How to better prevent sudden cardiac death? Recent advances
Key words: automated external defibrillator, prevention, sudden cardiac death

 CC BY 4.0
CC BY 4.0
How to better prevent sudden cardiac death? Recent advances
Sudden cardiac death (SCD) is a global public health problem. Despite efforts of the scientific community, it is characterized by low survival (<10%). Strategies used to prevent this catastrophic event are divided into those aimed at individual and populational level. Individuals known to be at a high risk for SCD may be treated with medications, implantable cardioverter‑defibrillators, catheter ablation, or temporary defibrillation devices. At the population level, efforts are concentrated on prevention of ischemic heart disease, as it is responsible for over 70% of sudden mortality cases in adults, and on development of resuscitation and early defibrillation programs. Much still needs to be done to improve survival by raising awareness in the population through training initiatives and by optimizing available technologies and making them more accessible.
Introduction
Sudden cardiac death (SCD) accounts for 15%–20% of overall mortality, has an estimated annual burden of 4–5 million cases, and therefore is a public health problem of great magnitude.1-3 Due to its unexpected nature, it is still associated with poor overall survival (<10%).4,5
However, a lot has been done by the scientific and public health community to improve prevention and early response strategies (resuscitation) both at the individual and population level.6-8 Preventive measures have focused on identifying high‑risk individuals among patients with known underlying electrical or structural heart disorders and preventing coronary artery disease (CAD) responsible for nearly 70% of SCDs.9-11 On the population level, public initiatives have aimed at raising awareness and educating people on recognition of cardiac arrest (CA) and early intervention steps.6-8,12
The most common cause of SCD is ischemic heart disease (IHD), and its consequences (acute myocardial ischemia, scarring from previous myocardial infarction [MI], heart failure [HF]) manifest in 80% of SCD victims. Dilated nonischemic and hypertrophic cardiomyopathy (HCM) are the next more common causes of SCD, whereas other cardiac disorders, including congenital heart defects and ion channel anomalies, account for 5%–10% of SCD cases. The spectrum of SCD risk factors varies with age. In young people, it is predominantly due to channelopathies, cardiomyopathies, and myocarditis, while in older populations the main risk factor is CAD.
Predicting and preventing sudden cardiac death: the epidemiologic paradox
The paradox regarding relative risk vs absolute event count has been described in the 1990s by Zipes and Wellens13: individuals at the highest risk (those with a history of malignant ventricular arrhythmias [VAs] in the context of structural heart disease) only account for a limited number of the total SCDs per year (Figure 1).
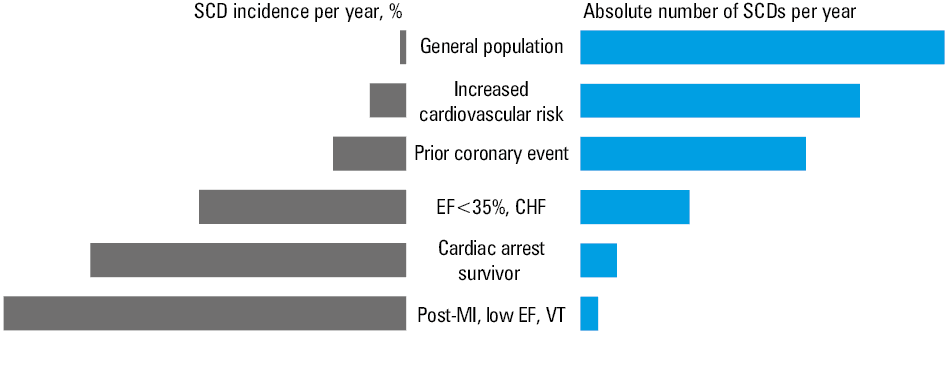
Abbreviations: CHF, chronic heart failure; EF, ejection fraction; MI, myocardial infarction; SCD, sudden cardiac death;
VT, ventricular tachycardiaThe incidence in the general population without known heart disease is relatively low (0.1%–0.2% per year), however, a majority of SCD events occur in this group. Therefore, therapeutic measures addressing patients in small high‑risk subgroups (easier to identify) only have a limited overall impact on the total number of SCDs.
The accurate prediction of SCD risk in the general population remains a major challenge with a chance to significantly reduce SCD burden. Ongoing studies based on big data and artificial intelligence suggest that personalized prediction of SCD may be based on a multiparametric approach involving a combination of multiple specific markers.14
Preventing sudden cardiac death at an individual level
SCD prevention can be aimed at preventing the underlying cardiac disease causing SCD or preventing SCD in patients with established heart disease (Figure 2).
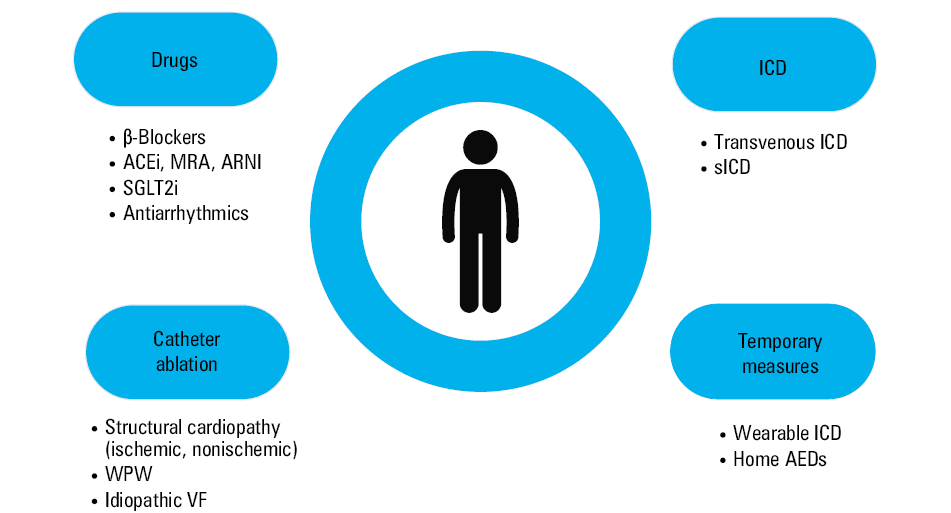
Abbreviations: ACEi, angiotensin‑converting enzyme inhibitor; AED, automated external defibrillator; ARNI, angiotensin receptor / neprilysin inhibitor; ICD, implantable cardioverter‑defibrillator; MRA, mineralocorticoid receptor antagonist; sICD, subcutaneous ICD; SGLT2i, sodium‑glucose cotransporter‑2 inhibitor; VF, ventricular fibrillation; WPW, Wolff–Parkinson–White syndrome
Drugs
Pharmacologic treatment to reduce SCD risk includes drugs that modify the arrhythmia substrate and antiarrhythmic agents.
β-Blockers not only have been shown to reduce mortality in patients with HF and CAD, but also to reduce the risk of SCD and VAs.15-18
Angiotensin‑converting enzyme inhibitors, angiotensin II type 1 receptor blockers, and mineralocorticoid receptor blockers improve myocardial remodeling and reduce the risk of SCD.19-21
Administration of dual antagonist of angiotensin II and neprilysin receptors (angiotensin receptor / neprilysin inhibitor [ARNI]) resulted in 20% reduction in SCD risk in HF patients with reduced ejection fraction (EF). ARNI has also been associated with improvements in diastolic function, left ventricular function, quality of life, and burden of VAs.22-24 Sodium‑glucose cotransporter‑2 inhibitors have been shown to reduce the risk of worsening HF or death from cardiovascular causes regardless of the presence of diabetes in patients with HF.25-27
Statins are known to have a beneficial effect on SCD; particularly, their use has been associated with a reduction in the risk of SCD, since most SCD cases are associated with ischemic cardiomyopathy.28 Among antiarrhythmic drugs, amiodarone is currently only indicated to treat symptomatic VAs. It reduces the incidence of implantable cardioverter‑defibrillator (ICD) shocks but does not improve survival.29
Mexiletine can be used in patients with type 3 long QT syndrome to reduce arrhythmic events,30 and quinidine has some positive effects in patients with Brugada syndrome.31
Implantable cardioverter‑defibrillator
The first ICDs were approved for implantation in the United States in 1985, and were indicated in survivors of CA or life‑threatening arrhythmia. Patients with documented ventricular fibrillation (VF) or hemodynamically nontolerated ventricular tachycardia (VT) in the absence of reversible causes are considered for secondary preventive ICD implantation.32 However, they represent only a small percentage of those who receive an ICD; in fact, most of the patients are implanted in the context of primary prevention.
