Coexistence of dilated cardiomyopathy with pre-existing testicular cancer in a young man: successful treatment ensured by interdisciplinary cooperation

 CC BY 4.0
CC BY 4.0
Coexistence of dilated cardiomyopathy with pre-existing testicular cancer in a young man: successful treatment ensured by interdisciplinary cooperation
A 35‑year‑old man with a 2‑year history of advanced heart failure (HF) in the course of dilated cardiomyopathy (DCM) was admitted to the National Institute of Cardiology for further diagnostics and qualification for orthotopic heart transplantation (OHT).
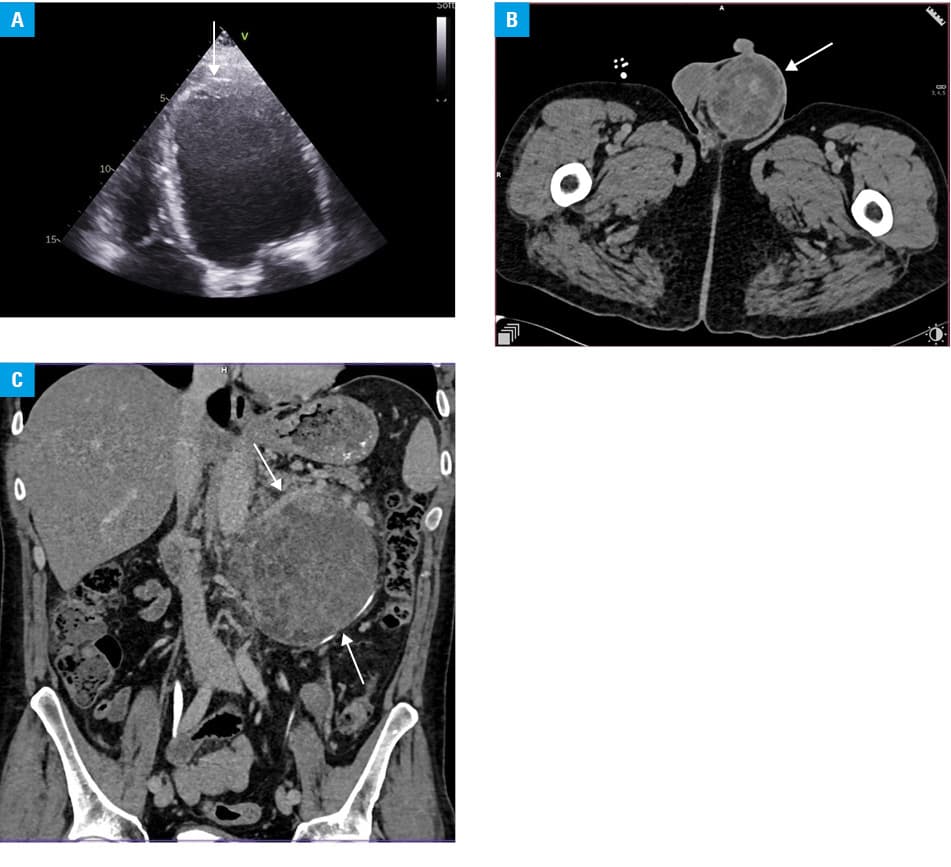
Laboratory workup showed an elevated level of N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP; 5717 pg/ml; reference range [RR] <125 pg/ml). On the second day of hospitalization, sudden cardiac arrest (SCA) in the course of ventricular fibrillation occurred. Successful resuscitation was performed and the patient was transferred to the department of intensive cardiac therapy (DICT). Transthoracic echocardiography (TTE) showed significantly dilated left ventricle (LV) with left ventricular ejection fraction (LVEF) of 13%, and a thrombus in the apex of the LV (Figure 1A). Physical examination showed enlarged left testicle, which was first noticed by the patient 6 weeks earlier. Computed tomography (CT) showed a tumor of the left testicle and a tumor in the retroperitoneal space (Figure 1B and 1C) with metastases to the lymph nodes and lungs. Coronary artery disease was excluded on CT angiography. Tumor marker levels were elevated: lactate dehydrogenase at 358 U/l (RR, 135–225 U/l), human chorionic gonadotropin β at 433 mIU/ml (RR, 5–50 mIU/ml), and α-fetoprotein at 7510 ng/ml (RR <5.8 ng/ml). On the third day of treatment, radical left‑sided orchidectomy was performed.
On day 10 of hospitalization, an interdisciplinary team consisting of a cardiologist, cardiac surgeon, urologist, and oncologist decided to administer a 3‑drug chemotherapy regimen (cisplatin, etoposide, and bleomycin). Prior to initiation of this therapy, myocarditis was excluded on magnetic resonance imaging and a cardioverter‑defibrillator was implanted.
On the 12th day of treatment at the DICT, chemotherapy was implemented. Simultaneously, standard HF pharmacotherapy and enoxaparin were also administered. Control laboratory workup showed reduction of the NT‑proBNP level to 177 pg/ml, and control TTE showed improvement of LVEF to 35%–40%. The patient’s condition significantly improved and he was transferred to the department of urological cancer of the National Institute of Oncology, where oncological treatment was continued.
Control CT showed stabilization of the neoplastic process. The patient was referred for retroperitoneal lymphadenectomy. Histopathological examination showed teratoma of a mature endodermal and mesodermal origin. After the procedure, all tumor marker levels normalized, and the neoplastic lesions in the retroperitoneum were radically removed. Currently, the patient is awaiting removal of the persistent lung lesions.
The coexistence of 2 uncommon and potentially lethal diseases, such as DCM and testicular teratoma is extraordinarily rare, which is why the treatment is usually individual and eludes the framework defined by guidelines. In this case, HF exacerbation can also be explained by the occurrence of paraneoplastic syndrome.1 Therefore, the improvement of heart function was not only due to the modification of the HF treatment, but also due to the intensive treatment of testicular cancer.
The presence of cancer, regardless of its nature, is an absolute contraindication for OHT. For nonmetastatic testicular cancer, the required time period between cure and organ transplantation is 2 years.2 For patients with severe heart damage, it may be too long because of a high risk of pulmonary hypertension, multiorgan dysfunction, or death from HF exacerbation or SCA caused by ventricular arrythmias, the incidence of which rises along with HF progression.3 At the time of the patient’s hospitalization, in Poland, qualification for OHT was required for implantation of a left ventricular assist device (LVAD), which would be a possible bridge until the end of the grace period. Therefore, the patient could not be a candidate for OHT or LVAD.
The close interdisciplinary cooperation and prompt therapeutic intervention not only resulted in curing the patient from advanced cancer, but also allowed for avoiding OHT and LVAD, and made the subsequent removal of nodal metastases in the retroperitoneum possible.
- Sanaka P, Reagan JL. Clinical overview: paraneoplastic syndromes. Elsevier. 2024.
- Chadban SJ, Ahn C, Axelrod DA, et al. KDIGO clinical practice guideline on the evaluation and management of candidates for kidney transplantation. Transplantation. 2020; 104: S11‑S103. | Crossref
- Wojtaszczyk A, Gąsior M, Szyguła‑Jurkiewicz B, Tajstra M. Prevalence of heart rhythm disorders in patients with end‑stage heart failure referred to qualification for heart transplantation. Kardiol Pol. 2022; 80: 339‑341. | Crossref
ARTICLE INFORMATION