daily with placebo on a background of standard antiplatelet therapy in patients post noncardioembolic stoke or high‑risk TIA. Notably, the dose being tested in this trial is lower than the 100 mg twice daily dose being studied in the LIBREXIA‑AF; however, patients will also be receiving concurrent antiplatelet therapy, which may allow them to benefit from lower doses of anticoagulant in the context of DPI.
LIBREXIA‑ACS is comparing milvexian 25 mg twice daily against placebo on a background of standard antiplatelet therapy in patients with recent ACS (within 7 days) undergoing medical management or percutaneous coronary intervention. As with the LIBREXIA‑STROKE trial, this study uses a lower dose of milvexian in the context of concomitant antiplatelet therapy. While there was no signal for benefit of asundexian in the phase II PACIFIC‑MI trial, if milvexian proves effective in the phase III LIBREXIA‑ACS trial, it may provide a lower bleeding risk DPI therapy alternative in this population who remain at high risk for recurrent cardiovascular events despite DPI.
Abelacimab for stroke prevention in atrial fibrillation
LILAC‑TIMI 76 trial is comparing abelacimab 150 mg monthly to placebo in patients with AF deemed unsuitable for oral anticoagulation or left atrial appendage closure.
Patients with AF at high bleeding risk may not be able to tolerate currently available anticoagulants at doses tested in the pivotal phase III trials for optimal stroke prevention. Elderly individuals form an increasingly large and important population of patients with AF at high bleeding risk who are often also at elevated stroke risk due to shared risk factors.33 ELDERCARE‑AF (Edoxaban Low‑Dose for Elder Care Atrial Fibrillation Patients) trial demonstrated that reduced‑dose edoxaban (15 mg daily) in elderly patients deemed inappropriate for anticoagulation at standard doses approved for stroke prevention in AF was effective for stroke prevention, but still numerically increased major bleeding compared with placebo (3.3% vs 1.8%; HR, 1.87; 95% CI, 0.9–3.89; P = 0.09).34 If abelacimab is effective for stroke prevention and associated with an acceptable bleeding profile in patents with AF not suitable for treatment with existing therapies, it would address an important therapeutic gap.
Conclusions
There is cautious optimism with respect to the potential of FXI agents to provide effective anticoagulation without increasing bleeding. Ongoing studies will establish whether FXI agents could replace VKAs for indications in which DOACs are less effective or contraindicated, or whether they could be safely used in patients at the highest risk for bleeding. However, many outstanding questions remain (Table 5), which await the results of ongoing randomized trials.
Are there important efficacy and safety differences between classes or agents? |
Are they as effective or more effective than existing agents in AF? |
Can they replace VKAs for indications where DOACs have failed? |
Can they be used in indications where existing agents cannot be used? |
How much do they increase bleeding risk compared with placebo? |
How should they be managed periprocedurally? |
Are reversal agents required? |
Can they be used in advanced kidney and liver disease? |
Are there any significant drug‑drug interactions? |
Are there any unexpected long‑term side effects? |
Are they cost‑effective? |
- Arepally GM, Padmanabhan A. Heparin‑induced thrombocytopenia: a focus on thrombosis. Arterioscler Thromb Vasc Biol. 2021; 41: 141‑152. | Crossref
- Martel N, Lee J, Wells PS. Risk for heparin‑induced thrombocytopenia with unfractionated and low‑molecular‑weight heparin thromboprophylaxis: a meta‑analysis. Blood. 2005; 106: 2710‑2715. | Crossref
- Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta‑analysis of randomised trials. Lancet. 2014; 383: 955‑962. | Crossref
- Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves. N Engl J Med. 2013; 369: 1206‑1214. | Crossref
- Wang TY, Svensson LG, Wen J, et al. Apixaban or warfarin in patients with an On‑X mechanical aortic valve. NEJM Evid. 2023; 2: EVIDoa2300067. | Crossref
ARTICLE INFORMATION