Primary prevention ICD implantation is recommended by the European Society of Cardiology (ESC) guidelines in the following cases:
-
Left ventricular dysfunction: ICD therapy is indicated in patients with symptomatic HF (New York Heart Association class II–III) regardless of its etiology and left ventricular EF (LVEF) up to 35% after more than 3 months of optimal medical therapy who are expected to survive for at least 1 year with good functional status.
-
Cardiomyopathies: ICD implantation should be considered in the case of dilated cardiomyopathy with a disease‑causing mutations in lamin A/C genes and at least 2 of the following risk factors: nonsustained VT on ambulatory electrocardiogram (ECG) monitoring, LVEF below 50% at first evaluation, male sex, and nonmissense mutations (insertion, deletion, truncations, or mutations affecting splicing). In patients with HCM, the decision is based on the 5‑year SCD risk according to the HCM Risk‑SCD model. An ICD should be implanted in patients with arrhythmogenic right ventricular cardiomyopathy and arrhythmic syncope or nontolerated sustained VT.
-
Inherited primary arrhythmia syndromes: ICD implantation is recommended for secondary prevention. Moreover, it is recommended in patients with long QT syndrome who experienced syncope and / or VT while receiving an adequate dose of β-blockers. It may be considered in high‑risk patients, such as women with LQT2 and corrected QT longer than 500 ms, patients with corrected QT longer than 500 ms and signs of electrical instability, and those with high‑risk genetic profiles. It is also indicated in patients with Brugada syndrome with documented VT, where it should be considered in those presenting with a spontaneous type 1 ECG pattern and a history of arrhythmic syncope.
-
Finally, ICD implantation is recommended in patients with catecholaminergic polymorphic VT and recurrent syncope or polymorphic / bidirectional VT despite optimal therapy (β-blockers or flecainide).
Particular attention must be paid to patients suffering from HCM, the most frequent cause of genetically determined SCD. Several studies confirm the effectiveness of ICD in primary and secondary prevention in patients with HCM, with appropriate device interventions occurring in more than 50% of patients from the secondary prevention group and 16.7% of patients who received an ICD for primary prevention.33
The guidelines regarding primary prevention are therefore based solely on EF, with a cutoff of 35%. This approach has been supported by landmark primary prevention trials conducted in the 1990s and 2000s.34-36 However, in the current clinical context, the literature regarding prophylactic ICD implantation appears to have noticeable limitations, since medical therapies currently available have improved considerably and differ significantly from those used more than 20 years ago, just as reperfusion techniques in the case of IHD and resynchronization therapies have undergone notable changes.37
In this sense, the DANISH trial (Danish ICD Study in Patients with Dilated Cardiomyopathy),38 conducted more recently with up‑to‑date medical therapy available, has shown that in patients suffering from nonischemic heart disease the implantation of ICDs for primary prevention does not reduce mortality. Sudden mortality in patients with HF has significantly decreased over the last 20 years, so it would be important to consider the issue of competing risks. In fact, several predictive markers of SCD (such as diabetes, renal dysfunction, atrial fibrillation) are also predictive of nonsudden mortality, and the more comorbidities, the greater the probability of nonsudden death, and therefore reduced the benefit of implanting an ICD. As reported in the CERTITUDE study,39 95% of the excess mortality in cardiac resynchronization therapy patients without a defibrillator was not associated with SCD. The DANISH study data also indicate that patients with IHD benefit more from ICD implantation than individuals with nonischemic heart disease.38
Therefore, the current approach of selecting candidates for the implant based solely on EF appears to be neither sensitive nor specific in classifying patients at a low or high risk of SCD. In fact, there are patients who receive an ICD based on low EF who will in fact never need the therapy but are exposed to the risk of device‑related or lead‑related complications, and there are patients who present a high risk of SCD but are not recognized as ICD candidates, because their EF exceeds 35%.
