Hyperthyroidism caused by massive toxic nodular goiter accompanied by primary hyperparathyroidism

 CC BY 4.0
CC BY 4.0
Hyperthyroidism caused by massive toxic nodular goiter accompanied by primary hyperparathyroidism
Hyperthyroidism is characterized by increased production of thyroid hormones, with diverse etiology and treatment methods.1 The most common cause is Graves’ disease, followed by toxic multinodular goiter (MNG).2 Primary hyperparathyroidism (PHP) is another frequent endocrinopathy, caused primarily by parathyroid hormone (PTH)-secreting adenoma.3 Coexistence of nontoxic MNG with PHP is common; however, a combination of PHP with toxic MNG is less frequently observed.4
We present a case of a 76‑year‑old woman who was admitted to a department of endocrinology for diagnostic workup of suspected mediastinal goiter and qualification for surgical treatment.
Initially, the patient was diagnosed with hyperthyroidism in 2018 (Graves’ disease was excluded), and was subsequently treated with thiamazole for 15 months. As permanent euthyroid status was not achieved, she underwent radioiodine therapy with an activity of 800 MBq in 2019. Due to a relapse of the disease, treatment was repeated twice, 800 MBq in 2020 and 740 MBq in 2021. Thyroid scintigraphy showed inhomogenous uptake of 99mTc‑pertechnetate in the nodular goiter located in the neck and only slight radiotracer accumulation in the upper mediastinum. Due to poor response to radioiodine treatment, it was decided to expand the anatomic range of imaging after the third administration of 131I. Single‑photon emission computed tomography / computed tomography (CT) of the chest showed a heterogeneous mediastinal mass extending up to the diaphragm and compressing the right lung and some other structures. The large tumor showed heterogenous accumulation of 131I (Figure 1A and 1B). Based on these findings, the patient was admitted to our department for further clinical evaluation with a perspective of surgical treatment.
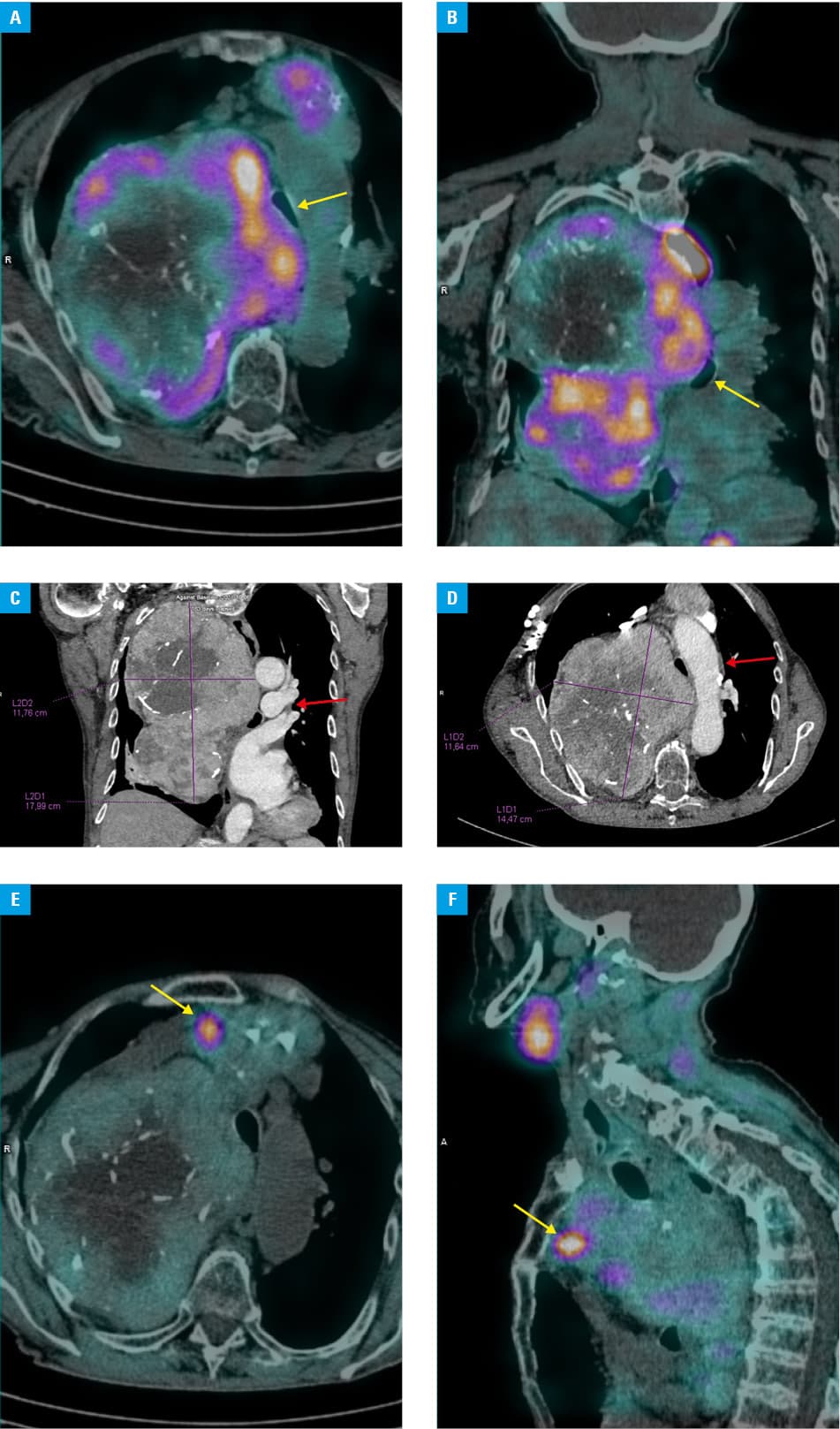
