A rare coexistence of intrathyroidal parathyroid gland and papillary thyroid carcinoma in a patient with MEN1 syndrome: a clinical, diagnostic, and surgical challenge

 CC BY 4.0
CC BY 4.0
A rare coexistence of intrathyroidal parathyroid gland and papillary thyroid carcinoma in a patient with MEN1 syndrome: a clinical, diagnostic, and surgical challenge
Hyperfunctional intrathyroidal parathyroid gland (IPG) is a rare condition responsible for approximately 2% of all hyperparathyroidism (HPT) cases, mostly affecting the inferior glands.1 Similarly to other ectopic locations, the intrathyroidal one may pose a diagnostic challenge, especially in patients with a concomitant thyroid nodule. Moreover, an undiagnosed IPG may cause considerable difficulties during surgical removal of the parathyroid gland. The association between thyroid and parathyroid pathologies is well known, although the relationship between papillary thyroid carcinoma (PTC) and HPT remains unclear, particularly in hereditary HPT.2,3
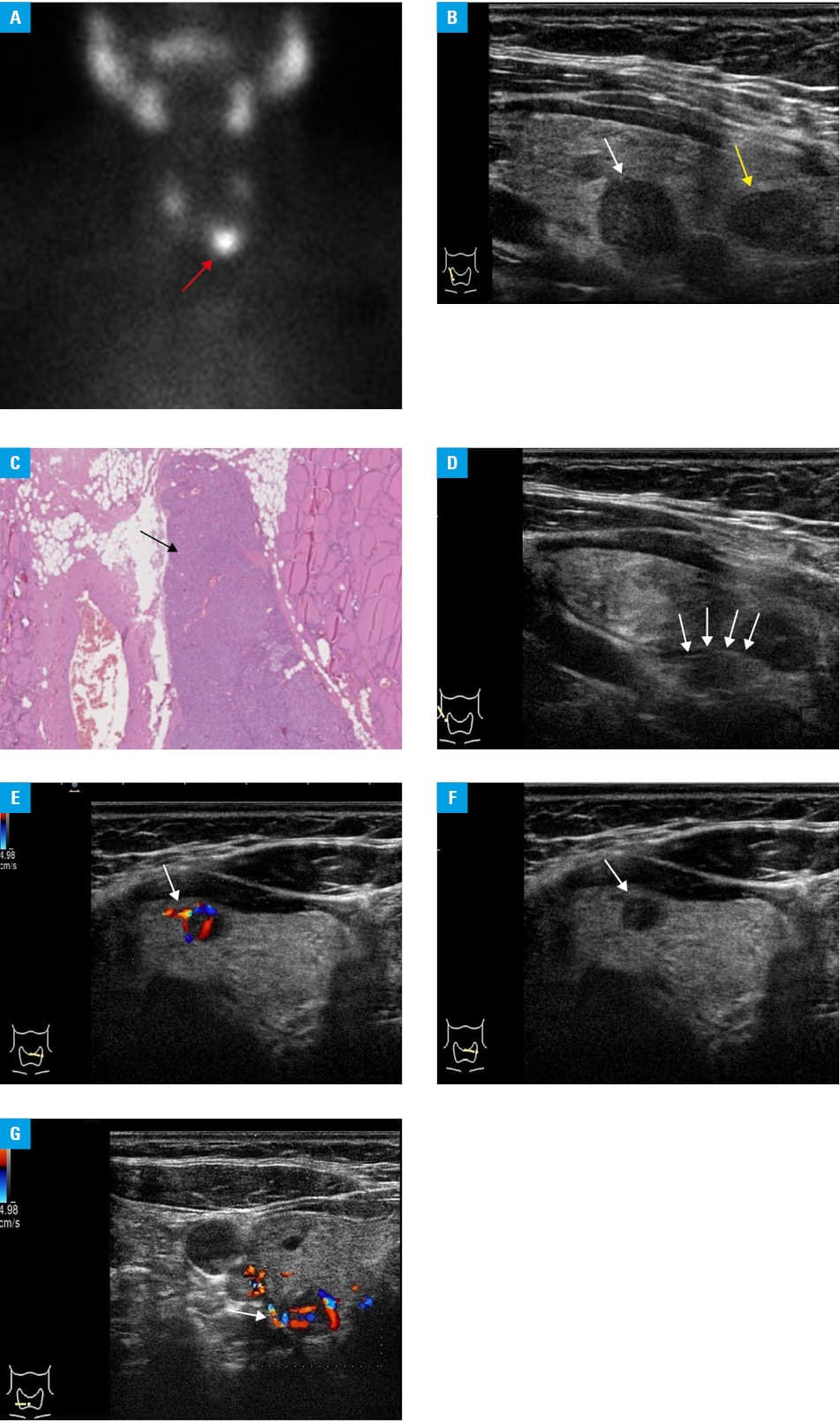
A 30‑year‑old woman with genetically confirmed multiple endocrine neoplasia type 1 (MEN1) syndrome was admitted to the department of internal medicine and endocrinology of the Medical University of Warsaw for a routine oncologic and endocrinologic follow‑up assessment related to genetic predispositions. At the age of 13, she had undergone enucleation of a solitary pancreatic tumor (size, 1 cm) confirmed by histopathology as insulinoma (World Health Organization grade G1; Ki‑67 index <2%). The symptoms suggestive of hypoglycemia recurred after 15 years, and included palpitations, sweating, dizziness, and confusion, especially after night sleep and exercise. First, the patient was referred to our department for further evaluation and management. The symptoms were similar to those observed by the patient and her family prior to the insulinoma resection. During initial hospitalizations, based on the prolonged fasting test results as well as abdominal computed tomography and magnetic resonance imaging findings, endogenous hyperinsulinemia due to multiple recurrent insulinomas was diagnosed. It was the first manifestation of MEN1 syndrome. The patient refused surgical interventions. She chose to focus on controlling her glucose levels through changing her diet, and began treatment with diazoxide and lanreotide analog somatostatin, which resulted in satisfactory control of hypoglycemia. She underwent biochemical screening for other MEN1‑related abnormalities. The results showed mild hypercalcemia (2.72 mmol/l; reference range [RR], 2.2–2.6 mmol/l) with increased parathyroid hormone levels (PTH; 132 pg/ml; RR, 10–65 pg/ml), which confirmed primary HPT (PHPT) as part of MEN1 syndrome. Renal and liver function parameters were normal. Bone densitometry showed signs of osteopenia. The patient was asymptomatic; however, she was referred for parathyroid resection due to young age. Imaging studies were performed for preoperative evaluation of the parathyroid glands. 