Paravertebral echocardiographic views: a window that should be open wider for diagnosis and monitoring of thoracic aortic aneurysms

 CC BY 4.0
CC BY 4.0
Paravertebral echocardiographic views: a window that should be open wider for diagnosis and monitoring of thoracic aortic aneurysms
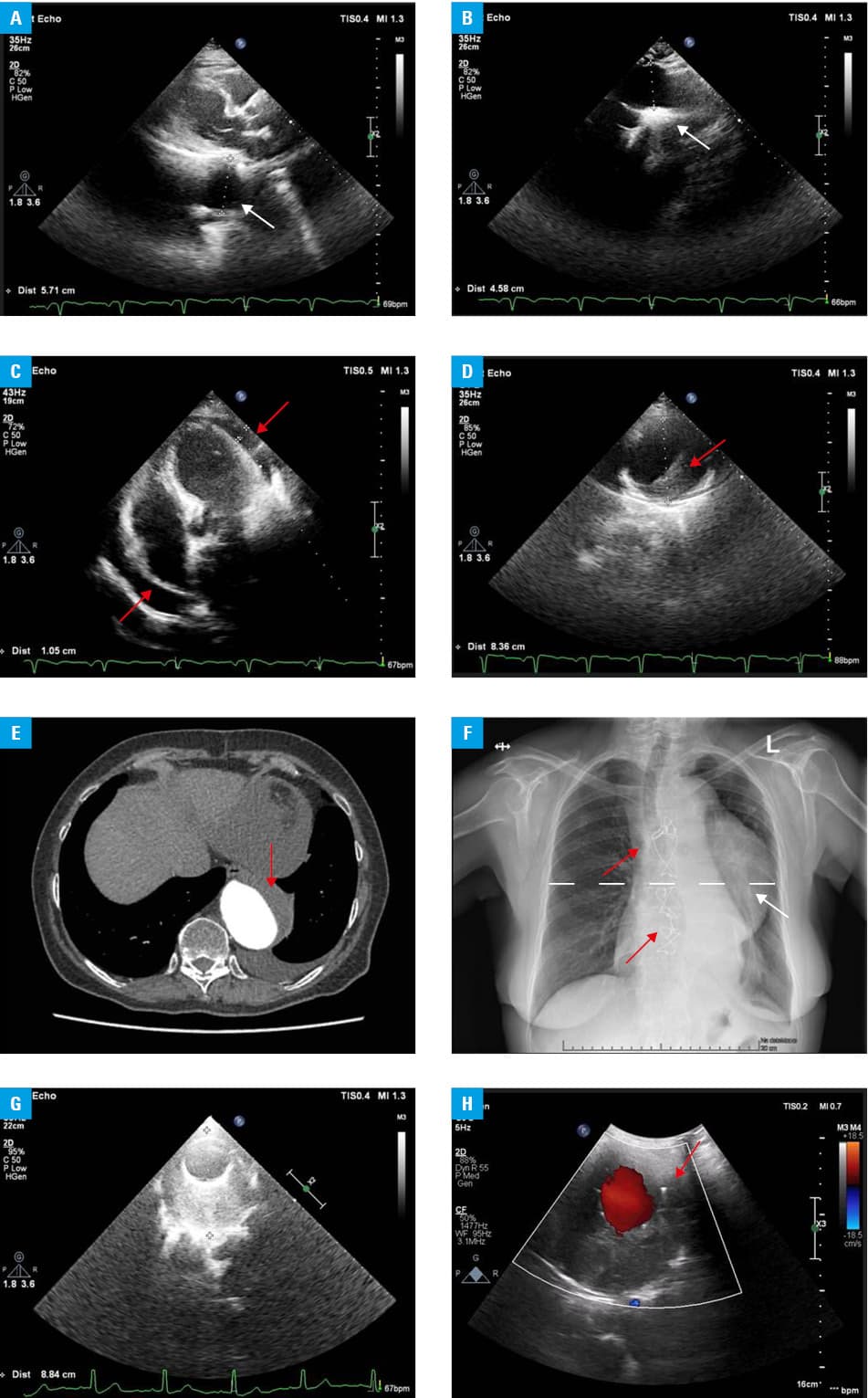
Transthoracic echocardiography (TTE) remains the first‑line method in a differential diagnosis of acute chest pain and in detection and monitoring of aortic diseases. However, its potential in the examination of thoracic aortic aneurysms (TAAs) is often underused in clinical practice, for example, by limiting imaging to the anterior chest surface (Figure 1A and 1B), which may delay adequate diagnosis and result in excessive risk of death and complications.1,2
A 65‑year‑old woman (height, 158 cm; weight, 56 kg), with hypertension and diabetes, was admitted to our department due to anemia (hemoglobin, 8.1 g/dl, reference range [RR], 12–16 g/dl), increased inflammatory markers, reduced glomerular filtration rate of 33 ml/min/1.73 m2 (RR >60 ml/min/1.73 m2), and D‑dimer level over 7000 ng/ml (RR <500 ng/ml).
