Ultrasound-assisted catheter-directed thrombolysis therapy for normotensive shock in acute pulmonary embolism

 CC BY 4.0
CC BY 4.0
Ultrasound-assisted catheter-directed thrombolysis therapy for normotensive shock in acute pulmonary embolism
Pulmonary embolism (PE) is the third most common cause of cardiovascular death after myocardial infraction and stroke.1 Risk stratification is the most important factor determining optimal management of PE patients.1,2 Accordingly, anticoagulation is the mainstay of treatment for low- to intermediate‑risk patients, while advanced therapies, such as ultrasound‑assisted catheter‑directed thrombolysis (USCDT) are reserved for patients with intermediate to high risk of PE.2,3 In the intermediate‑risk category, the choice among conservative and interventional approaches is often arbitrary, and clinical trial evidence to support the optimal approach is still lacking. Recently, the FLASH registry of patients with acute PE who underwent catheter‑based mechanical thrombectomy identified intermediate‑risk patients with normotensive shock defined as systolic blood pressure equal to or above 90 mm Hg but cardiac index (CI) equal to or below 2.2 l/min/m2.4 Normotensive shock was initially described in acute myocardial infarction patients, and associated with 43% in‑hospital mortality.5 PE intermediate‑risk patients with normotensive shock may therefore represent a unique population likely to benefit from catheter‑based therapies, as evidenced by our case.
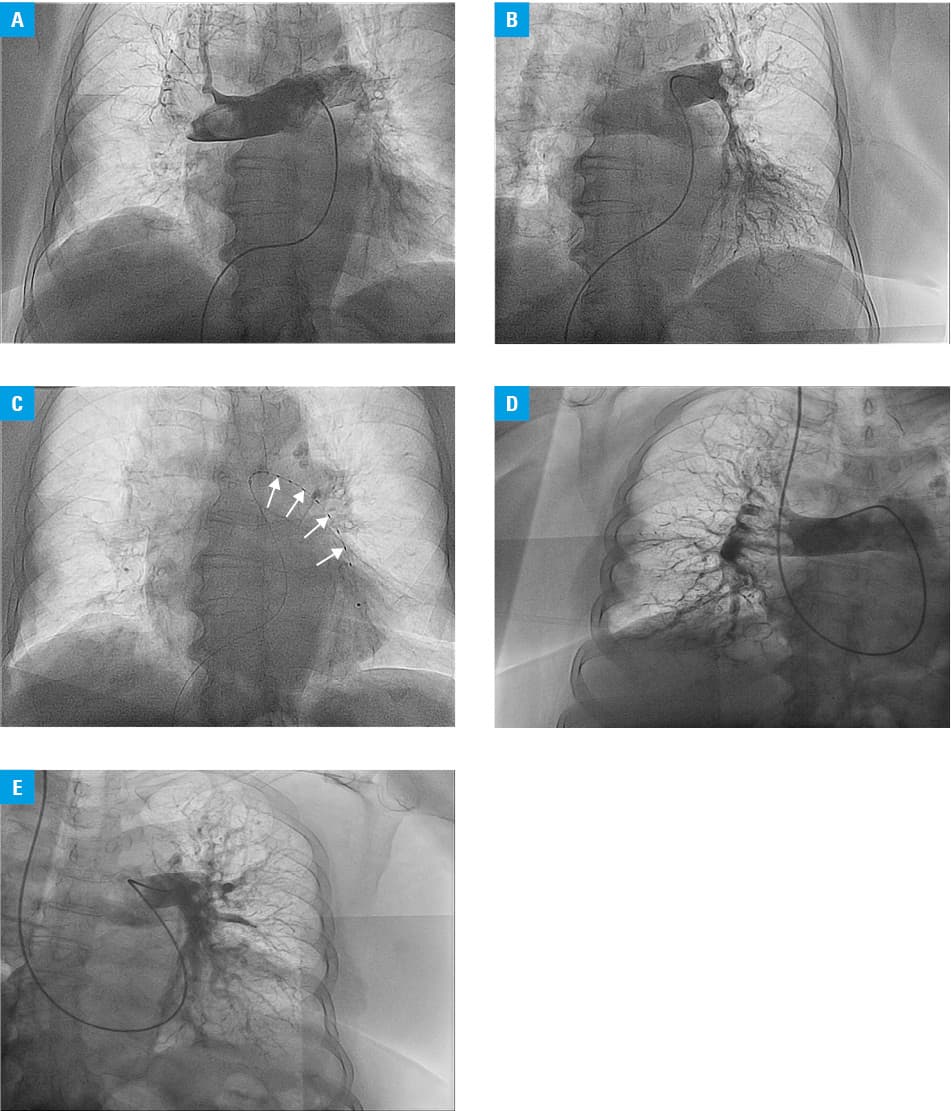
An 81‑year‑old woman with a history of type 2 diabetes mellitus, arterial hypertension, and left knee arthroplasty 3 weeks earlier was admitted with dyspnea and progressive exercise intolerance. On examination, her blood pressure was 160/105 mm Hg, heart rate 140 bpm, respiratory rate 33 breaths/min, and SpO2 76%, while breathing 15 l O2/min via a nonrebreather face mask. Laboratory tests showed elevated troponin T (62 ng/l; reference range [RR], 0–14 ng/l), N‑terminal pro–B‑type natriuretic peptide (7255 pg/ml; RR, 0–300 pg/ml), and D‑dimer (11 591 ng/ml; RR, 0–500 ng/ml). On urgent computed tomography angiography massive, bilateral pulmonary embolism and right / left ventricular ratio above 1 was visualized. The patient was admitted to cardiac care unit with a diagnosis of acute intermediate‑high risk of PE, put on unfractionated heparin infusion and high‑flow nasal cannula on maximal setting (60 l per min with FiO2 100%). Despite conservative treatment, her clinical condition did not improve, and tachycardia, tachypnea, and SpO2 values below 90% persisted for the next 24 hours. The patient was constantly evaluated using noninvasive advanced hemodynamic monitoring (Acumen IQ sensor, HemoSphere, Edwards Lifesciences, California, United States), which indicated persistent normotensive shock confirmed by CO 3 l/min, markedly