The ongoing PROFID trial (Prevention of Sudden Cardiac Death after Myocardial Infarction by Defibrillator Implantation)14 aims at identifying more sensitive and specific parameters than EF to recognize high‑risk patients also with big data analysis. It involves 2 optional substudies (on cardiac magnetic resonance imaging and on genomics), and an artificial intelligence‑based analysis of 12‑lead ECG will be used to develop personalized prediction of SCD.
In the future, the use of longer‑lasting (or rechargeable) batteries could reduce the risk of infections associated with replacements, and the use of extravascular systems (also with a possibility of pacing with a subcutaneous ICD) could reduce the risk of other lead‑related complications.40
A technology called optogenetic defibrillation, which allows for the cellular electrical activity to be modified (both in terms of pacing and defibrillation) through epicardial illumination mediated by short blue‑light pulses, is also being studied with promising results.41
Catheter ablation
While ICD can terminate VAs, it cannot prevent their recurrence, which, however, can be achieved with catheter ablation. Wolf–Parkinson–White syndrome can cause SCD and is effectively treated by ablation. Studies regarding prophylactic ablation to reduce SCD risk in the context structural heart disease (both ischemic or nonischemic) have not provided conclusive results; however, ongoing trials will hopefully clarify its usefulness in specific settings.42-44
In recent years, idiopathic VF triggered by premature ventricular complexes originating from the Purkinje fibers and premature ventricular complex‑induced cardiomyopathy have been successfully treated with catheter ablation.
Wearable defibrillator
There are some conditions in which the risk of sudden death is temporarily higher, such as in patients with myocarditis or in the first weeks after MI. Wearable cardioverter defibrillators or life vests are useful tools in patients with a transiently more severe SCD risk profile.45
The use of small devices with defibrillation capabilities in the context of home defibrillation programs is being studied. This approach is promising, but it requires compliance from a patient’s caregiver and has potential psychological effects on sudden CA survivors and their families.46
Preventing sudden cardiac death in health care systems and communities
Lifestyle measures
At a population level, interventions addressing traditional coronary disease risk factors have been implemented in the past decades. Smoking cessation, healthy diet, and physical exercise can reduce SCD burden.47,48 Recently, the role of nontraditional risk factors, such as air pollution, has attracted considerable attention. In fact, uncontrolled urbanization and increased pressure of environmental stressors have been associated with elevated risk of cardiovascular diseases and VAs.49 Community‑based programs aimed at reducing air pollution through improved public transportation and reduced CO2 emissions have been proposed and further studies will be needed to measure how these initiatives may affect cardiovascular and SCD risk over time.
