Renal arteriovenous fistulas (RAVFs) are abnormal direct communications between arteries and veins in the kidney. They can be classified as congenital, acquired or idiopathic, with an overall prevalence of less than 0.04%.1 RAVFs may cause several symptoms, including high‑output congestive heart failure, hypertension, pain, abdominal bruit, and hematuria. While endovascular approach is the mainstay of RAVF treatment, the use of large and high‑output shunts can be challenging due to the possibility of incomplete occlusion and nontarget embolization, when the embolic agents can migrate into the venous circulation and from there, into the lungs. Given the possibility of growth and serious cardiovascular complications, RAVFs warrant treatment.2,3
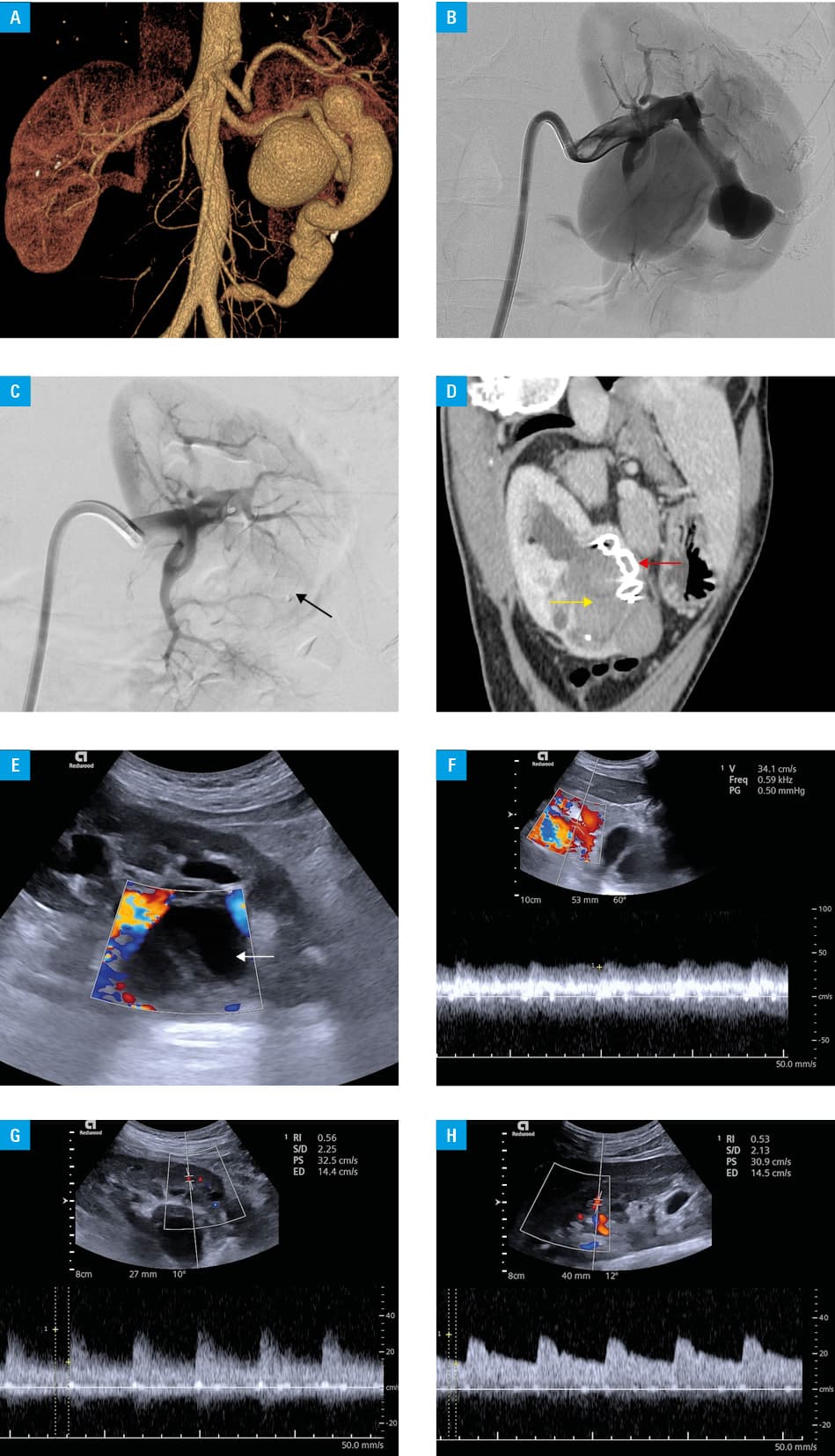
A 36‑year‑old man presented with left hydronephrosis and enlargement of the left renal vein of up to 50 mm × 54 mm in diameter, visible on a follow‑up ultrasound image. Periodic pain in his left flank was attributed to the history of lithiasis. Laboratory workup showed microhematuria and leukocyturia. Renal function was normal (serum creatinine, 68.95 μmol/l; estimated glomerular filtration rate, 116 ml/min/1.73 m2). However, renal scintigraphy showed decreased function of the left kidney (41%). The patient had a history of untreated grade I hypertension. A month before the admission, he experienced an episode of chest pain, and electrocardiography showed a right bundle branch block with no signs of heart hypertrophy. Computed tomography angiography (CTA) showed Yakes type I, direct high‑flow RAVF, consisting of dilated renal artery (RA) shunting into aneurysmally dilated renal vein with a diameter of 5.5 cm (Figure 1A). Hydronephrosis resulted from venous pelvicalyceal compression. Based on the characteristic imaging and no prior history of renal trauma, a diagnosis of congenital left RAVF was established. The patient was admitted to our hospital and was qualified for embolization. The Amplatzer Vascular Plug II (AVP) 16 mm × 22 mm (Abbott Medical, Plymouth, Minnesota, United States) was deployed via percutaneous common right femoral access. The AVP occluded both the fistulous RAs and a small saccular aneurysm within it. Digital subtraction angiography confirmed successful embolization, while