Integrating point-of-care ultrasound into rheumatology practice
Key words: diagnosis, point of care, probability score, rheumatic and musculoskeletal diseases, ultrasound

 CC BY 4.0
CC BY 4.0
Integrating point-of-care ultrasound into rheumatology practice
A scenario‑based probability approach integrating point‑of‑care rheumatology ultrasound (POCRUS) into rheumatology practice has recently been proposed as a teaching methodology to encourage greater awareness of US among practicing clinicians, especially with respect to the management of overlapping clinical conditions. This article reviews the rheumatological areas where application of POCRUS substantially enhances clinical reasoning to confirm or exclude target conditions. It highlights the definitions of US‑detected pathologies in rheumatoid arthritis, spondylarthritis, gout and crystal arthritis, osteoarthritis, and polymyalgia rheumatica, and discusses the added value of POCRUS in diagnosing these conditions. Additionally, it summarizes advances in predicting giant cell arteritis with sequential application of a probability score and US, and discusses the potential role of salivary gland US in the diagnostic workup of suspected Sjögren syndrome. Other areas for POCRUS application, such as in suspected nerve entrapment, are also reviewed.
Introduction
Ultrasound (US) is an investigation tool used increasingly often to assist with clinical decision‑making in rheumatology.1 It is used primarily to identify specific inflammatory disorders related to both the musculoskeletal and vascular systems. However, it can also help exclude inflammatory mimics, such as infection, cancer, and metabolic conditions, as well noninflammatory conditions, such as osteoarthritis and chronic pain syndromes.2 Despite its long‑standing application in routine practice, there remains a lack of clarity as to how to utilize US findings in practical decision‑making.
It is important that clinicians specializing in rheumatology should understand the place of US in terms of when to request it and what potential value it adds in rheumatological practice.3 Point‑of‑care US (POCUS), as an adjunct to clinical reasoning and rapid decision‑making, is applied in acute medicine for vascular, cardiac, urological, and other emergencies.4 We have coined the term point‑of‑care rheumatology ultrasound (POCRUS) to describe its probability‑based application in rheumatology.5
POCRUS has previously been shown to be a valuable prediction tool for giant cell arteritis (GCA), with the sequential application of clinical and US assessments enabling a numerical evaluation of post‑test probability using a simple nomogram.6 The European League Against Rheumatism (EULAR) recommendations for large vessel vasculitis7 and the polymyalgia rheumatica (PMR) criteria8,9 are also based on this approach. POCRUS is guided by the pretest probability of the target condition, which, in turn, is based on standardized medical history and physical examination. It is not directed by a protocolized survey of territories, such as small or large joints, vascular beds, salivary glands, and so on. Targeted US allows for establishing the post‑test probability, that is, whether the condition is likely, unlikely, or uncertain.
POCUS is not available in all rheumatology centers. The lack of equipment and training opportunities has been recently highlighted as an important barrier to its widespread utilization,10 but we also assume that there may remain a lack of understanding of how US findings specifically integrate into diagnostic algorithms. The objective of this review is to describe principles for integrating POCRUS in day‑to‑day care in order to make this tool complementary to rheumatology practice. It covers the following aspects: 1) basic definitions of US‑detected pathologies in rheumatoid arthritis (RA); 2) added value of US toward diagnosing RA; 3) US in spondyloarthritis (SpA); 4) added value of US toward diagnosing psoriatic arthritis (PsA); 5) US in crystal‑induced arthritis; 6) US in osteoarthritis (OA); 7) US in diagnosing GCA; 8) US in PMR; 9) US in carpal tunnel syndrome (CTS); 10) utility of salivary gland US for suspected Sjögren syndrome (SS); and 11) education and training.
Basic definitions of ultrasound‑detected pathologies in rheumatoid arthritis
First descriptions of US features of knee synovitis in RA and its response to yttrium‑90 injection come from 1978.11 Ten years later, De Flaviis et al12 described US features of synovitis, tenosynovitis, and erosion in rheumatoid hand.12 Application of power Doppler (PD) showed synovial hyperemia, which, as demonstrated in further studies, corresponded with active synovial tissue inflammation on dynamic magnetic resonance imaging (MRI) and histopathology.13-16 Semiquantitative scores of synovitis activity based on grey scale (GS)- and PDUS became popular not only for research but also in clinical practice.17,18 US proved to be more sensitive than conventional radiography in identifying erosions, as good as MRI in detecting synovitis, and more sensitive and specific than clinical examination in detecting synovitis and enthesitis.16,19-21 To ensure quality of US assessment in rheumatology, expert members of a “special interest group” within Outcome Measures in Rheumatology (OMERACT) defined US features of synovitis, tenosynovitis, and erosions.2,22