Early recognition and intervention: rationale for public‑access defibrillation programs
It is estimated that over 75%–80% of out‑of‑hospital CA (OHCA) cases occur at home, and less than one‑third in public places.50 A recent report by the International Liaison Committee on Resuscitation (ILCOR) published in 2017 considered 9 national and 7 regional OHCA registries, reporting survival between 3% and 20% 30 days after resuscitation; with better survival (11%–47%) in the case of witnessed OHCA and with a shockable rhythm. In environments with public access to defibrillation, such as sports facilities, survival rises to 70%–90% thanks to early defibrillation.51 It is now clear that the time to defibrillation is of crucial importance in determining survival: the shockable rhythms, which can be effectively treated by early electrical defibrillation, in fact deteriorate within minutes into nonshockable rhythms characterized by a significantly worse prognosis.52,53 Some case studies, in which the automated external defibrillator (AED) was applied and the rhythm was recorded on arrival, report the incidence of shockable rhythms between 36% and 79% in the case of witnessed OHCA, depending on whether the arrest occurred at home or in a public place and on the time of assistance arrival on site. In fact, the incidence of shockable rhythms, such as first‑detection rhythms, is significantly reduced in the same case series, to 25% and 38% when the intervention by the emergency medical system (EMS) takes place at home or in a public place, respectively, due to a longer time of the assistance arrival.54
This is supported from a physiopathological point of view by a 3‑phase model of CA. The first phase is the electrical phase (within 3–4 min of syncope), the second phase is the circulatory phase (from 4 to 7 min), and the third phase is the so‑called metabolic phase (after 10 min; Figure 3).55
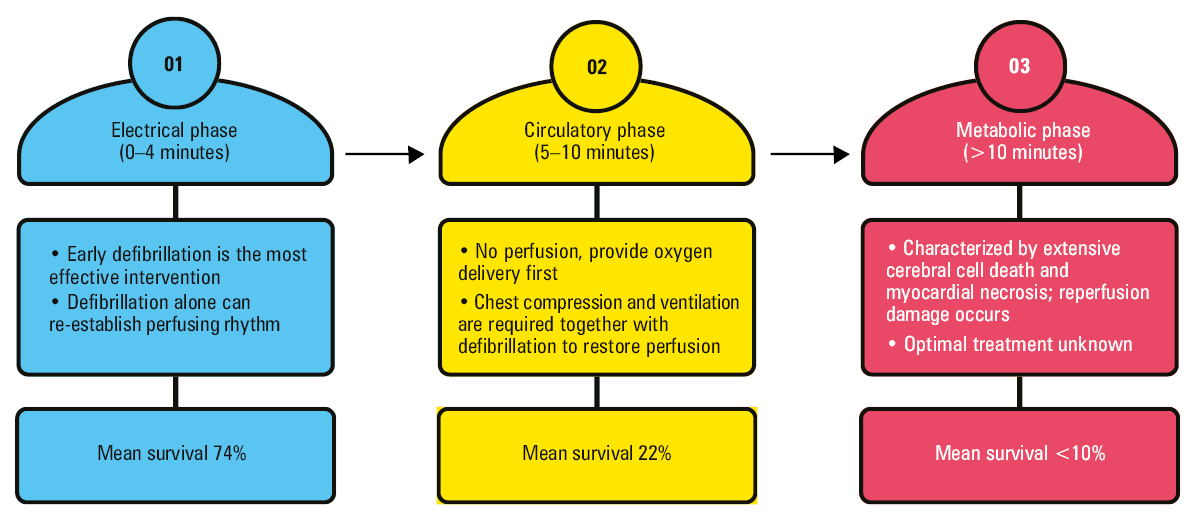
During the electrical phase of CA, blood pressure drops but not to zero. The arterial pressure remains between 15 and 20 mm Hg, higher than the central venous pressure, which is approximately 5 mm Hg. In this phase, a gradient remains between the arterial compartment and the venous compartment, which maintains circulation, albeit at minimal speeds. Defibrillation is most effective in restoring the spontaneous cardiac rhythm, and it also re‑establishes the circulation and pressure independently of the basic life support maneuvers. A study conducted by Gilmore et al55 demonstrated that if an action is taken in the very first minutes of CA, during the electrical phase, survival is independent of cardiopulmonary resuscitation (CPR), if defibrillation is performed promptly. In the subsequent phases, survival rate is progressively reduced, and CPR maneuvers combined with defibrillation are fundamental for effective resuscitation. In the circulatory phase of CA, blood pressure drops to zero. In this phase, survival is significantly reduced, and it is necessary to support circulation with cardiac massage and ventilation, as well as to interrupt the arrhythmia with defibrillation. Finally, in the third metabolic phase, the ischemia / reperfusion damage due to a lack of circulation becomes permanent and requires complex means of cardiac support with the lowest probability of survival.
