Transarterial embolization with radiofrequency ablation as a bridge therapy in tumor-induced osteomalacia treatment

 CC BY 4.0
CC BY 4.0
Transarterial embolization with radiofrequency ablation as a bridge therapy in tumor-induced osteomalacia treatment
Tumor‑induced osteomalacia (TIO) is a rare paraneoplastic syndrome characterized by hypophosphatemia, hyperphosphaturia, and low level of 1,25‑dihydroxyvitamin D3 (1,25[OH]2D3). Its most frequent cause is a phosphaturic mesenchymal tumor (PMT), which secretes phosphatonins, primarily fibroblast growth factor 23 (FGF‑23). Symptoms of oncogenic osteomalacia include pathologic fractures, muscle weakness, bone pain, and overall exhaustion. Given the nonspecific clinical symptoms and the exceptional rarity of the tumor, its proper diagnosis and treatment may be challenging, and often take years (average time of diagnosis delay is estimated at 2.9 years).1
A 42‑year‑old man with a diagnosis of TIO was admitted to a department of endocrinology in August 2018 due to a lack of improvement of his condition after PMT surgery in May 2018.
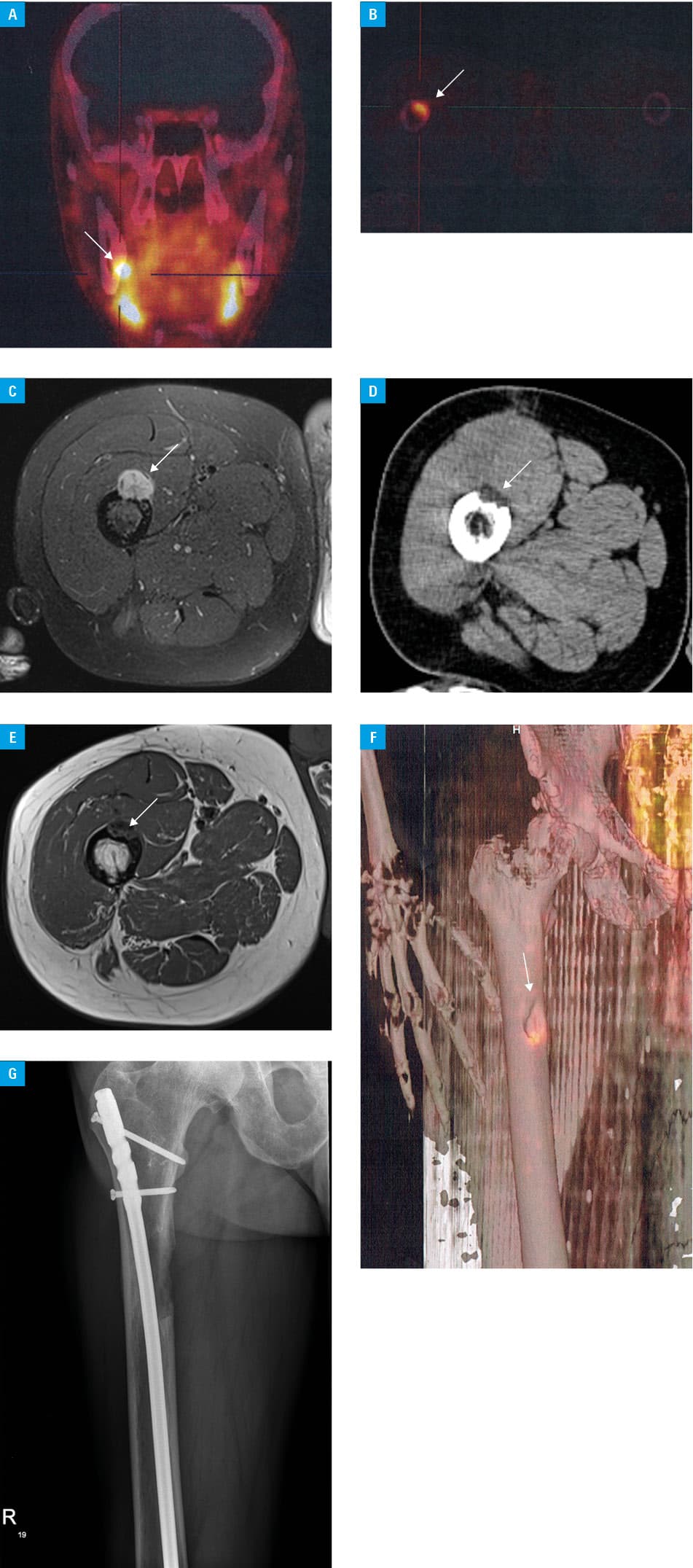
Initial symptoms of lumbar and feet pain were noticed in 2014. The patient started seeking medical advice in 2015, and after numerous outpatient visits, imaging examinations, and 4 hospitalizations, a proper diagnosis was made in March of 2018. During the diagnostic process, the patient’s condition gradually deteriorated leading to severe muscle and joint pain, waddling gait, and the use of crutches. Imaging examinations showed multiple fractures of the ribs, spinous processes, and right spatula. Laboratory tests showed hypophosphatemia at 2 mg/dl (reference range [RR], 2.5–5 mg/dl), low 1,25(OH)2D3 levels at 9.8 pg/ml (RR, 19.9–79.3 pg/ml), and high levels of alkaline phosphatase (310 U/l; RR, 38–126 U/l) and FGF‑23 (434 kRU/l; RR, 26–110 kRU/l). In order to locate the lesion, gallium‑68 DOTA‑D‑Phe1, Tyr3‑octreotate (68GaDOTA‑TATE) positron emission tomography with computed tomography (PET/CT) scan was performed, exposing 2 possible locations—the jaw or, more probably, the right