Introduction
Despite the generally accepted concept that obesity is a life‑threatening disease, its incidence is still alarmingly high.1 Pathophysiology of this widespread condition is complex; nonetheless, it is considered to be a chronic inflammation leading to severe complications, especially cardiovascular diseases and diabetes mellitus.2,3 For this reason, an effective method of treating the disease has been sought for years. One of such methods, showing extraordinary effectiveness in reducing obesity‑associated complications and mortality,4 is bariatric treatment, which involves surgical intervention in the gastrointestinal tract.
Like any surgical procedure, weight‑loss surgery carries a risk of acute and chronic complications. What is thought‑provoking from both a clinical and pathophysiologic point of view is its relationship with the degree of inflammation. Nowadays, the severity of inflammation may be assessed using the neutrophil‑to‑lymphocyte ratio (NLR), a parameter easily calculated from a complete blood count (CBC). NLR is a widely‑accepted sensitive and predictive indicator of proinflammatory stage in surgical patients.5 It found particular clinical application during the recent COVID‑19 pandemic, when it was used primarily to assess severity of the disease.6 However, the relationship between NLR and bariatric surgery remains fragmented. The association between NLR, bariatric surgery, and COVID‑19 in obese patients is also unknown.
This study aimed to assess the dynamics of NLR changes in patients undergoing laparoscopic sleeve gastrectomy (LSG) in the context of previous SARS‑CoV‑2 infection. Considering that NLR is a deeply‑rooted indicator of the course of inflammation, such a study seems justified and fills the gap in understanding the relationship between LSG, COVID‑19, and inflammation.
Patients and methods
Briefly, consecutive patients eligible for bariatric surgery (individuals with morbid obesity [body mass index, BMI ≥40 kg/m2) or with BMI ≥35 kg/m2 and comorbidities, following Polish guidelines7) treated at the Department of General, Gastroenterological, and Oncological Surgery, Collegium Medicum of the Nicolaus Copernicus University (Toruń, Poland) in 2022 and 2023 were included in the study. Following dietary and psychological preparation, all patients underwent a single‑stage LSG. As part of routine medical care, each patient had a CBC performed at the central hospital laboratory 1 day before and 1 day after surgery, based on which NLR was calculated. Serum high‑sensitivity C‑reactive protein (hs‑CRP) levels were measured in each patient at the same time points. The analysis also took into account previous SARS‑CoV‑2 infections occurring within 6 months before the procedure, confirmed by the polymerase chain reaction test. Based on the results, the patients were divided into 2 subgroups, COVID‑19(+) and COVID‑19(–).
All study participants provided informed consent. The study was approved by the institutional ethics committee (KB 82/2021).
Statistical analysis
All calculations were performed using Statistica software, version 13.4 (Dell Computer Corporation, Round Rock, Texas, United States). Categorical variables were compared with the Pearson χ2 test and are reported as numbers and percentages. For appropriate comparison of continuous variables (reported as median and interquartile range [IQR]), the Mann–Whitney test and the Wilcoxon signed‑rank test were used. We used nonparametric correlations (Spearman correlation coefficient) to test for correlations between NLR and the hs‑CRP level. Differences were considered significant if the corresponding P values were below 0.05.
Results
A total of 41 patients (18 men) were included in the study. The age range of the participants was 20 to 59 years (median [IQR], 40 [11] years), and the median BMI (IQR) was 42.3 (7.8) kg/m2. The most frequent comorbidity was hypertension (n = 13). Eighteen patients (44%) had SARS‑CoV‑2 infection up to 6 months before LSG. Most patients (n = 32) were vaccinated against COVID‑19 before surgery.