The American Heart Association defines well what public access to defibrillation means: “making AEDs available in public or private places where large numbers of people gather or where people at high risk of cardiac arrest live.”56
Early defibrillation, performed by witnesses or so‑called first responders, represents an organizational approach that may increase survival from OHCA. In fact, further reducing the EMS arrival time is impossible. A study funded by the United Kingdom Department of Health found that reducing ambulance times was not a cost‑effective policy.57 Ong et al58 showed that the average EMS response time in Singapore was 9.6 minutes, making public access to defibrillation an essential link in the chain of survival. Numerous studies have demonstrated that early defibrillation, regardless of who performed it, was associated with favorable neurological outcomes.59 Ringh et al60 demonstrated that defibrillation with public AEDs had higher survival rates than defibrillation by EMS due to a much shorter time to defibrillation.
Unfortunately, in Europe, there are still few communities organized according to the early defibrillation model, and the AEDs present in public places are often underused. According to the ILCOR data, AEDs available in the case of OHCAs are used only in 2% to 37% of cases, mainly due to missing integration with emergency services and a limited knowledge of defibrillation in the community.51
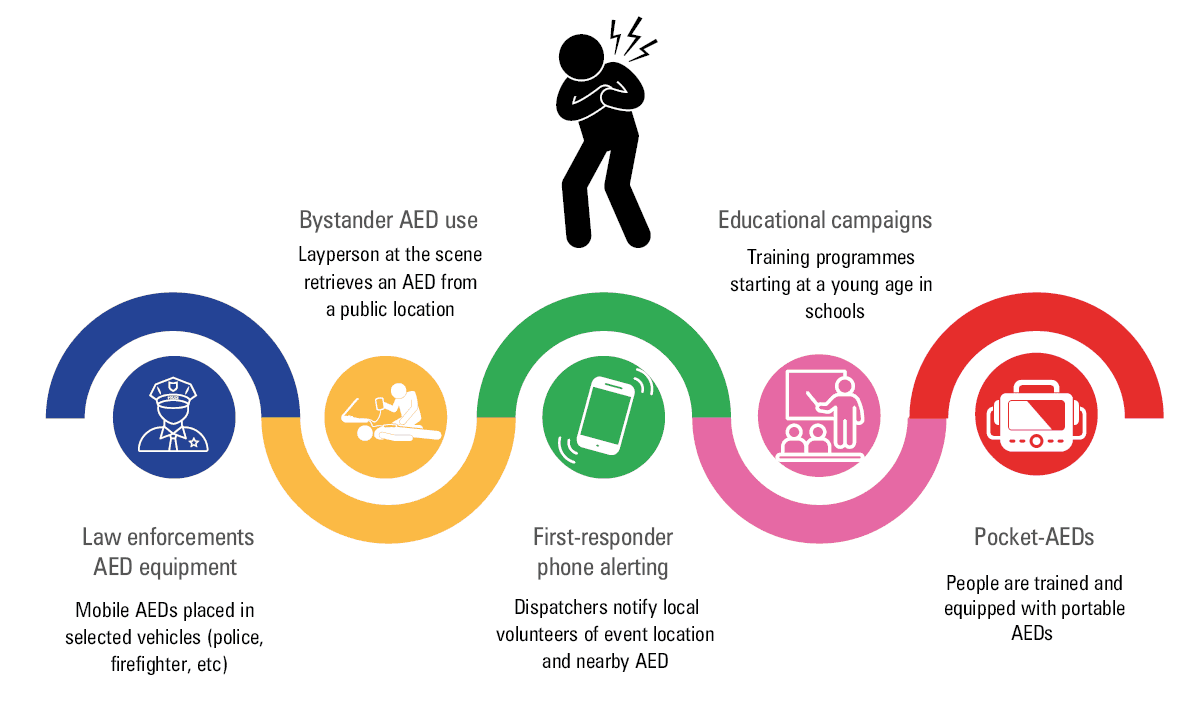
The programs of early defibrillation are based on establishing a widespread network of AEDs and training potential users, who can apply the AED in the shortest time possible (Figure 4).
In the 1980s, many projects were launched to involve communities in the use of AEDs in public places.61-64 These devices have become increasingly simple to use, with guiding voices that assist in various phases of the rescue procedure and more precise algorithms for the recognition of arrhythmias, reducing the recognition time to less than 20 seconds.63 In Rochester, Minnesota, United States, between 1990 and 1995, 31 patients with OHCA were treated with AEDs by the police, with a survival to hospital discharge of 58%.65 Over the years, several projects have demonstrated effectiveness of early defibrillation in various contexts, including OHCA in public and private places.60,66
In Europe, the city of Piacenza, Italy, has played a pioneering role in the implementation of an early defibrillation system since 1998, thanks to the Progetto Vita program.67 The project involved law enforcement and volunteer rescuers and availability of AEDs in various public places. Timely interventions of lay rescuers with AED significantly increased survival as compared with traditional EMS (15.5% in the volunteer group vs 4.4% for the EMS; P = 0.002), already in the first published cases.68 Similar success was achieved in Seattle in 2002, where survival from OHCA was 27%, 3 times the national average at that time.68
In a randomized study, Hallstrom et al69 demonstrated that survival to discharge from a hospital was higher when lay volunteers used the AED together with CPR than when CPR alone was used (30/128 survivors in the CPR+AED group vs 15/107 in the CPR only group; P = 0.03).
However, most of the available data are based on observational registries, which show an increase in AED use over time (from 21.4% in 2006 to 59.3% in 2012), and a reduction in the time between the onset of OHCA and connection of the AED carried out by lay people present on site (8 vs 9.9 min; P <0.0001).70-72 Berdowski et al73 reported improved neurological outcome on discharge in patients rescued with AEDs present on site vs individuals who were rescued without the use of an AED and in whom defibrillation was carried out upon arrival of medical assistance.
Data relating to a Japanese national register published by Kitamura et al74 highlighted an increase in the use of public AEDs from 1.1% in 2005 to 16.5% in 2013, which was associated with a greater probability of survival with favorable neurological outcome in the case of intervention by lay rescuers with public AEDs (38.5% vs 18.2% for EMS).
Recently, numerous studies have aimed at evaluating the economic effectiveness of AED distribution in public spaces. One of the most relevant works by Andersen et al75 highlighted how, in the United States, installation of AEDs in public spaces is advantageous from an economic point of view, and suggested their wider distribution over the country’s territory.
The 2015 ILCOR guidelines76 strongly recommend promoting public access to defibrillators. The most recent guidelines of the ESC, published in 2022,32 support early defibrillation as a class I intervention, with a high degree of scientific evidence, in the fight against sudden death.
The strategies of organizing early defibrillation assistance can be divided into 3 main categories:
-
Two‑tiered system, in which medical personnel of ambulances and police forces equipped with mobile AEDs are alerted simultaneously by a dispatcher of an emergency system;
-
Bystander system, in which AEDs are installed in public and private places accessible to passers‑by and are used by witnesses while waiting for the arrival of medical professionals;
-
Network of occasional rescuers (first‑responder network), that is, a network of non–health care volunteers, known as lay rescuers, available through a communication system coordinated via an EMS.
It is important to underline that these organizational approaches are not mutually exclusive. The choice depends on a specific situation and increasing availability of AEDs in the communities.
However, despite efforts to promote the distribution of AEDs and CPR education, the data available in the literature and our practical experience show that less than 12% of patients suffering from SCA are treated with an AED. This rate is particularly low in private places as compared with public ones (1.3% vs 15.3%).77 This is because AEDs are not yet so widespread, and because approximately 50% of OHCAs are unwitnessed.
Educational interventions certainly increase the percentage of patients receiving bystander CPR and defibrillation. An example of this are the educational campaigns conducted in North Carolina, United States78 and Japan,79 which correspond to a greater probability of survival without neurological damage. However, it is necessary to simplify and concentrate public training on the use of AEDs, with or without CPR, to increase the number of interventions. Simplified training programs have been shown to reach a wider audience and are more likely to be successful.80 The American Heart Association’s “Nation of Lifesavers” program, the British Heart Foundation’s “Call, Push, Rescue,” Osaka’s “PUSH” project, and Singapore’s “DARE” (Dispatcher‑Assisted first Responders) program are examples of streamlined training programs focused on teaching compression‑only CPR and AED.