femur (Figure 1A–1C). In May 2018, a surgery of the lesion in the right femur was performed with a histopathologic confirmation of PMT (Figure 1D). In the following months, the patient’s condition and laboratory tests did not improve. A second 68GaDOTA‑TATE PET/CT scan was performed, and again it showed 2 foci—in the previously operated femoral bone and in the jaw. To confirm which lesion should be removed, a simultaneous venous sampling of FGF‑23 was performed, resulting in exclusion of the lesion in the jaw. FGF‑23 levels were measured using a commercially available assay kit. Specifically, we utilized the Liaison FGF‑23 assay manufactured by DiaSorin (Saluggia, Italy). Due to the patient’s poor general condition and the surgical risk of bone fracture and healing issues, we carried out transarterial embolization (TAE) of the vessels supplying the PMT to facilitate subsequent radiofrequency ablation (RFA) of the tumor remnants (Figure 1E). In the following months, the patient’s condition significantly improved. He was able to walk without the crutches and the waddling gait disappeared. Although the FGF‑23 levels normalized, hypophosphatemia persisted. A year after RFA, a fatigue fracture of the left tibia appeared. Therefore, in July 2020, a third 68GaDOTA‑TATE PET/CT scan was performed and it showed increased expression of somatostatin receptors in the tumor’s remnants (Figure 1F). Due to unsuccessful treatment with somatostatin analogs and better general condition of the patient, we decided to surgically remove PMT remnants and use prophylactic intramedullary nailing of the femur, which resulted in normalization of phosphate levels and complete recovery (Figure 1G).
In conclusion, if the patient’s surgery risk of PMT excision is too serious, a less invasive procedure of TAE combined with RFA should be considered as a bridge therapy to definitive surgical resection or as an alternative radical therapy of PMT.
- Feng J, Jiang Y, Wang O, et al. The diagnostic dilemma of tumor induced osteomalacia: a retrospective analysis of 144 cases. Endocr J. 2017; 64: 675‑683. | Crossref
ARTICLE INFORMATION