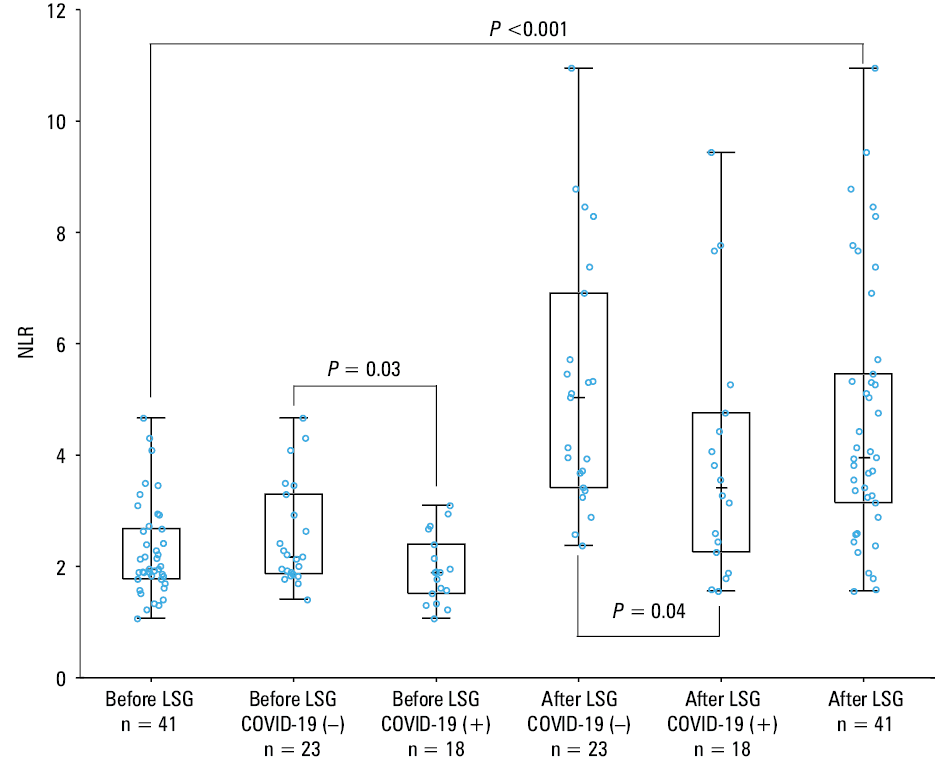
First, we checked the dynamics of NLR changes before and after LSG. We found a significant increase in NLR after surgery (median [IQR], 1.96 [0.9] vs 3.96 [2.32], respectively; P <0.001) (Figure 1). An intriguing observation has emerged regarding the connection between NLR, previous COVID‑19, and LSG. Before surgery, NLR was significantly lower in the COVID‑19(+) patients than in the COVID(–) group (median [IQR], 1.9 [0.88] vs 2.18 [1.43], respectively; P = 0.03) (Figure 1). A similar observation was made after LSG, whereby the patients with prior infection had lower NLR, as compared with those without infection (median [IQR], 3.42 [2.5] vs 5.04 [3.49], respectively; P = 0.04) (Figure 1). There were no differences in pre- and postoperative NLR between the groups of vaccinated and unvaccinated LSG patients (median [IQR], 1.95 [0.97] vs 2.14 [0.5]; P = 0.61 and 4.01 [3.19] vs 3.96 [2.31]; P = 0.86, respectively). As expected, we observed a significant increase in hs‑CRP levels postsurgery, as compared with the levels before the procedure, both in the entire study population (median [IQR], 11.5 [8.9] mg/l vs 3.51 [5.89] mg/l; P <0.001) and in the subgroups (COVID‑19[+]: median [IQR], 10.66 [21.78] mg/l vs 2.65 [8.71] mg/l; P <0.001; COVID‑19[–]: median [IQR], 11.62 [5.29] mg/l vs 4.25 [4.49] mg/l; P <0.001). However, we found no significant correlations between NLR and hs‑CRP, which may be due to a small sample size.
Discussion
Our current pilot study showed that obese patients after bariatric surgery are exposed to an enhanced proinflammatory response, as expressed by increased NLR. We also made a unique observation that a potential association between the inflammatory response and previous COVID‑19 in patients undergoing LSG may exist. Somewhat surprisingly, the COVID‑19(+) patients had a lower NLR, which may suggest a modified immune response after infection.