Synovitis is defined as a presence of hypoechoic synovial hypertrophy regardless of the presence of effusion or any grade of Doppler signal (Figure 1A). Clinical examination is less accurate than US, with approximately 20% of false‑positive results, while over a third are false‑negative. More than a half of patients have synovitis in more joints than detected on clinical examination.20
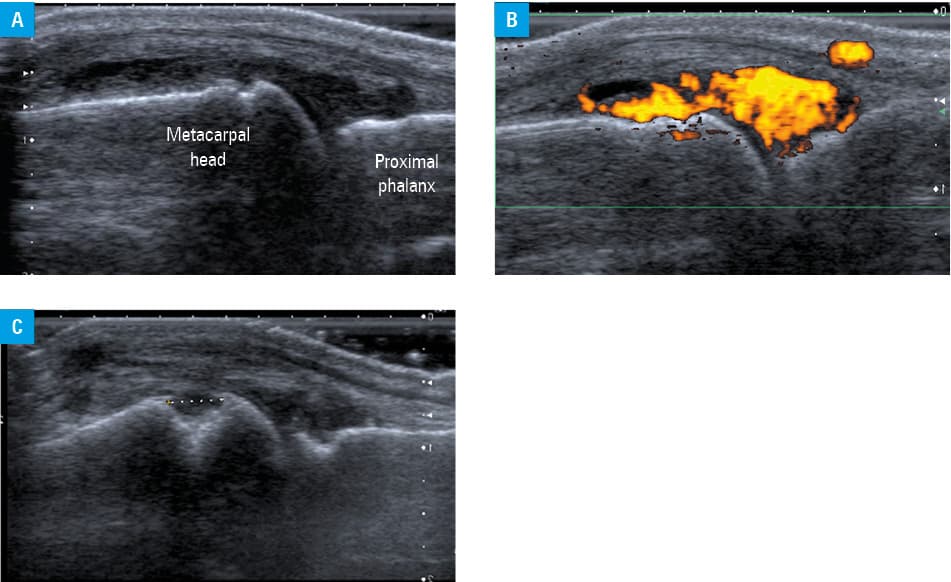
Synovial hyperemia, demonstrated as increased color Doppler (CD) or PD signal (Figure 1B), is without doubt the most useful US finding indicative of synovial inflammation. A US‑based scoring system for synovitis has been proposed based on PD signal intensity and synovial hypertrophy.17,18 The scoring system has initially been developed as an outcome measure instrument in clinical trials but is widely adopted in clinical practice. Presence of low‑grade increased vascularity in / around the joint is not exclusive to inflammatory arthritis, and can be observed following injures, in osteoarthritis, or as an incidental finding in healthy individuals, particularly those who often engage in physical exercise.23,24
Bone erosions are defined as intra- and / or extra‑articular discontinuity of bone surface visible in 2 perpendicular planes (Figure 1C). In comparison with conventional radiogram, US is 3.4‑fold and 6.5‑fold more sensitive in detecting erosions in late and early RA, respectively.19 The superior value of US is related to its ability for multiplanar assessment of bone surface, since small erosions on radiography can be obscured by the volume of bone presented on a 2‑dimensional image.19
Added value of ultrasound toward diagnosing rheumatoid arthritis
According to the 2010 American College of Rheumatology (ACR) / EULAR classification criteria for RA,25 confirmed presence of synovitis in at least 1 joint and absence of an alternative diagnosis that would better explain the synovitis are consistent with a diagnosis of undifferentiated inflammatory arthritis. Additional criteria are required to classify arthritis as RA. Each criterion is given a numerical value that contributes to the total score to classify a patient as having RA. Classification criteria scores can be regarded in clinical practice as probability scores for RA. Small joint involvement, presence of rheumatoid factor (RF) or anti–cyclic citrullinated peptide antibodies, elevated levels of inflammatory markers, and longer duration of symptoms all increase the total score received for classification criteria computation and, consequently, the probability of RA (Supplementary material, Table S1). Patients with a total score of 6/10 and above are at a high risk of RA and should be treated as such. Between 87% and 97% of patients with a high probability of RA require treatment with methotrexate within 1 year.
Nakagomi et al26 evaluated the additional value of US in relation to the ACR/EULAR RA classification criteria. A total of 109 patients with possible RA defined as the presence of musculoskeletal symptoms lasting up to 3 years and swelling or tenderness of joints were included. The patients underwent US examination of 38 joints at the baseline. Synovitis was defined by 2 levels of intensity: group A, GS synovial hypertrophy of 1 or greater, and group B, GS synovial hypertrophy of 2 or greater and a presence of PD signal greater than or equal to 1. The primary outcome was a percentage of patients who required treatment with methotrexate at 1 year. The authors found that the patients who did not have clinical and US‑detected synovitis at the baseline required treatment with methotrexate in less than 20% of cases. The patients who had clinical synovitis at the baseline and synovitis on US required treatment in 80% of cases. The findings were particularly interesting among the patients in whom clinical examination and US results were discordant. The participants who did not present with clinical synovitis but had synovitis on US, either GS- or CDUS, at the baseline, required treatment within a year in 60% and 80% of cases, respectively.
The performance of the ACR/EULAR RA classification criteria for clinical synovitis in comparison with US‑detected synovitis for all patients was not significantly lower. However, in patients with a score of 3/10 to 7/10, US performed almost 2‑fold better than clinical examination (area under the curve [AUC] of 0.457 vs 0.8, respectively) (Supplementary material, Figure S1). The difference between AUC values for clinical examination and US reflects the additional value of US in diagnostically uncertain cases.
Thus, US can enhance the pretest probability determined based on the ACR/EULAR classification criteria by confirming / excluding synovitis, and hence by influencing the total score of involved joints (as a method more sensitive than clinical examination in detecting synovitic joints). It can also point toward an alternative diagnosis by revealing elementary lesions associated with other types of inflammatory arthropathies, such as crystal deposits in crystal arthropathies, or enthesitis, which is a key feature of SpA.
This points toward the need of a reasoning process that has to be applied before using US. The risk of a target diagnosis or pretest probability should be estimated based on clinical and laboratory data before a US examination is performed. As a test, US leads to a more specific post‑test diagnosis, evaluating a condition as likely, unlikely, or uncertain. This process is not different from any other diagnostic process in medicine. POCRUS requires that the operator be informed of the basic pretest probability of the target rheumatological condition.
Ultrasound in spondyloarthritis
Enthesitis is a hallmark feature of SpA.27 On US, enthesitis is defined as a hypoechoic and thickened insertion of the enthesis that exhibits Doppler signal if active, and that may show erosions and enthesophytes as signs of structural damage (Figure 2A–2D).2,28 Similarly as in the case of synovitis, US is superior to clinical examination in detecting enthesis. According to Balint at al,21 as compared with US, sensitivity of clinical examination for the detection of lower limb enthesitis was low, at 22.6%, and specificity was moderate, at 79.7%.21
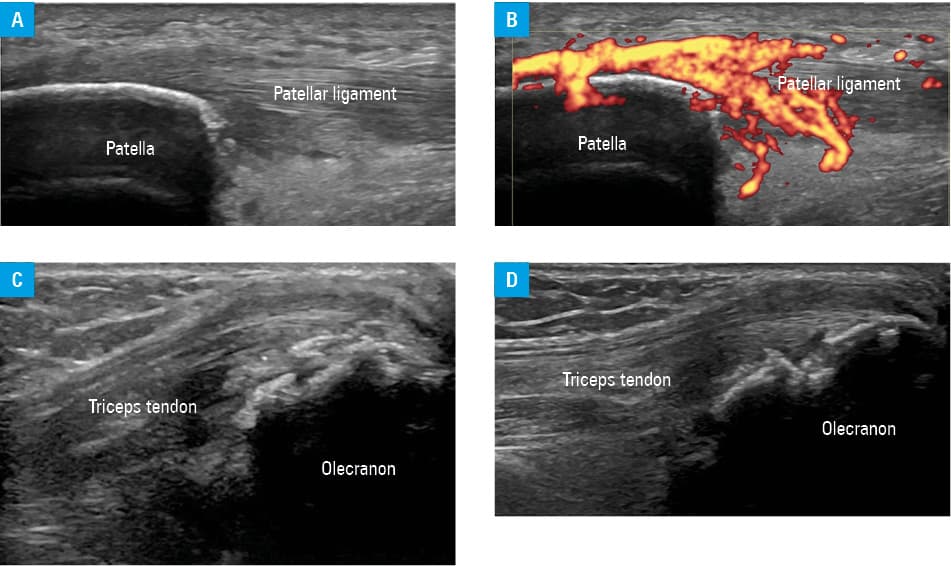
It may not be possible to distinguish between mechanical and inflammatory causes of enthesitis.29,30 Enthesitis can be seen in athletes, volleyball players, and other physically active individuals. Typical locations of mechanical enthesitis include the common extensor origin at the lateral epicondyle (tennis elbow), common flexor origin at the medial epicondyle (golfer’s elbow), patellar ligament (jumper’s knee), and Achilles tendon. Signs of severe inflammation, such as increased PD signal, erosive lesions, and multiple entheseal involvement in individuals who are not physically active can support the diagnosis of SpA. Additional data to support the diagnosis include predisposing features, such as psoriasis (PsO), inflammatory bowel disease, anterior uveitis, or positivity for human leukocyte antigen (HLA)class I molecule B27.
Added value of ultrasound toward diagnosing psoriatic arthritis
Classification criteria for PsA (CASPAR)31 are based on a presence of inflammatory articular disease and require more than 2 additional criteria out of 5 categories: presence of dactylitis, current or past PsO, family history of PsO in a first- or second‑degree relative, psoriatic nail disease, negative RF, and presence of juxta‑articular new bone formation on radiography (Supplementary material, Table S2).31 These classification criteria can be used as a probability score for PsA in rheumatology practice.
In PsA, enthesitis can affect small structures, such as collateral ligaments of the proximal interphalangeal joints and central slip insertion to the base of a middle phalanx (Figure 3A and 3B). Enthesitis affecting small structures of hand joints or the nail bed, and associated with an increased Doppler signal, capsular enthesophytes, pulley involvement, or juxta‑articular periosteal reaction, are findings typical of PsA (Figure 3C and 3D).32-34 Peritendon inflammation of the extensor digitorum tendon over the metacarpophalangeal joint is considered a form of enthesitis. POCRUS patterns of these findings substantially contribute to a post‑test probability of PsA.35 None of the abovementioned findings can be ascertained through clinical examination only.
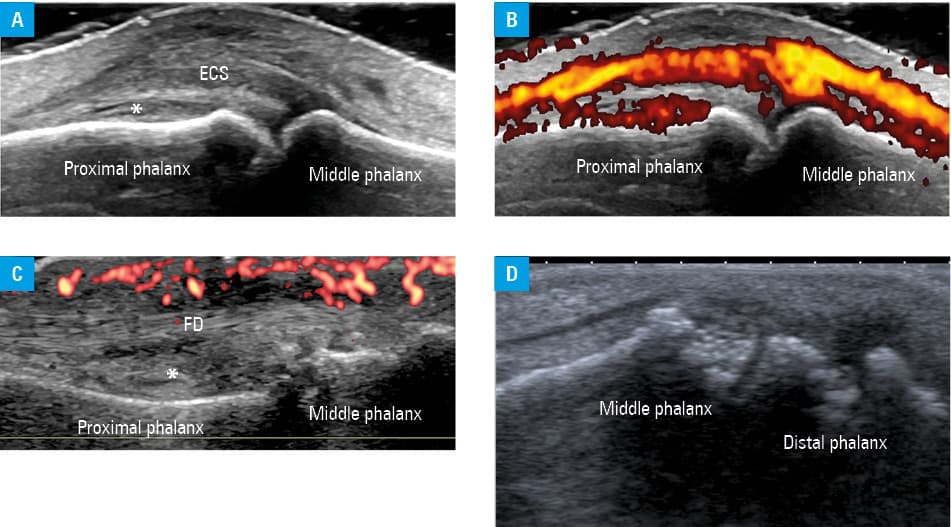
Abbreviations: ECS, extensor central slip; FD, flexor digitorum; PIPJ, proximal interphalangeal joint
As expected, US has been shown to be of additional value to CASPAR for diagnosing PsA.36 Geng et al36 tested the performance of CASPAR in 326 consecutive patients with suspected peripheral PsA. A total of 164 individuals were diagnosed with PsA and 162 with non‑PsA (PsO, osteoarthritis, fibromyalgia, seronegative RA, and undifferentiated arthritis). US was used to assess the presence of synovitis in 46 joints (bilateral elbows, wrists, small hand joints, knee, ankle, and metatarsophalangeal joints), enthesitis at 16 sites (similar as on physical examination), and tenosynovitis in 36 tendons. Tenosynovitis, enthesitis, and bone erosion on US were significantly more frequent in the PsA group than in the non‑PsA group. Tenosynovitis and enthesitis on US were identified as independent risk factors for PsA, with a value higher than that of dactylitis or new bone formation on X‑ray. The authors suggested adding US tenosynovitis and / or enthesitis to the CASPAR scoring system by offering 1 point for positive findings. The total score was increased to 7 points, and the cutoff for diagnosing PsA was increased to at least 4 points out of 7. By integrating US into the CASPAR criteria, the performance of the criteria improved, with superior specificity (91.4% vs 84%) and similar sensitivity (95.7% vs 94.5%), as compared with the original score. AUC for the original CASPAR criteria was high at 0.933, and increased with US supplementation to 0.954. Of note, the authors did not calculate the improved CASPAR score for patients with ambiguous clinical presentation, which may prove even more useful.