On admission, she presented with subclinical hyperthyroidism. Laboratory test results showed a thyroid‑stimulating hormone level of 0.17 μIU/ml (reference range [RR], 0.27–4.2 μIU/ml), free thyroxine level of 11.1 pmol/l (RR, 11.5–21 pmol/l), and free triiodothyronine level of 4.97 pmol/l (RR, 3.9–6.7 pmol/l). Physical examination showed increased neck circumference and visible collateral circulation. Neck and chest CT confirmed a massive goiter modeling the cervical and thoracic vessels, without evidence of infiltration. The mass extended on the left side to the level of the brachiocephalic trunk and on the right side to the diaphragm, compressing the trachea, esophagus, and right lung, and causing atelectasis of the right lower lobe (Figure 1C and 1D).
Moreover, we diagnosed vitamin D3 deficiency (9 ng/ml; recommended range, 30–80 ng/ml) and primary hyperparathyroidism with markedly elevated concentrations of PTH (410 pg/ml; RR, 15–65 pg/ml), total calcium (12.32 mg/dl; RR, 8.8–10.2 mg/dl), and ionized calcium (6.44 mg/dl; RR, 4.2–5.2 mg/dl), and a decreased level of phosphate (2 mg/dl; RR, 2.7–4.5 mg/dl). Subtraction scintigraphy of the parathyroid glands with 99mTc‑methoxyisobutylisonitrile revealed a hot spot in the immediate vicinity of the goiter behind the sternal manubrium, suggesting parathyroid adenoma (Figure 1E and 1F). Despite comorbidities, the patient was referred to a thoracic surgery department. After surgery, diagnosis of MNG and parathyroid adenoma was confirmed on histopathologic examination.
Hyperthyroidism caused by toxic goiter often requires sequential use of various treatment methods. Clinical status, additional test results, and patient preferences should be considered for a personalized approach. Radioiodine therapy is effective in achieving euthyroidism; however, surgery remains the treatment of choice in the case of large goiter causing airway compression. PHP may coexist with other thyroid diseases, and should be taken into account in this group of patients.5
- Chaker L, Cooper DS, Walsh JP, Peeters RP. Hyperthyroidism. Lancet. 2024; 403: 768‑780. | Crossref
- Lee SY, Pearce EN. Hyperthyroidism: a review. JAMA. 2023; 330: 1472‑1483. | Crossref
- Kowalski GJ, Buła G, Żądło D, et al. Primary hyperparathyroidism. Endokrynol Pol. 2020; 71: 260‑270. | Crossref
- Jarząb B, Dedecjus M, Lewiński L, et al. Diagnosis and treatment of thyroid cancer in adult patients – recommendations of Polish Scientific Societies and the National Oncological Strategy. 2022 Update [in Polish]. Endokrynol Pol. 2022; 73: 173‑300.
- Regal M, Páramo C, Luna Cano R, et al. Coexistence of primary hyperparathyroidism and thyroid disease. J Endocrinol Invest. 1999; 22: 191‑197. | Crossref
ARTICLE INFORMATION