The first of our observations may not seem notably groundbreaking, as it is well known that surgical intervention is associated with increased inflammation. Nevertheless, our results confirm this phenomenon and indirectly suggest the clinical utility of NLR in assessing the severity of inflammation in patients after LSG. Previous studies examined NLR in LSG patients in a relatively long‑term postoperative period, at least 3 months after surgery.8,9 We focused on the pre- and short‑term postoperative values of NLR; however, this indicator in later periods may provide clinically significant information on the relationship between NLR and weight loss in patients after LSG.8,9
A unique conclusion from our study, one that sheds new light on the pathophysiology of post–COVID‑19 and its relationship with bariatric surgery, is the observation that the patients with a history of SARS‑CoV‑2 infection before LSG exhibited a less intense proinflammatory response than those who did not contract the infection. To our best knowledge, this is the first study showing such a relationship. A previous work by Swanson et al10 demonstrated the safety of sleeve gastrectomy and Roux‑en‑Y gastric bypass in patients who had COVID‑19 within 2 weeks before surgery, but the authors did not focus on assessing the severity of the inflammatory response.
NLR has become extremely useful, one could say popular, during the COVID‑19 pandemic, when it was utilized to predict severity of the disease or response to treatment.11 The results of our study indicate a less intense immune response in the patients with a history of COVID‑19, both before and after surgery. This may be related to persistent dysfunctions in the immune system as a result of infection. This phenomenon, called immune exhaustion, has been described in the literature since 2020. However, it mainly affects lymphocytes and may persist long after the disease.12-14 The effect of infection on neutrophils is less known, but the latest research suggests that neutrophil dysfunction may also be observed in the course of COVID‑19.15,16 How such a phenomenon affects the functioning of this subpopulation of leukocytes remains unknown. We suggest that future studies could link NLR with the assessment of neutrophil function and outcomes in patients after LSG. This seems eminently substantial due to continuous presence of clinically notable SARS‑CoV‑2 infections and the possibility of long‑term impact of this infection on the immune system. Future research should also focus on elucidating the relationship between NLR and the CRP level. In some way, we were surprised by a lack of correlation between these parameters, both before and after LSG; however, as mentioned above, this may be related to the small size of the study group and the short postoperative follow‑up. This relationship requires further exploration, especially in specific groups of patients, such as those included in our study, although the lack of correlation between NLR and CRP has already been described in the literature.17
Our study has several important limitations, including a small number of patients and a short follow‑up period. However, it clearly showed a relationship between NLR and a history of COVID‑19 in patients undergoing LSG.
In summary, our study confirmed that in the short postoperative period, patients after LSG are exposed to an increased proinflammatory response, which was reflected by a more than 2‑fold increase in NLR after the procedure. We also showed that COVID‑19 can modulate the immune response, which remains altered after bariatric surgery. The mechanisms causing this phenomenon and its role in predicting patient outcomes following LSG remain to be determined.
- Heindel JJ, Lustig RH, Howard S, Corkey BE. Obesogens: a unifying theory for the global rise in obesity. Int J Obes (Lond). 2024; 48: 449‑460. | Crossref
- Lin X, Li H. Obesity: epidemiology, pathophysiology, and therapeutics. Front Endocrinol (Lausanne). 2021; 12: 706978. | Crossref
- Rulkiewicz A, Pilchowska I, Lisik W, et al. Prevalence of obesity and severe obesity among professionally active adult population in Poland and its strong relationship with cardiovascular co‑morbidities – POL‑O‑CARIA 2016–2020 Study. J Clin Med. 2022; 11: 3720. | Crossref
- Kim MS, Kim JY, Song YS, et al. Association of bariatric surgery with indicated and unintended outcomes: an umbrella review and meta‑analysis for risk‑benefit assessment. Obes Rev. 2024; 25: e13670. | Crossref
- Haghi SE, Khanzadeh M, Sarejloo S, et al. Systematic review of the significance of neutrophil to lymphocyte ratio in anastomotic leak after gastrointestinal surgeries. BMC Surg. 2024; 24: 15. | Crossref
ARTICLE INFORMATION