Ultrasound in crystal‑induced arthritis
Gout
Double contour sign, tophi, and aggregates are the elementary lesions typical of gout.37 Double contour sign is defined as a hyperechoic band over the superficial margin of the articular hyaline cartilage, independent of the angle of insolation of the ultrasound beam (Figure 4A). It represents monosodium urate (MSU) deposits on the cartilage surface. Tophus is defined as a circumscribed, inhomogeneous aggregation that may be surrounded by a small anechoic rim (Figure 4B–4D).2 Tophi may be located within the synovial tissue, tendons, ligaments, or soft tissues. Successful urate‑lowering treatment leads to resolution of MSU deposits38; however, structural damage to tendons and bone is irreversible. The value of US in detecting MSU deposits has been recognized in the 2015 ACR/EULAR classification criteria for gout.39 The relative weighting of an imaging domain category (presence of a double contour sign on US or MSU deposits on dual‑energy computed tomography) is equal to that of a presence of tophus or a serum urate level greater than or equal to 10 mg/dl (≥0.6 mmol/l) (Supplementary material, Table S3).
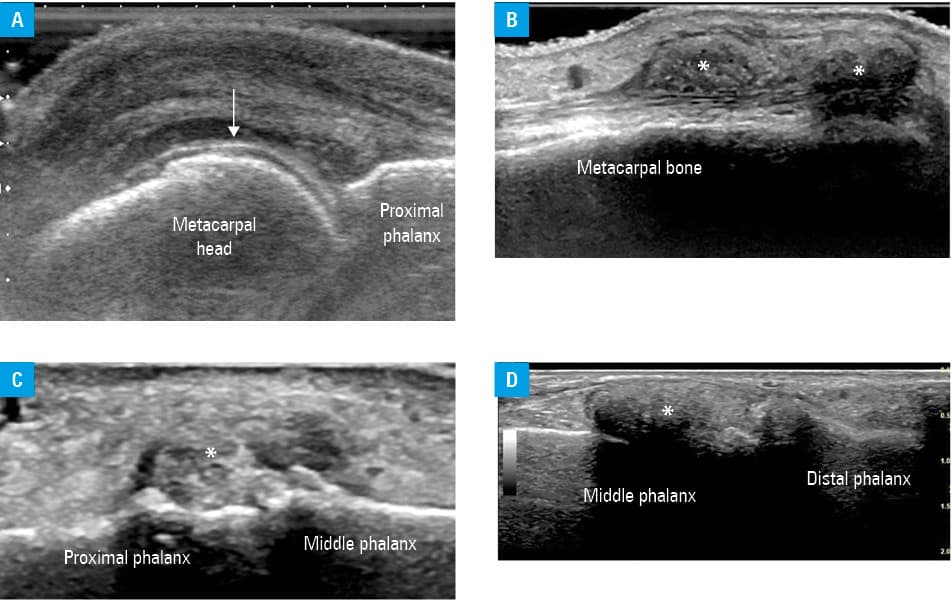
Abbreviations: IPJ, interphalangeal joint; MSU, monosodium urate; others, see Figure 3
The 2015 ACR/EULAR classification criteria for gout have sensitivity of 0.92 and specificity of 0.89. When only clinical parameters were used, without MSU evaluation or imaging data, sensitivity and specificity values of the criteria were 0.85 and 0.78 respectively.