maintaining flow to the remaining renal branches (Figure 1B and 1C). The patient developed postembolization syndrome, characterized by pain and fever, which resolved spontaneously. On follow‑up (immediately after the procedure, 2 weeks later, and 3 months later), the patient renal function was not impaired and blood pressure was normal. CTA and Doppler ultrasound showed complete occlusion of the fistula and no recanalization (Figure 1D–1H).
Congenital RAVFs are rare, accounting for 25% of all RAVFs.3 If present, the symptoms are nonspecific and clinically resemble those of other, more prevalent kidney diseases, such as tumors, aneurysms, and parapelvic cysts. Therefore, a higher level of clinical awareness among treating specialists and referring physicians is required.4 Increased renin production, secondary to renal parenchymal ischemia resulting from blood shunting distal to the AVF is thought to be the cause of hypertension.5 The goal of the treatment is to maintain renal function, eliminate fistula‑related symptoms, and enhance hemodynamics. Historically, RAVFs have been managed surgically (ligation of the arterial feeder, nephrectomy or partial nephrectomy). Embolization can preserve renal function with fewer risks; therefore, it is currently the favored treatment.3,5 RAVFs are rare and often overlooked causes of hypertension, arrhythmia, and right ventricular failure. They can be safely and effectively managed by endovascular embolization, while preserving renal function.
- Luo J, Liu P. Cinematic rendering of giant renal arteriovenous fistula. Radiology. 2023; 309: e231045. | Crossref
- Campbell JE, Davis C, Defade BP, et al. Use of an amplatzer vascular plug for transcatheter embolization of a renal arteriovenous fistula. Vascular. 2009; 17: 40‑43. | Crossref
- Duc VT, Duong NQT, Phong NT, et al. Large renal arteriovenous fistula treated by embolization: a case report. Radiol Case Rep. 2021; 16: 2289‑2294. | Crossref
- Nassiri N, Dudiy Y, Carroccio A, Rosen RJ. Transarterial treatment of congenital renal arteriovenous fistulas. J Vasc Surg. 2013; 58: 1310‑1315. | Crossref
- Khorrami MH, Javadi N, Ebrahimi H, et al. Congenital renal arteriovenous fistula presenting with gross hematuria and its management. Urol Case Rep. 2021; 39: 101818. | Crossref
ARTICLE INFORMATION