Three months before, she underwent cardiac surgery of an aneurysm of the ascending aorta with spared native aortic valve and a supracoronary prosthesis insertion. Six months earlier she had undergone embolization of a cerebral anterior artery aneurysm, having in her medical history also gastric ulcer perforation. On anamnesis, a recurrent sensation of chest pressure at rest was reported. TTE (standard parasternal, apical, suprasternal, and subcostal views) showed the postoperation status of the ascending aorta and aortic arch (Figure 1A and 1B) as well as a widened part of the descending aorta at the diaphragm level. Moreover, a moderate amount of pericardial fluid (Figure 1C) was noted, which raised the imaging red flag for the patient’s status. Despite good tolerance of the left lateral position, after sitting up the patient suffered from a strong back pain, dyspnea, and her heart rate increased by 20 bpm. This clinical instability prompted widening of TTE to the lung fields, including the left paravertebral (PV) scanning, which may provide an accurate image of the extended, dissected, or aneurysmatic aorta.3-5
Indeed, in this atypical and often omitted view, we could clearly observe a large TAA (diameter >8 cm) with thrombus in the anterolateral part (Figure 1D), corresponding probably to a thrombotic false lumen of a chronic dissection (Figure 1E of subsequent urgent computed tomography [CT]). The location of the maximal TAA diameter was visible also on chest X‑ray (Figure 1F).
Considering the unstable status, abnormal imaging and laboratory data, threatening rupture of the TAA was diagnosed. The patient was immediately transferred to a vascular surgery department, where a stent‑graft (Tbranch, Cook Medical, Limerick, Ireland) was implanted to the descending aorta without further complications (Supplementary material, Figure S1). A year later the patient underwent CT and TTE, which provided PV views of TAA and the implanted stent‑graft (Figure 1G and 1H). At follow‑up, the patient presented in stable condition, without chest and back pain, pericardial fluid, or aortic disease progression.
This clinical image illustrates high utility of TTE, enriched with the PV views, in aortic syndromes, as the fastest and the most clinically useful bedside technique in acute settings, as well as the contrast- and radiation‑free method, unfortunately still underused in long‑term monitoring.
- Iliceto S, Ettorre G, Francioso G, et al. Diagnosis of aneurysm of the thoracic aorta. Comparison between two non invasive techniques: two‑dimensional echocardiography and computed tomography. Eur Heart J. 1984; 5: 545‑555. | Crossref
- Erbel R, Aboyans V, Boileau C, et al. ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014; 1: 2873‑2926. | Crossref
- Makihata S, Tanimoto M, Yamamoto T, et al. Two‑dimensional echo‑Doppler technic for evaluating dissecting aneurysms using the paravertebral approach. J Cardiogr. 1985; 15: 181‑195.
- Prastaro M, Losi MA, Pastore F, et al. Paravertebral echocardiographic views and thoracic aortic dissected aneurysm. Eur J Echocardiogr. 2011; 12: 480. | Crossref
- Blanco P. Paravertebral echocardiographic views in a patient with acute aortic dissection. Int J Cardiovasc Imaging. 2015; 31: 707‑708. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION