We present a case of a 52‑year‑old man with Chilaiditi syndrome (CHS). The patient exhibited escalating abdominal pain localized in the right upper quadrant, accompanied by nausea, irregular bowel movements, increased intestinal gas, and loose stools. Additionally, he reported dyspnea that exacerbated during speech and while in a supine position, but notably subsided with physical activity. Further clinical assessment showed generalized weakness, chronic fatigue, and sleep disturbances attributed to pain in the large joints. The patient had a history of idiopathic, right‑sided diaphragmatic paralysis, and he underwent diaphragm plication in 2019. Although flaccidity of the diaphragm was initially reduced, 3 years postoperatively the symptoms of diaphragmatic paralysis re‑emerged.
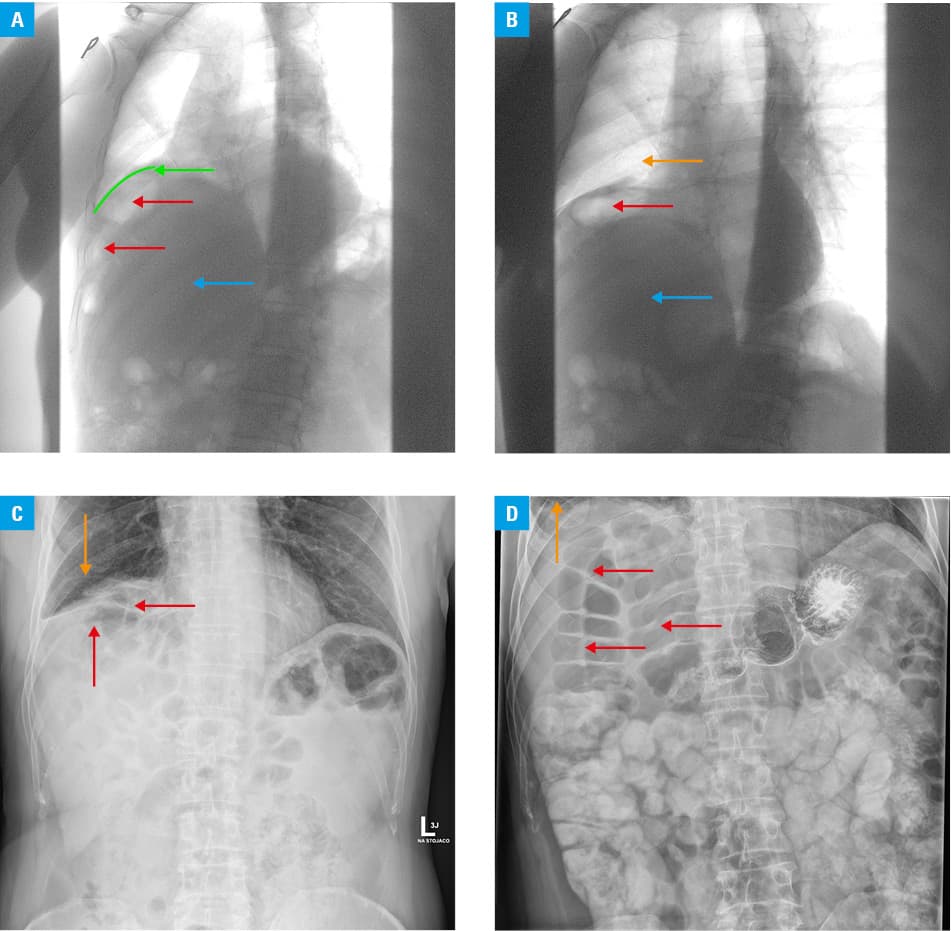
Abdominal and pelvic X‑ray imaging revealed significant elevation of the right hemidiaphragm, with narrow bands of atelectasis visible above the diaphragm due to compression (Figure 1A–1C). The colon was visible anteriorly from segment 8 of the liver. A subsequent erect abdominal X‑ray, following oral administration of a contrast agent showed no significant abnormalities (Figure 1D). The hepatic flexure of the colon was beneath the elevated right hemidiaphragm, which was consistent with the diagnostic criteria for CHS (Figure 1A–1C). No pathologic changes in the mucosa were found on colonoscopy. The patient was referred for laparoscopic right hemicolectomy. However, after being informed about potential risks and benefits of the surgery, he refused the treatment and was discharged from the hospital on his request.
The Chilaiditi sign is a radiographic phenomenon characterized by interposition of a segment of the large or small intestine between the liver and the diaphragm. It was first described by Antoine Beclere in 1899, but it was characterized in detail and officially documented by Demetrius Chilaiditi, a radiologist, in 1910.
This anatomical anomaly is clinically referred to as CHS if accompanied by gastrointestinal symptoms.1 CHS arises from structural variations that result in an abnormal positioning of the colon. Various etiologic factors can contribute to CHS, including congenital malpositions, functional disorders, such as chronic constipation leading to elongation and redundancy of the colon, colonic distension, reduced liver size due to cirrhosis or hepatectomy, ascites resulting from heightened intra‑abdominal pressure, significant weight loss in obese individuals, and abnormalities, such as an elevated diaphragm or diaphragmatic paralysis.1
Clinical manifestations of CHS include abdominal pain, anorexia, constipation, flatulence, changes in bowel habits, vomiting, nausea, and, occasionally, respiratory distress. Some patients may experience cardiac symptoms, such as chest pain resembling angina and arrhythmias. These symptoms can easily be confused with those of other internal diseases.1
In this particular case, CHS may have been induced by diaphragm paralysis. Up to 2023, only 3 cases of CHS with concomitant diaphragmatic paralysis have been reported in the literature.2,3 Interestingly, there is also a documented case of an individual with CHS and bilateral diaphragmatic paralysis.3 The causes of diaphragmatic paralysis vary and include iatrogenic factors. Unilateral diaphragm paralysis due to phrenic nerve palsy is associated with multiple conditions, such as multiple sclerosis, cervical spinal cord injury, tumor infiltration, motor neuron disease, and idiopathic origins. Additionally, several infectious agents, including HIV, poliovirus, West Nile virus, and dengue virus, have been reported to cause diaphragmatic dysfunction.4
Of note, only 2 cases of CHS have been reported in Poland. Considering the rarity of CHS and its potential for diagnostic confusion with other diseases, it is crucial to provide comprehensive descriptions of adhesive CHS cases. The limited documentation of this syndrome in medical databases underscores the importance of detailed case reports to enhance understanding and recognition of CHS in clinical practice.
- Kumar A, Mehta D. Chilaiditi syndrome. In: StatPearls. Treasure Island (FL): Stat Pearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK554565/. Accessed June 2024.
- Saha BK, Bonnier A. Chilaiditi syndrome secondary to hepatic migration in a patient with bilateral diaphragmatic palsy. Am J Med Sci. 2020; 360: 79‑80. | Crossref
- Tamam M, Tamam C, Yldrm D. Extracardiac uptake on myocardial perfusion imaging in a patient with diaphragmatic paralysis and Chilaiditi’s sign. Clin Nucl Med. 2010; 35: 295‑297. | Crossref
- Huh S, Chung JH, Kwon HJ, Ko HY. Unilateral diaphragm paralysis associated with neurosyphilis: a case report. Ann Rehabil Med. 2020; 44: 338‑341. | Crossref
ARTICLE INFORMATION