Calcium pyrophosphate deposition disease
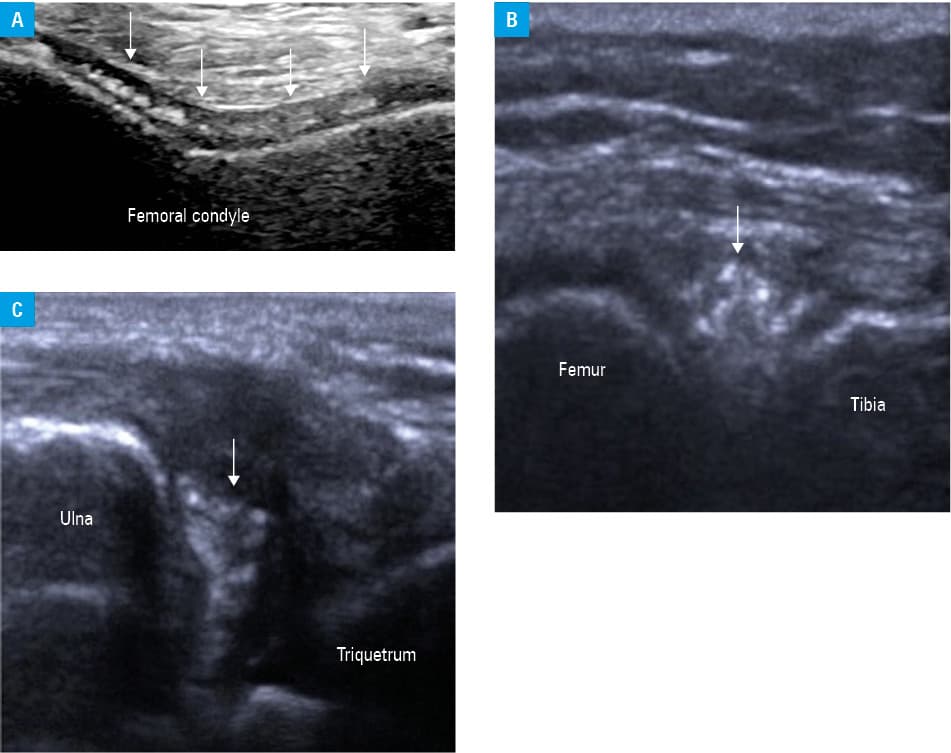
Calcium pyrophosphate deposition (CPPD) disease, acute calcium pyrophosphate crystal arthritis, chondrocalcinosis, or pseudogout are various names of the same rheumatic disease, used depending on the circumstances of the diagnosis.40 Patients presenting with a hot and swollen joint would be given the diagnosis of acute CPP crystal arthritis (previously pseudogout), while an incidental finding of joint cartilage calcifications on X‑ray is defined as chondrocalcinosis. On US, calcifications can be seen within the hyaline cartilage, but unlike in gout, they are located in the central layer of the cartilage and not on its surface (Figure 5A).41 US also shows calcifications in fibrocartilages, such as the menisci or the triangular cartilage complex (Figure 5B and 5C). With synovial fluid analysis as a reference method, US detected CPP crystals with sensitivity of 0.6 to 0.9 and specificity of 0.9 to 0.97, depending on the scanning protocol (knees, wrists, target joint). The scanning protocol comprising US of both knees and wrists had the highest diagnostic accuracy (>90%).42 In comparison with radiography, US showed superior sensitivity and specificity in detection of CPP crystals in the knees.43 US was also found more specific than synovial fluid analysis (0.96 vs 0.86).40 US is a reliable and noninvasive technique for identification of CPP crystals in hyaline- and fibrocartilages, and has been included in the 2023 ACR/EULAR classification criteria for CPPD disease (Supplementary material, Table S4).44
Calcific periarthritis
Calcific periarthritis can present as acute arthritis or can be silent and found incidentally on imaging. A typical example is calcific tendinitis of the supraspinatus tendon, but periarticular calcifications can also be found in other joints, including small joints of hands and feet.45 Acute presentation has a high rate of misdiagnosis, as it mimics infective or inflammatory process (Figure 6A–6D).46,47 US can visualize periarticular calcifications at various phases.48 In a formative phase, the calcification is compact and solid, with a strong acoustic shadow. In a resorptive phase, the calcification is soft, with faint acoustic shadow (Figure 6C). The resorptive form is often associated with an increased Doppler signal and clinically presents as acute arthritis / bursitis. Aspiration and barbotage of the lesion under US guidance are more successful at this stage, while needling may be required when the calcification is larger or of more compact structure.
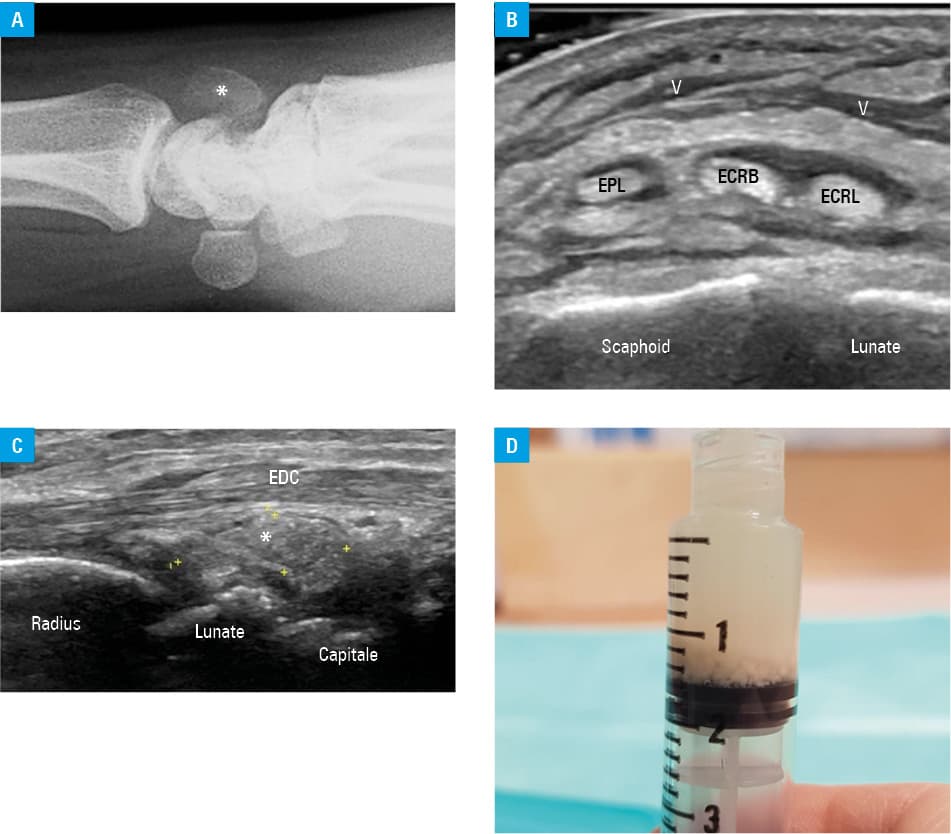
Abbreviations: ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; EDC, extensor digitorum communis; EPL, extensor pollicis longus
Ultrasound in osteoarthritis
Osteophytes are a very common finding on US examination of joints in adult patients. An osteophyte is defined as a step‑up, bony prominence at the bony margin that is visible in 2 perpendicular planes.2 OA can be associated with a PD signal at the joint capsule / collateral ligaments,25 mainly at the first carpo‑metacarpal joint, first metatarso‑phalangeal joint, and talo‑navicular joint. US examination in OA detects effusion, thickening of the collateral ligaments, hyaline cartilage defects, meniscal protrusion, erosions, and occasionally loose calcified bodies in the joint recesses.49 The major role of US is to exclude inflammatory arthritis overlapping with OA.
