Unraveling the enigma: Echinococcus multilocularis in the adrenal gland as a very rare cause of hypertension in a young patient

 CC BY 4.0
CC BY 4.0
Unraveling the enigma: Echinococcus multilocularis in the adrenal gland as a very rare cause of hypertension in a young patient
A 32‑year‑old farmer from the north‑eastern region of Poland was admitted to the Department of Internal Medicine and Hypertension for hypertension and proteinuria diagnosis. On admission, the patient reported reduced exercise tolerance, and chest and lumbar area pain. Physical examination showed elevated blood pressure (150/100 mm Hg) and moderate leg edema. Laboratory tests indicated elevated serum creatinine concentration (1.71 mg/dl; reference range [RR], 0.7–1.2 mg/dl) with decreased estimated glomerular filtration rate (eGFR; 50 ml/min/1.73 m²; RR >60 ml/min/1.73 m²) and proteinuria (1966 mg in a 24‑hour urine collection). The ambulatory blood pressure monitoring recorded mean blood pressure of 141/87 mm Hg, with a “dipper” pattern.
Doppler ultrasound of the renal arteries raised a suspicion of hemodynamically significant left renal artery stenosis. To further investigate, contrast‑enhanced computed tomography (CT) was performed, showing a heterogeneous polycyclic mass with calcification in the anatomical location of the right adrenal gland, involving an adjacent fragment of the liver parenchyma, and smaller lesions of similar appearance in the liver (Figure 1A and 1B).
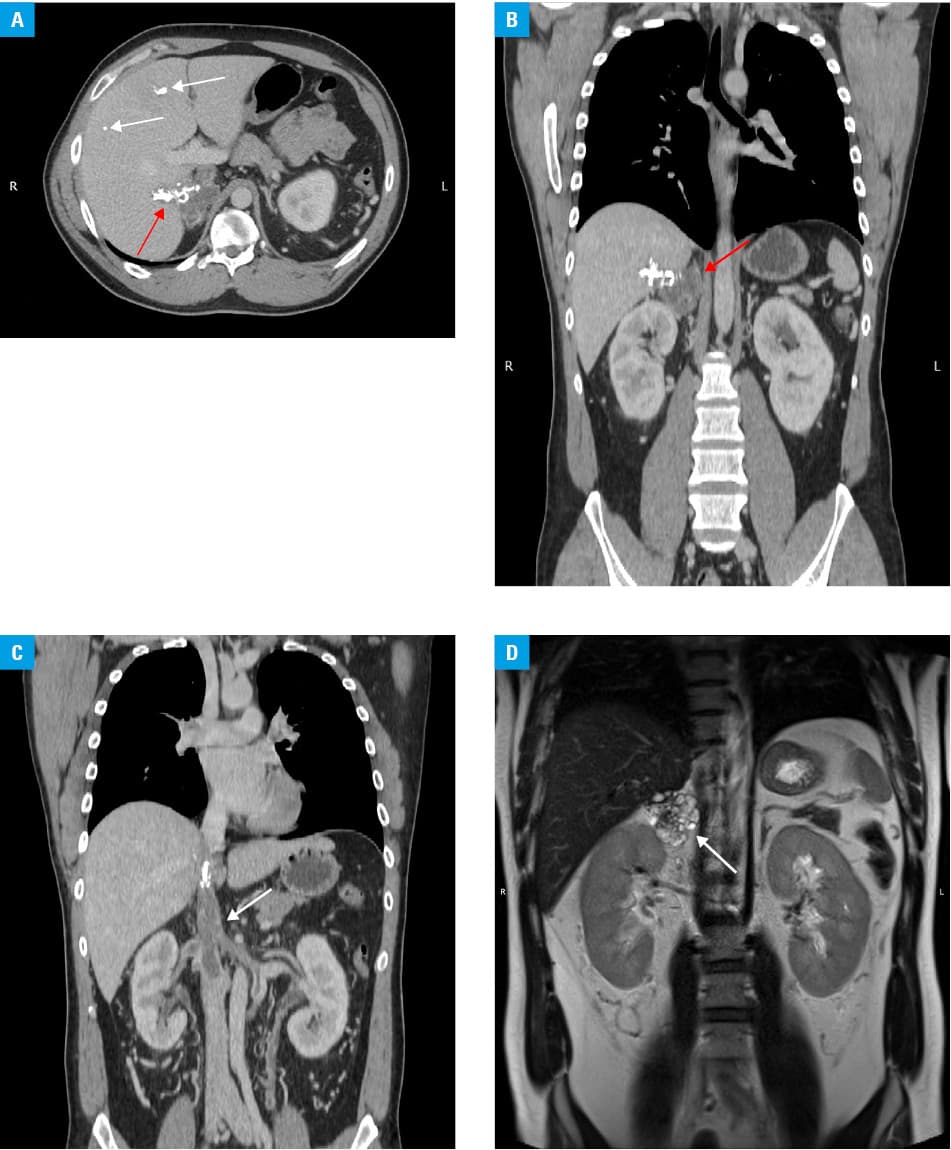
Additionally, the inferior vena cava, at the level of the hepatic vein, was filled with a hypodense thrombus, with trace marginal flow preserved. The renal veins and the right hepatic vein were also filled with hypodense thrombotic material within all the vessels (Figure 1C). Numerous, tortuous, wide veins of collateral circulation were visualized around both kidneys. The kidneys appeared moderately edematous due to venous stasis.
Following the CT results, immediate treatment with enoxaparin was initiated. Due to extensive abdominal venous thrombosis, undiagnosed malignancy was suspected. However, according to a consulting oncologist, the changes described in the imaging tests did not correspond to any type of cancer. Consequently, magnetic resonance imaging of the abdomen was performed, showing a polycyclic mass composed of numerous small cystic structures and signal voids corresponding to calcifications (Figure 1D). Serological tests confirmed the presence of Echinococcus multilocularis, and albendazole treatment was prescribed.
