Metastasis to the male breast from squamous cell lung carcinoma 18 months after radical surgical treatment

 CC BY 4.0
CC BY 4.0
Metastasis to the male breast from squamous cell lung carcinoma 18 months after radical surgical treatment
Breast metastases from extramammary cancer are rare, with a prevalence of 0.5%–2.7%.1 While breast cancer is significantly more common in women, men can also experience metastases to the breast from melanoma, lymphoma, or prostate cancer.2 This report discusses a rare case of a man diagnosed with breast metastasis from squamous cell carcinoma (SCC) of the lung, highlighting a distinct approach required for treating breast metastases vs primary breast cancer.
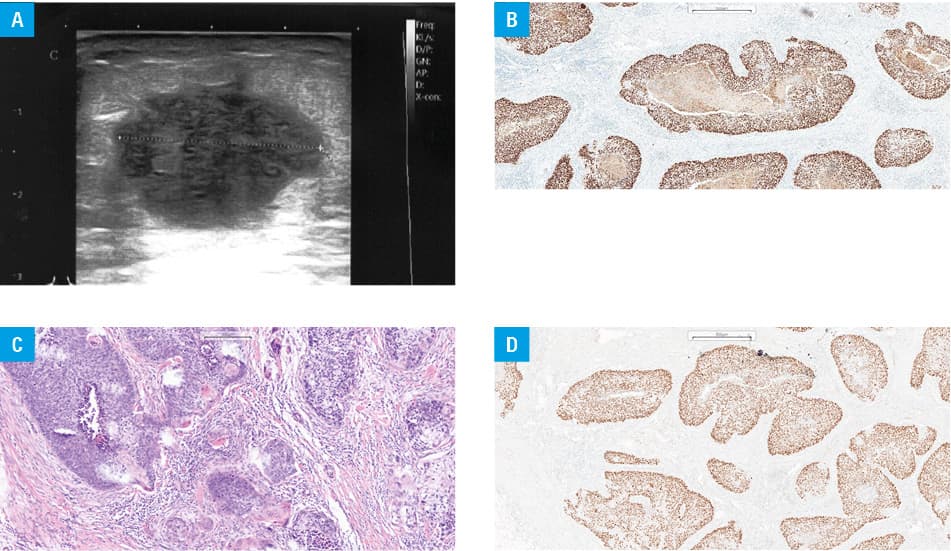
An 81‑year‑old man reported to an oncologic surgery outpatient clinic with a hard lump in his right breast he had noticed 4 weeks earlier. A well‑defined, 3 cm tumor was found in the retroareolar area of the breast without palpable local lymph nodes. Ultrasound showed an irregular hypoechoic mass (Breast Imaging Report and Data System 4C) without enlarged lymph nodes (Figure 1A). A core‑needle biopsy confirmed metastasis of lung SCC. Positron emission tomography / computed tomography (PET/CT) indicated proliferative process in the right breast, linked to previous lung cancer, with no other primary focus.
Eighteen months earlier, the patient underwent a right upper lobectomy. Postoperative histopathological results were nonkeratinizing SCC, World Health Organization / Union for International Cancer Control stage pT2a, N0, R0 resection. Follow‑up CT scans were performed 6 months and a year after surgery, and showed no signs of recurrence or features of dissemination.
On September 13, 2023, the patient underwent surgical removal of the tumor at the Department of Oncological Surgery in Katowice. Postoperative histopathological examination results showed SCC (G2) possibly corresponding to metastatic lung cancer, and focal lymphatic and vascular invasion. Total number of lymph nodes examined was 1. No node metastasis was found. The tumor was histopathologically classified as pTxN0M1; R0 resection was performed.
Early follow‑up CT scans showed no features of recurrence and tumor dissemination.
Breast cancer in men is rare, making up 0.2% of all cancers and 0.5%–1% of all breast cancer cases, with a risk estimated at 0.01%.2 Metastasis to the breast is more common in women, which is attributed to endocrine and vascular differences. Primary cancers, such as melanoma, lymphoma, and prostate cancer are typical metastasis sources in men. Lung cancer usually metastasizes to the brain, bones, liver, and adrenal glands.3 Spread of SCC to the breast is generally very rare and extremely rare in men. These metastatic lesions can rapidly grow and mimic primary breast cancer.4 Imaging studies, particularly PET/CT, play a crucial role in diagnosis but may be insufficient to distinguish metastasis from primary or benign breast conditions.5 Regardless of the differences between primary and metastatic lesions on imaging studies, core‑needle biopsy remains the primary test to confirm the diagnosis. Breast metastases show features that are not histologically specific and require, as in our case, a series of immunohistochemical studies to confirm the diagnosis (Figure 1B–1D).
This case highlights an incredibly rare occurrence of breast metastasis from SCC in a man previously treated for lung cancer. It underscores the importance of considering metastatic cancer in differential diagnosis for male breast lesions.
- Wojciechowska U, Barańska K, Miklewska M, Didkowska JA. Cancer incidence and mortality in Poland in 2020. NOWOTWORY J Oncol. 2023; 73: 129‑145. | Crossref
- Feder JM, de Paredes ES, Hogge JP, Wilken JJ. Unusual breast lesions: radiologic‑pathologic correlation. Radiographics. 1999; 19: 11‑26. | Crossref
- Noguera J, Martínez‑Miravete P, Idoate F, et al. Metastases to the breast: a review of 33 cases. Australas Radiol. 2007; 51: 133‑138. | Crossref
- Klingen TA, Klaasen H, Aas H, et al. Secondary breast cancer: a 5‑year population‑based study with review of the literature. APMIS. 2009; 117: 762‑767. | Crossref
- Yeh CN, Lin CH, Chen MF. Clinical and ultrasonographic characteristics of breast metastases from extramammary malignancies. Am Surg. 2004; 70: 287‑290. | Crossref
ARTICLE INFORMATION