decreased CI of 1.6 l/min/m2, stroke volume (SV) 23 ml/beat, and SV index (SVI) 12 ml/beat/m2 (Supplementary material, Figure S1A). Due to an increased risk of bleeding, a local PE response team decided to pursue USCDT. First, bilateral pulmonary angiography was performed via right femoral vein access, which showed massive thrombotic burden (Figure 1A and 1B), and then EkoSonic Mach 4 catheter (EKOS; Boston Scientific, Massachusetts, United States) of 135 cm (treatment zone 12 cm) was placed in the left pulmonary artery under fluoroscopic guidance (Figure 1C). Intraprocedurally, a bolus of 10 mg of alteplase was injected into the right pulmonary artery, followed by a standard bolus (2 mg) and infusion of alteplase 1 mg/h for 7 hours via the EKOS catheter. HemoSphere monitoring directly after the procedure confirmed significant increase of CO at 6.6 l/min, CI at 3.4 l/min/m2, SV at 55 ml/beat, and SVI at 29 ml/beat/m2 (Supplementary material, Figure S1B). Control pulmonary angiography was performed as per local protocol 72 hours after the procedure and showed an excellent angiographic result of the intervention (Figure 1D and 1E). Further hospitalization was uneventful.
Aging and cancer‑surviving populations will become increasingly affected by PE, and its management should be tailored to adequately address the risk of hemodynamic decompensation (crucial role of hemodynamic monitoring to detect normotensive shock), and to lower the risk of possible therapy‑related complications.
- Kopeć G, Araszkiewicz A, Kurzyna M, et al. Role of catheter‑directed therapies in the treatment of acute pulmonary embolism. Expert opinion of the Polish PERT Initiative, Working Group on Pulmonary Circulation, Association of Cardiovascular Interventions, and Association of Intensive Cardiac Care of the Polish Cardiac Society. Kardiol Pol. 2023; 81: 423‑440. | Crossref
- Pruszczyk P, Klok FA, Kucher N, et al. Percutaneous treatment options for acute pulmonary embolism: a clinical consensus statement by the ESC Working Group on Pulmonary Circulation and Right Ventricular Function and the European Association of Percutaneous Cardiovascular Interventions. Eurointervention. 2022; 18: e623‑e638. | Crossref
- Krakowian M, Machowski M, Potępa M, et al. Rheolytic thrombectomy with local thrombolysis in a patient with COVID‑19 pneumonia and acute pulmonary embolism. Pol Arch Intern Med. 2021; 131: 292‑294. | Crossref
- Bangalore S, Horowitz J, Beam D, et al. Prevalence and predictors of cardiogenic shock in intermediate‑risk pulmonary embolism: insights from the FLASH registry. J Am Coll Cardiol Intv. 2023; 16: 958‑972. | Crossref
- Menon V, Slater JN, White HD, et al. Acute myocardial infarction complicated by systemic hypoperfusion without hypotension: report of the SHOCK trial registry. Am J Med. 2000; 108: 374‑380. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION