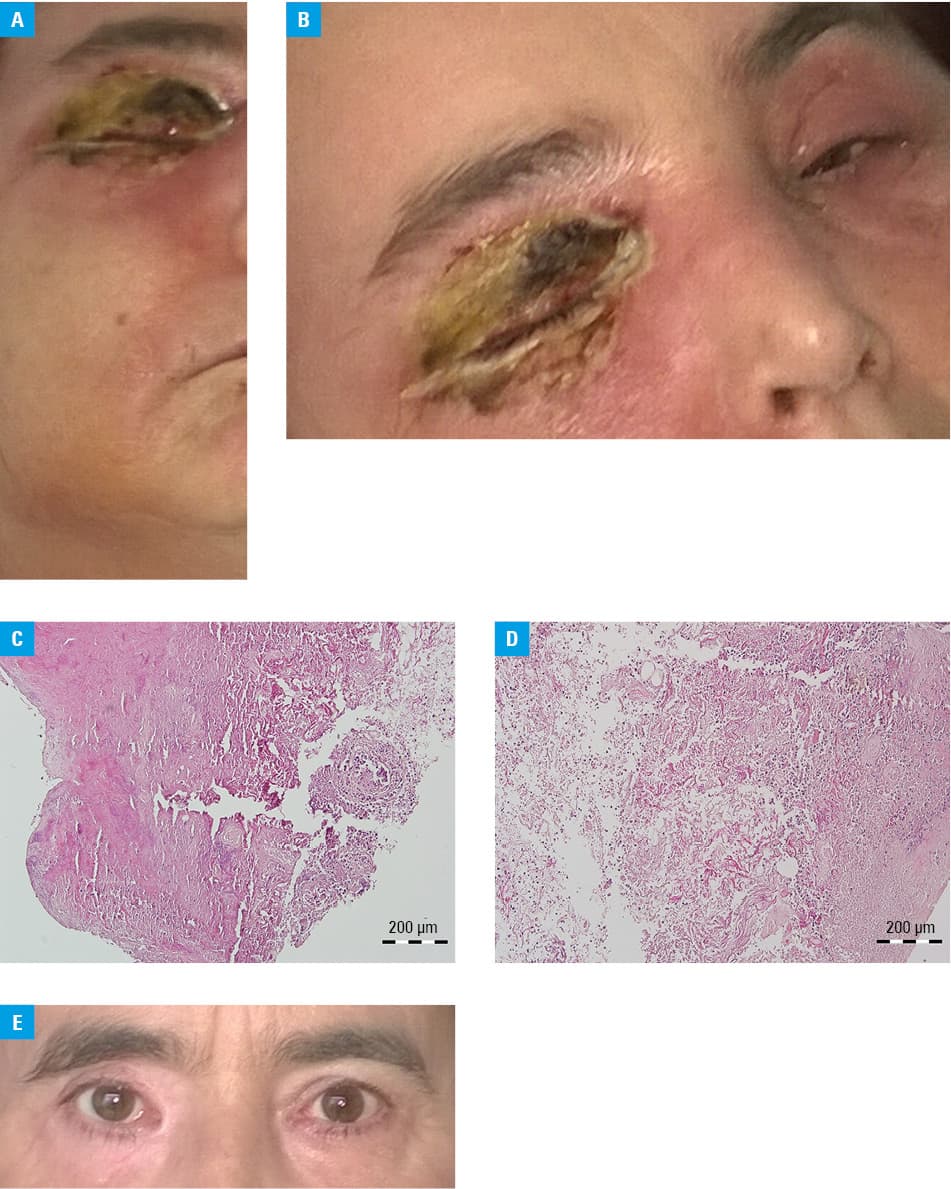
A 47‑year‑old white woman was admitted to a department of nephrology and transplantation medicine 11 years after receiving a kidney transplant from a deceased donor, due to orbital phlegmon and acute kidney allograft injury. At that time, immunosuppressive regimen was based on prednisone 5 mg once daily and mycophenolate mofetil 250 mg twice a day. Prior to the admission, the patient had been treated for 48 hours with topical tobramycin and dexamethasone due to blepharitis of the right eye. At admission, physical examination revealed right‑sided orbital inflammation with phlegmon and focal skin necrosis of the eyelids, accompanied by massive purulent conjunctival discharge. The inflammation, manifested as cellulitis, also involved the skin of the right cheek, right side of the neck, and left eyelids (Figure 1A and 1B). Submandibular lymph nodes were significantly enlarged. Examination of the anterior segment of the right eye was not possible due to narrow palpebral fissure and extreme tenderness of the tissues. Pupillary functions seemed unaltered and relative afferent pupillary defect was not present. Computed tomography (CT) and magnetic resonance imaging (MRI) did not show any orbital, sinal, or central nervous system involvement. Microscopic examination of surgically removed necrotic tissues affirmed morphologic features of Mucor (Figure 1C and 1D). Moreover, the intraoperative swab culture examination showed growth of Streptococcus pyogenes. Considering the high concentration of C‑reactive protein (493 mg/l; reference range [RR] <0.5 mg/l) and procalcitonin (>200 ng/ml; RR <0.05 ng/ml), parenteral treatment with liposomal amphotericin B, meropenem, and clindamycin was initiated. In addition, mycophenolate mofetil was discontinued and intravenous methylprednisolone was administered as the only immunosuppressive agent. Initially, the acute kidney allograft injury occurred with admission serum creatinine levels of 5.1 mg/dl (RR, 0.6–1.3 mg/dl), with subsequent gradual lowering over the course of treatment to 1.46 mg/dl at the time of discharge. During the last outpatient visit prior to the admission, serum creatinine concentration was 1.73 mg/dl. Due to improvement of the patient general condition, cyclosporin A was introduced into the treatment and parenteral glucocorticoids were converted to an oral