Ultrasound in diagnosing giant cell arteritis
Typical lesion in GCA is a halo sign.50,51 Inflammatory infiltration / remodeling of the arterial wall leads to its thickening and decreased echogenicity on US (Figure 7). In a healthy individual, the superficial temporal artery (STA) wall is thin and poorly visible on US. When the pressure is applied by the US probe, the lumen of the STA collapses and the artery disappears from view. In GCA, thickened arterial wall remains visible upon compression. The low echogenicity of the arterial wall makes it difficult to distinguish it from the vessel lumen. When CD is used, the signal reveals flow in the artery, and the surrounding hypoechoic wall appears as a rim or a halo around the vessel lumen.
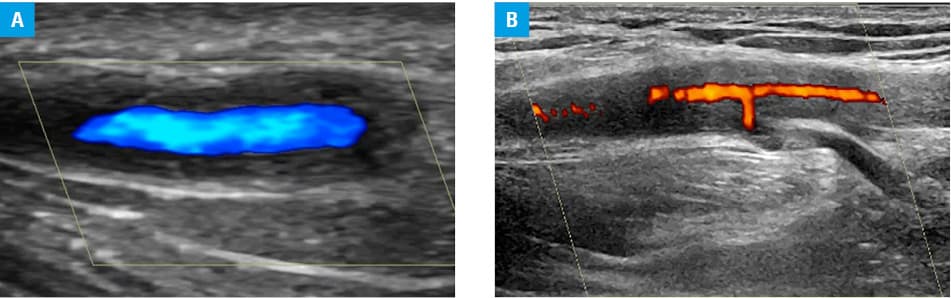
Thickening of the arterial wall can be seen not only at the STA but also at its frontal and parietal branches, facial, occipital, vertebral, carotid, subclavian, and axillary arteries, and other sites. An 8‑vessel scan comprising a bilateral assessment of the temporal arteries, terminal branches, and axillary arteries is recommended by the EULAR as an imaging method to confirm a diagnosis of GCA, and it is now the imaging modality of first choice for a diagnosis of suspected GCA and large vessel vasculitis.50 Less common findings in GCA are luminal stenosis and occlusion, but these lesions are technically more difficult to elicit and hence harder to ascertain.50
The pretest probability of GCA in a fast‑track clinic can be assessed by the well‑validated Southend GCA probability score (SGCAPS) (Supplementary material, Figure S2).52,53 It categorizes patients into high- (>12), intermediate- (9–12), and low‑risk groups (<9). A subsequent 8‑vessel scan (assessing the halo count, halo score, and OMERACT US score) can be used to establish the post‑test probability of GCA as likely, unlikely, or uncertain.54-56 Further data from a multicenter, prospective, longitudinal HAS GCA study6 have shown that the sequential application of SGCAPS and halo count (the number of scanned arterial segments that exhibit a sensitive halo sign) enables calculation of the HAS‑GCA score—a numerical and objective estimation of post‑test probability that can be performed using a simple nomogram.6 This report strongly validates the POCRUS approach.
Ultrasound for polymyalgia rheumatica
Early studies identified shoulder bursitis, gleno‑humeral synovitis, biceps tenosynovitis, hip synovitis, and hip bursitis as lesions frequently identified on US in patients with PMR.57 Accordingly, the 2012 EULAR/ACR provisional classification criteria for PMR incorporated these US lesions into the criteria.8 This improvement was ground‑breaking; however, the prevalence of most of these synovial lesions was not significantly different between patients with PMR and controls with RA,8 suggesting that such US lesions are not specific to PMR.
On the other hand, studies using 18F‑fluorodeoxyglucose positron emission tomography / computed tomography (18F‑FDG PET/CT) showed that inflammatory changes in the ischial tuberosity, greater trochanter, and spinous process are specific to PMR.58,59 A study using whole‑body MRI demonstrated that extracapsular lesions that included a wide range of anatomical structures, such as the bursa, tendon, and ligament, are more characteristic of PMR than of RA.60 More recent studies using MRI and 18F‑FDG PET/CT showed that tendons and muscles in the shoulder and hip were the anatomical structures inflamed in PMR.61,62 One of these reports was accompanied by an editorial in which it was argued that the origin of inflammation in PMR is likely to be the musculotendinous junction.63
Interestingly, data from a recent study from Japan support the notion that inflammation of the tendon and ligament is characteristic of PMR.9 In that study, the locations of inflammation in the shoulder and knee were compared between PMR, PMR‑mimic, and RA, using Doppler US. As a result, biceps tenosynovitis (Supplementary material, Figure S3A and S3B), supraspinatus / subscapularis tendinitis (Supplementary material, Figure S3C and S3D), knee collateral ligament inflammation, and popliteal tenosynovitis (Supplementary material, Figure S3E) were the lesions that discriminated PMR from the other conditions. Importantly, the authors demonstrated that incorporating these findings into the 2012 EULAR/ACR provisional classification criteria for PMR substantially increased their diagnostic accuracy (Supplementary material, Figure S4A and S4B). Although these data need to be validated in an independent cohort, this study indicates that the POCRUS approach can be applied to PMR as well, with the classification criteria used as the pretest probability score.