It took 3 hospitalizations to reach the final diagnosis (from July 7 to August 21, 2023). A follow‑up evaluation 4 months after the initiation of treatment showed similar CT findings and improvement in kidney function (with a creatinine level of 1.21 mg/dl and a reduction in 24‑hour proteinuria to 1050 mg). Low‑molecular‑weight heparin was switched to apixaban (5 mg twice daily). Surgery is still planned.
Echinococcus multilocularis is a cause of a disease known as alveolar echinococcosis. Humans are accidental intermediate hosts of the larval stage (metacestode) of a fox tapeworm Echinococcus multilocularis. In 2021, only 26 cases were reported in Poland,1 with the largest number in the Subcarpathian region, followed by Podlaskie (a north‑eastern region).2 A slow growth of the larvae in the asymptomatic phase can last for several years. If left untreated, the condition can be fatal.3 The disease usually primarily involves the liver and exhibits tumor‑like growth. In rare cases, cysts may develop in other organs, such as the adrenal glands or brain.4 The adrenal glands could also be the location of rare nodular lesions, including neoplasms.5
Our case illustrates the potentially severe complications resulting from alveolar echinococcosis, beyond the disease itself.
- European Centre for Disease Prevention and Control. Echinococcosis. In: ECDC. Annual epidemiological report for 2021. Stockholm: ECDC; 2024. https://www.ecdc.europa.eu/en/publications‑data/echinococcosis‑annual‑epidemiological‑report‑2021. Accessed Feb 6, 2024
- Stefaniak M, Derda M, Zmora P, et al. Risk factors and the character of clinical course of the Echinococcus multilocularis infection in patients in Poland. Pathogens. 2023; 12: 199. | Crossref
- Davidson RK, Romig T, Jenkins E, et al. The impact of globalisation on the distribution of Echinococcus multilocularis. Trends Parasitol. 2012; 6: 239‑247. | Crossref
- Mihmanli M, Idiz UO, Kaya C, et al. Current status of diagnosis and treatment of hepatic echinococcosis. World J Hepatol. 2016; 8: 1169‑1181. | Crossref
- Hellmann AR, Szymański M, Śledziński M, et al. “Ancient” Schwannoma of the adrenal gland pretending to be melanoma metastasis. Pol Arch Intern Med. 2022; 132: 16260. | Crossref
ARTICLE INFORMATION