The simplification should be supplemented by educational campaigns aimed at promoting CPR skills from a young age, in all schools of all levels. Annual training programs, lasting 1–2 hours, conducted by adequately trained teaching staff, are essential to develop in teachers the abilities to educate students on the use of the AED and CPR maneuvers, so that during their school career every student becomes capable of intervening in the event of OHCA. This organizational aspect is of considerable importance and must be addressed in parallel with the distribution of AEDs.
Challenges for the future
In the context of OHCA and early defibrillation, it is essential to consolidate the efforts of the scientific community. The creation of national and European CA registries is of primary importance, as it would allow for a better understanding of any organizational disparities and a more precise definition of intervention and improvement strategies.
Most CAs occur at home; therefore, strategies for early home defibrillation need to be implemented.
Our organization started the “Condominium Life Project” in 2017 that involved installation of 150 AEDs in the condominium areas of Piacenza. In condominiums, rescue interventions are challenging due to architectural barriers, difficult access, or stairs that delay the arrival of medical professionals. An analysis of OHCA cases in various areas of the city was initially carried out and neighborhoods with the highest mortality were identified. Following this, preliminary meetings were held with the administrators of the condominiums to obtain authorization to place the AEDs on the walls, approximately 150–200 m from each other. Business owners from various neighborhoods were also involved and information evenings were organized for residents, during which the objectives of the project and a map of the AED locations were presented. Starting from September 2017, the placement of the AEDs began with adequate signage to facilitate rapid access.
Automatic and semiautomatic external defibrillators of the future
Current AEDs are designed for intensive use, that is, they allow for sustained and repeated use over time with 250 shocks available. They may serve for several years with maintenance involving replacement of electrodes and batteries at scheduled intervals (4–5 years for batteries, approximately 2 years for electrodes). However, most AEDs installed in public places are used rarely and require few shocks, following which, whether effective or not, expensive electrodes and batteries must be replaced. In the future, it would be desirable to use cheaper technologies, with a possibility of delivering a limited number of shocks, with less expensive and easily portable devices also for home use. Technologies aimed at miniaturization of AEDs are already being developed. So‑called ultraportable AEDs can be easily transported into various locations and function as “bridges” until the arrival of professional emergency services.80 Thus, an option emerges of moving from AED equipment installed in public spaces to AEDs stored at home for personal use. The new AEDs will soon be portable, pocket‑sized, light, small, and inexpensive. An Australian company is already advertising a CellAED device with the CE mark. A compromise is sought between the device performance and its cost. The solution is made plausible by the fact that the use of an AED is never an alternative to an intervention of emergency services, which must always be alerted in the event of OHCA. The single‑use personal AEDs will be accessible to a much larger part of the population and could in the future significantly increase survival by offering greater availability and a possibility of earlier and more numerous interventions in the community. Home defibrillation is a real challenge for the future, and it will be simpler to implement with these personal, easily available devices.
- Empana JP, Lerner I, Valentin E, et al. Incidence of sudden cardiac death in the European Union. J Am Coll Cardiol. 2022; 79: 1818‑1827. | Crossref
- Zheng ZJ, Croft JB, Giles WH, Mensah GA. Sudden cardiac death in the United States, 1989 to 1998. Circulation. 2001; 104: 2158‑2163. | Crossref
- WHO scientific group on sudden cardiac death and World Health Organization. Sudden cardiac death. Report of a WHO Scientific Group. World Health Organ Tech Rep Ser. 1985; 726: 5‑25.
- Lynge TH, Risgaard B, Banner J, et al. Nationwide burden of sudden cardiac death: a study of 54,028 deaths in Denmark. Heart Rhythm. 2021; 18: 1657‑1665. | Crossref
- Marijon E, Narayanan K, Smith K, et al. The Lancet Commission to reduce the global burden of sudden cardiac death: a call for multidisciplinary action. Lancet. 2023; 402: 883‑936. | Crossref
ARTICLE INFORMATION