Clinical vs ultrasound diagnosis of carpal tunnel syndrome
There are no uniform diagnostic criteria for CTS.64 The diagnosis is based on a patient’s history, clinical examination, and additional tests, including nerve conduction studies (NCSs; considered the gold standard) and / or imaging data. Reliability of the clinical examination with reference to NCS varies depending of the selected test.65 Approximately 50% of patients with a clinical suspicion of CTS have positive NCS results. US is a noninvasive method used for assessment of the median nerve entrapment in CTS.66,67 Compression within the carpal tunnel results in characteristic changes to the nerve thickness and echostructure: swelling at the entrance to and exit from the carpal tunnel and flattening within (hourglass shape). The nerve loses its honeycomb echo structure and its echogenicity is decreased, while the epineurium appears thick and bright. Measurement of the cross‑sectional area (CSA) of the median nerve at the entrance to the carpal tunnel corresponds to the grade of compression measured in NCSs.66 Although there is a variation in normal values of median nerve CSA across different studies, a value of 10 mm2 or less is considered normal, while a value exceeding 15 mm2 indicates significant compression.67 Pooled analysis showed that US had sensitivity of 77.6% and specificity of 86.8% for diagnosing CTS.68
Salivary gland ultrasound for suspected Sjögren syndrome
The salivary glands, including the parotid and submandibular glands, are commonly affected in SS. In a scenario of suspected SS, bilateral parotid and submandibular gland US allows for their direct visualization to assess homogeneity, echogenicity, gland posterior borders, number and size of focal lesions, blood flow, lymph nodes, and calcification.69,70 This can facilitate detection of active inflammation and vascular changes associated with sialadenitis and SS.
Traditionally, the diagnosis of SS has been based on clinical evaluation, antibody level measurement, and minor salivary gland biopsy (MSGB). MSGB is considered the gold standard; however, it is an invasive procedure with limited availability, requiring histologic expertise. An Italian study involving 30 women classified as having SS by the European criteria and age- and sex‑matched controls with dry mouth, showed salivary gland US to be as accurate as the MSGB lymphocytic score.71,72
Studies in new‑onset SS have shown that salivary gland scintigraphy findings correlate with abnormal US findings, providing additional evidence that US is a good noninvasive tool to assess salivary gland function.73,74
The real value of salivary gland US is in evaluation of suspected SS in patients with sicca symptoms who are negative for anti–Sjögren syndrome A antibodies (SSA/Ro). In this aspect, a French group retrospectively analyzed 337 patients who were treated at a dry eye syndrome clinic.75 A total of 77 patients were confirmed to have SS, while 192 did not fulfil the SS classification criteria (non‑Sjögren dry eye syndrome). Abnormal findings on salivary gland US were significantly more frequent in the SS group than in the group with non‑Sjögren dry eye syndrome. The authors also reported that a US score greater than or equal to 2 had good specificity (91%) to diagnose SS. In summary, most patients with SS have abnormal findings on US of the salivary glands.
In a report by the EULAR primary SS study group,76 a negative US was shown to predict negative parotid gland biopsy, while a positive US predicted positive lip biopsy. Sensitivity and specificity of salivary gland US were 71% and 92%, respectively, as compared with the classification criteria by the American European Consensus Group. In comparison with the 2016 ACR/EULAR classification criteria, sensitivity and specificity was 77% and 92%, respectively.
In a study of 72 patients with suspected SS from a Spanish center, sensitivity and specificity of US were 90% and 67%, respectively, while biopsy had sensitivity of 76% and specificity of 90% when using the 2016 ACR/EULAR classification as the gold standard for classifying SS.77 Thus, US may play a valuable role in screening patients for suspected SS, and, if necessary, can be supplemented with biopsy of the minor salivary gland.77,78 It has been suggested that inclusion of salivary gland US can improve the sensitivity of the ACR/EULAR criteria to classify SS.79
Higher‑grade findings on salivary gland US appear to correlate with the severity of SS as measured by the EULAR SS disease activity index, and with the presence of antibodies, namely RF and anti–Sjögren syndrome B (SSB/La).80,81 The abnormal findings are also of higher grade in SS than in other connective tissue diseases.82
Characteristic abnormalities of the salivary glands include hypoechoic areas indicative of inflammation, whereas hyperechoic foci suggest fibrosis. A grading system for inhomogeneity has been developed83 and taken further by the OMERACT working group for US.84 The scoring system primarily focuses on identifying hypoechoic areas within the glands, which indicate pathological changes. Thus, a “normal parenchyma” is assigned a score of 0, whereas diffuse changes and extensive inhomogeneity, with the presence of hypoechoic or anechoic areas occupying the entire glandular surface, are assigned a score of 3 (Figure 8A–8D). Scores 1 and 2 represent mild and moderate involvement, respectively. A higher score increases the likelihood of a SS diagnosis. The inter‑reader agreement of the scoring system is good, and the system is helpful in identifying the SS patients with an increased risk of non‑Hodgkin lymphoma of the major salivary glands.85
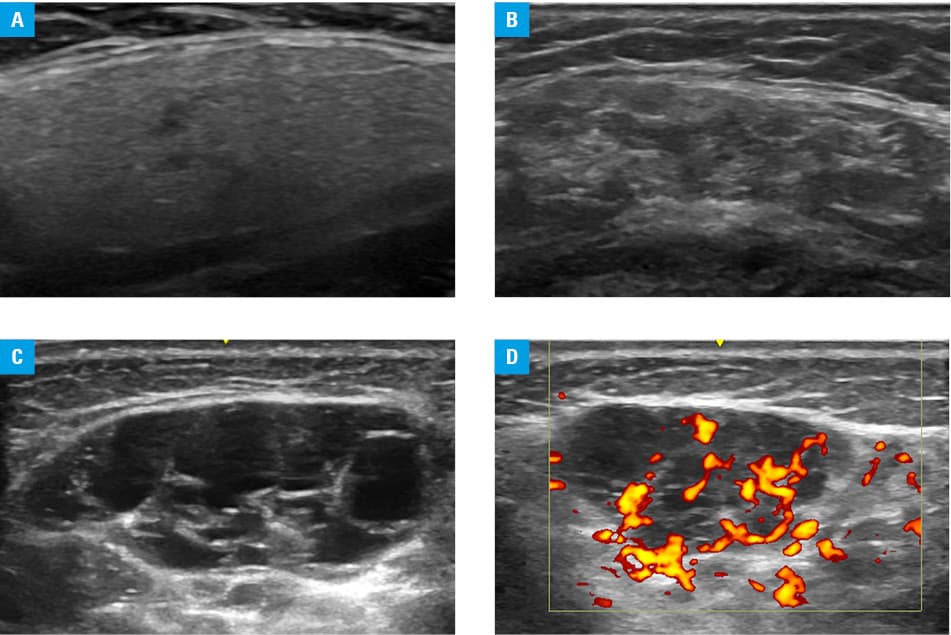
The OMERACT group has also developed a semiquantitative scoring system for vascular inflammation, graded as 0 to 3.86 Grade 0 represents an absence of vascularity, while grade 1 refers to a presence of focal vascular signals in the gland parenchyma, and grade 2 and grade 3 indicate the presence of diffuse vascular signals in less and more than 50% of the gland, respectively. These proposed grading system needs validation and reliability assessment.