99mTechnetium sestamibi scintigraphy showed an uptake of radioactivity at the inferior pole of the left thyroid lobe (Figure 1A), and ultrasonography identified potential right and left inferior parathyroid glands, several heterogeneous lesions in both lobes of the thyroid gland, and pathological cervical lymph nodes. The dominant nodules in the central part of the right lobe presented ultrasound features of malignancy, with the maximum diameter of 15 mm (Figure 1B). Similar nodules were observed in the lower part of the right lobe and in the upper part of the left lobe. Based on fine‑needle aspiration biopsy results, the dominant nodule in the right lobe was classified as category VI according to the Bethesda system, with cytologic nuclear changes typical of PTC. Hence, PHTP synchronous with multifocal PTC was suspected. The patient was immediately scheduled for neck exploration surgery with total thyroidectomy, central lymph node dissection, and subtotal parathyroidectomy. During the procedure, an experienced endocrine surgeon resected the pathological superior glands at their normal anatomical position. However, despite precise exploration, the inferior parathyroid glands were not identified. Nevertheless, an intraoperative measurement of serum PTH levels showed a decrease by over 90%, confirming a successful removal. In the early postoperative period, the patient developed symptoms of hypocalcemia, confirmed by laboratory test results of low PTH (5.6 pg/ml) and serum calcium (1.9 mmol/l) levels. This state exacerbated and continued despite substitution treatment involving oral and intravenous calcium supplementation, and the administration of active vitamin D and thiazide diuretics. Since partial improvement was seen over the course of 2 weeks, the decision of autotransplantation of cryopreserved parathyroid tissue into the subcutaneous tissue of a forearm was made due to a risk of permanent HPT. Surprisingly, the histopathological examination of the resected specimen showed not only PTC with multifocal small lesions in both lobes, but also 2 IPGs with features of hyperplasia (Figure 1C). The parathyroid origin could be confirmed by positive immunohistochemical staining for PTH and chromogranin A, and negative staining for thyroglobulin calcitonin and thyroid transcription factor 1. The lesions were originally assumed to be carcinoma foci. A retrospective evaluation of the ultrasound images showed that one of the IPGs presented a hyperechoic line, separating the thyroid gland from the intrathyroidal parathyroid adenoma (Figure 1D). Also, a pathognomonic Doppler vascular arc sign was seen in both glands (Figure 1E–1G).
Accurate preoperative localization of parathyroid lesions is essential for successful surgery. This report underlines potential difficulties in diagnosing HPT concomitant with thyroid carcinoma. Therefore, in practice, IPG should be considered in all HPT cases. Careful and precise evaluation of ultrasound findings may prevent potential intra- and postoperative complications.
- Gowrishankar SV, Bidaye R, Das T, et al. Intrathyroidal parathyroid adenomas: Scoping review on clinical presentation, preoperative localization, and surgical treatment. Head Neck. 2023; 45: 706‑720. | Crossref
- Jeong C, Kwon HI, Baek H, et al. Association of hyperparathyroidism and papillary thyroid cancer: a multicenter retrospective study. Endocrinol Metab (Seoul). 2020; 35: 925‑932. | Crossref
- Beebeejaun M, Chinnasamy E, Wilson P, et al. Papillary carcinoma of the thyroid in patients with primary hyperparathyroidism: is there a link? Med Hypotheses. 2017; 103: 100‑104. | Crossref
- Carullo J, Bani J, Averous G, et al. Hyperfunctioning intrathyroidal parathyroid: a misleading preoperative diagnosis. Nucl Med Mol Imaging. 2023; 57: 46‑50. | Crossref
- McClean A, England RJA. Revision parathyroid surgery – challenges and considerations in comparison to primary surgery. J Laryngol Otol. 2023; 137: 1233‑1236. | Crossref
ARTICLE INFORMATION