form. Antifungal therapy was continued for 5 weeks and after the acute phase reactants normalized, the patient was discharged in good general condition and with good allograft function, unaltered visual acuity, and only some scarring on the skin of the eyelids (Figure 1E). Due to immunosuppression, kidney transplant recipients (KTRs) are susceptible to invasive fungal diseases (IFDs). Mucormycosis, which is an opportunistic infection caused by the members of a ubiquitous fungal order of Mucorales, accounts for 0.2%–1.2% of IFDs in KTRs.1 Different manifestations of the disease have been described, such as pulmonary, rhino‑orbito‑cerebral, gastrointestinal, cutaneous, and disseminated form.2 Risk factors for mucormycosis in KTRs include age, deceased donor, tacrolimus, nonwhite race, and Hispanic ethnicity.3 Cutaneous form may manifest as painful erythema with edema, progressing over time to ulceration and necrosis, covering deeper structures with fistulas.4 Diagnosis of mucormycosis is possible through microscopic examination, supported by immunohistochemistry or polymerase chain reaction techniques. Imaging exminations, such as CT or MRI, should be performed to evaluate the extent of changes. Cultures should also be performed, but the results are positive only in 50% of cases.5 Treatment includes administration of lipid formulations of amphotericin B, posaconazole, or both, and, if possible, surgical resection of necrotic tissue. Despite availability of specific treatment, the overall mortality rate ranges from 40% to 80%, depending on the site of infection and on the underlying conditions.5 Early diagnosis, surgical debridement of the infected tissue, and antifungal treatment are crucial in the management of mucormycosis.
- Petrikkos G, Skiada A, Lortholary O, et al. Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 2012; 54: 23‑34. | Crossref
- Steinbrink JM, Miceli MH. Clinical review of mucormycosis. Infect Dis Clin North Am. 2021; 35: 435‑452. | Crossref
- Downey MR, Taskar V, Linder DF, et al. Incidence and risk factors for mucormycosis in renal transplant patients. J Investig Med. 2022; 70: 396‑401. | Crossref
- Castrejón‑Pérez AD, Miranda I, Welsh O, et al. Cutaneous mucormycosis. An Bras Dermatol. 2017; 92: 304‑311. | Crossref
- Cornely OA, Alastruey‑Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019; 19: e405‑e421.
ARTICLE INFORMATION