Serial salivary gland US examinations can assess the response to treatment, helping clinicians tailor therapeutic interventions based on individual patient responses.87 However, some uncontrolled observational studies comparing SS and non‑SS sicca groups have found no significant change in the US score over time.88 US‑guided procedures, such as fine‑needle aspiration and / or core needle biopsy can be performed at the POC, whenever an alternate diagnosis (such as malignancy) is considered.89
POCRUS of the salivary glands is an appealing noninvasive and a readily available imaging modality that may clearly aid in early detection and real‑time monitoring of disease activity in patients with SS when performed by an experienced operator. We suggest formulation of a diagnostic algorithm involving sequential application of pretest probability assessment with the existing classification criteria (including serology) as probability scores, followed by a standardized salivary gland US assessment and scoring. This will help establish a post‑test probability of whether SS is likely, unlikely, or uncertain (when a MSGB can be undertaken). Such an approach to confirming / excluding SS in suspected cases would considerably enhance clinical practice and research on this condition.
Performing ultrasound, education, and training
It has been noted recently that in the United States, training in US remains the single most important factor associated with utilization of US in rheumatology.10 This finding is not significantly different from what was observed in the last survey performed in the United Kingdom in 2007,90 and the situation is likely similar in other countries. Whether all rheumatologists should be able to perform US themselves remains controversial; but certainly, almost all agree that US is an extremely valuable investigative tool in rheumatology in terms of decision‑making. To that end, it is important that all operators and recipients of reports be able to understand the significance of specific US findings and how they might be used in practice.
The fact that rheumatologists are able to perform scans themselves is largely a result of the many technological improvements that have occurred most notably since the mid‑1990s. Due to improved computing power and development of higher‑frequency linear transducers, greater resolution images could be achieved. In addition, redesign of machines improved their usability by nonspecialists; not only did operating platforms become more intuitive, but also machines became more compact, which allowed for using them in a number of different clinical settings, including the outpatient department, the ward, and in community settings. Portability has allowed for greater accessibility, although the smaller machines do have limitations in terms of image resolution and Doppler capabilities. Therefore, they are arguably most suited for screening and detecting more obvious pathological changes as well as for guiding interventions, while a more sophisticated machine may be required to detect more subtle changes, for example, low levels of inflammation or GCA. To this end, it is crucial that a US examination be performed with appropriate equipment and by a trained individual in order to avoid over- or undercalling of findings. It is important for the clinician (whether they perform the scan themselves or not) to acknowledge that US may not answer every question (eg, due to inaccessibility of US beam secondary to severe obesity, deeply situated structures, or complex bone anatomy), and that sometimes other imaging tools, such as MRI, may be more appropriate.
We believe that our POCRUS‑based approach to probability‑based learning can facilitate learning and practice for health professionals by providing an evidence‑based map for navigating through the decision‑making process. The use of real‑world scenarios5 further reinforces the relevance of the scans to patient management. For those performing US examinations themselves, this approach may further clarify what should be included in the imaging reports. A recent paper by Lee et al5 reported on the successful delivery of an on‑line POCRUS program to Asia Pacific League of Associations for Rheumatology members with very positive results.
Conclusions
In recent decades, US imaging has become increasingly available outside traditional radiology‑based environments. Doctors and other health professionals of various specialties now pursue US training focused on their area of interest. It is imperative that those who use US understand which imaging findings are important to look for and how to interpret them in a clinical context. This review seeks the reader to better understand the place of US in order to improve early diagnosis, reduce cost of alternative tests, and provide more tailored treatments, all of which translate into improved patient care and satisfaction.
- Mandl P, Ciechomska A, Terslev L, et al. Implementation and role of modern musculoskeletal imaging in rheumatological practice in member countries of EULAR. RMD Open. 2019; 5: e000950. | Crossref
- Bruyn GA, Iagnocco A, Naredo E, et al. OMERACT definitions for ultrasonographic pathologies and elementary lesions of rheumatic disorders 15 years on. J Rheumatol. 2019; 46: 1388‑1393. | Crossref
- Atchia I, Brown AK, Chitale S, et al. Recommendations for rheumatology ultrasound training and practice in the UK. Rheumatology (Oxford). 2021; 60: 2647‑2652. | Crossref
- Lee L, DeCara JM. Point‑of‑care ultrasound. Curr Cardiol Rep. 2020; 22: 149. | Crossref
- Lee A, Kong KO, Ikeda K, et al. Enhancing rheumatology training: the POCRUS model for integrating ultrasound into clinical practice. Int J Rheum Dis. 2024; 27: e15225. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION