A 65‑year‑old woman was admitted to a surgical department due to nodular goiter causing tracheal shift to the right. Her medical history was unremarkable. Slightly increased inflammatory marker levels were noted upon admission (white blood cell count, 12 390/μl [reference range, 4000–10 000/μl]; C‑reactive protein, 11.6 mg/l [reference range, 0.4–5 mg/l]). The patient underwent left thyroid lobectomy and drainage of intraoperatively found thyroid abscess (culture showed methicillin‑sensitive Staphylococcus aureus). Postoperative course was uneventful and the patient was discharged.
Pathologic examination of a surgical specimen showed areas of normal thyroid follicles accompanied by inflammatory infiltration and nests of squamous epithelial cells with keratin pearls, consistent with keratinizing squamous cell carcinoma (SCC; Figure 1A). A suspicion of metastatic SCC was raised. However, chest X‑ray, laryngologic consultation, esophagogastroduodenoscopy, and dermatoscopy showed no potential primary site in the lungs, oral cavity, pharynx, larynx, esophagus, and skin, respectively.
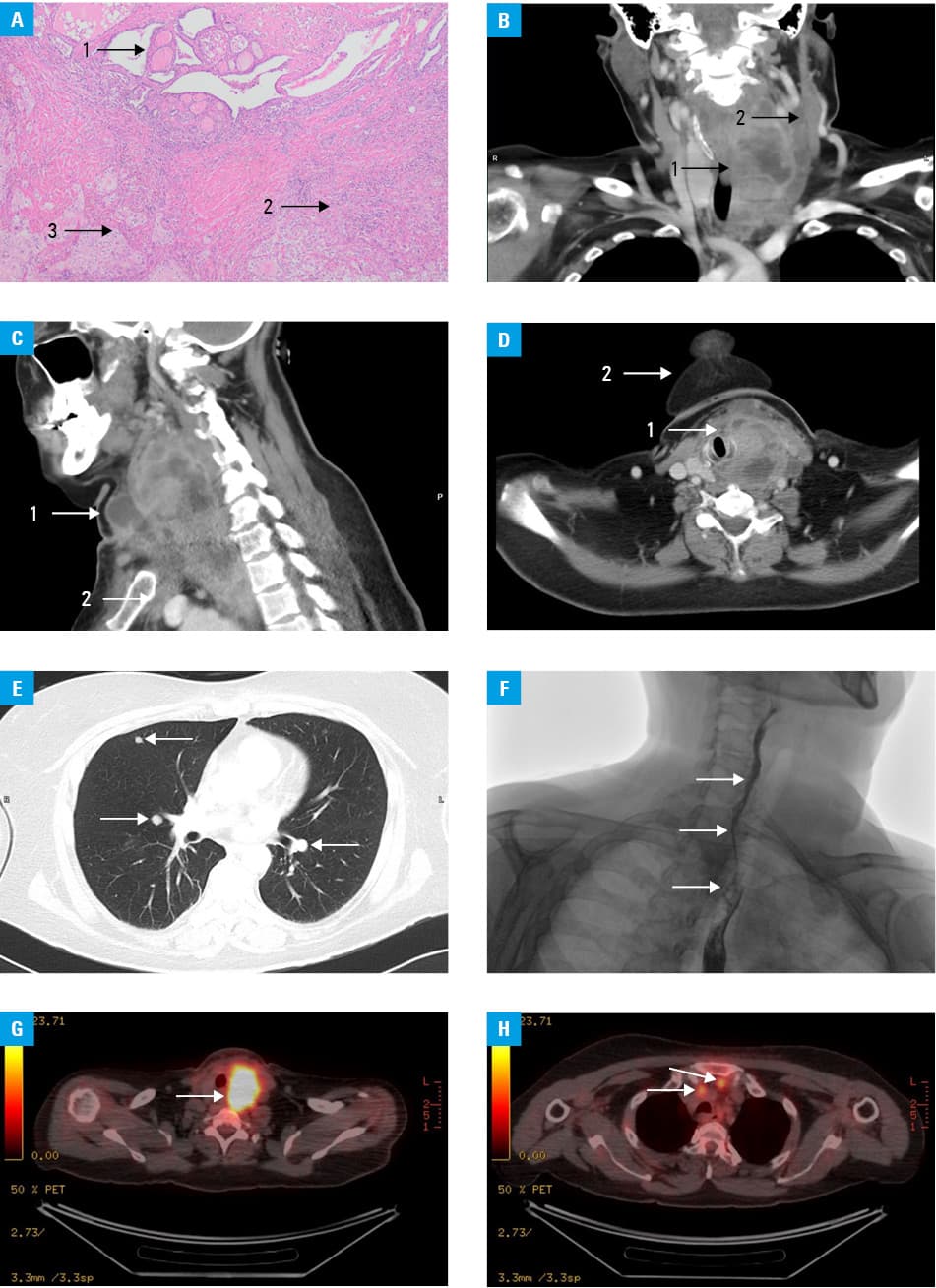
Over 9 weeks following the operation, the patient developed signs of recurrence and dissemination. Contrast‑enhanced computed tomography (CT) of the neck and chest showed extensive neoplastic infiltration with areas of fluid and abscesses, measuring 130 mm × 75 mm × 75 mm (craniocaudal × anterior‑posterior × transverse plane). It caused thrombosis of the left internal jugular vein (Figure 1B), extended down to the retrosternal area and upper mediastinum (Figure 1C), protruded to the front of the neck, and shifted the trachea and esophagus to the right (Figure 1D). Pathologic bilateral cervical and upper mediastinal lymph nodes were noted, together with multiple tumors of both lungs, measuring 10 to 11 mm, which were consistent with metastases (Figure 1E). X‑ray with oral contrast swallow confirmed esophageal stenosis (Figure 1F). Positron emission tomography (PET) showed metabolically‑active neoplastic infiltration of the operated area (maximum standardized uptake value, 13.5; Figure 1G) and pathologic cervical, retropharyngeal, and retrosternal lymph nodes (Figure 1H). Significant leukocytosis of up to 93 000/μl was observed, and blood smear showed mainly mature forms of neutrophils.
Following an oncologic consultation, the patient underwent palliative platinum‑based chemotherapy and external beam radiation therapy. Unfortunately, she died several months after the diagnosis.
Primary SCC is one of the rarest (prevalence, 0.1%–0.7%) malignancies of the thyroid gland. To date, slightly more than 100 cases have been described in medical literature. The disease typically affects women (female to male ratio of 1.4–2.4 to 1) in their fifth to seventh decade of life. Presentation most often resembles that of anaplastic thyroid cancer and includes rapidly progressive neck swelling (60%), dyspnea / dysphagia (20%), hoarseness (15%), cervical lymphadenopathy, and weight loss. Paraneoplastic syndromes may appear, such as leukocytosis attributed to granulocyte colony stimulating factor secretion by the tumor.1-5
Fine‑needle aspiration biopsy may point to the diagnosis, but not in every case. Additional tests, such as panendoscopy, are useful in excluding infiltration / metastasis from other primary sites, which is 10 times more probable than primary thyroid SCC. Magnetic resonance imaging, CT, and PET may be used to evaluate the extent of the disease and guide appropriate therapy.1-5
There is no consensus regarding treatment, but surgical resection (thyroidectomy, cervical lymph node dissection) followed by chemo‑radiation is recommended, although response to adjuvant therapy may be poor. Due to high aggressiveness and mostly advanced stage at the time of diagnosis, the prognosis remains poor, with median overall survival of 6 to 8 months.1-5
- Mohd‑Irman‑Shah I, Yusri‑Rahimi J, Nurul‑Nadhihah A, Irfan M. Primary squamous cell carcinoma of the thyroid gland. Iran J Otorhinolaryngol. 2018; 30: 65‑68.
- Struller F, Senne M, Falch C, et al. Primary squamous cell carcinoma of the thyroid: case report and systematic review of the literature. Int J Surg Case Rep. 2017; 37: 36‑40. | Crossref
- King‑yin Lam A. Squamous cell carcinoma of thyroid: a unique type of cancer in World Health Organization Classification. Endocr Relat Cancer 2020; 27: R177‑R192. | Crossref
- Makay O, Kaya T, Ertan Y, et al. Primary squamous cell carcinoma of the thyroid: report of three cases. Endocr J. 2008; 55: 359‑364. | Crossref
- Tunio MA, Al Asiri M, Fagih M, Akasha R. Primary squamous cell carcinoma of thyroid: a case report and review of literature. Head Neck Oncol. 2012; 4: 8. | Crossref
ARTICLE INFORMATION