Current practices in diagnosing acute pulmonary embolism: a comprehensive analysis of adherence to contemporary practice guidelines
1,2 Key words: age-adjusted D-dimer, pulmonary embolism response team, Pulmonary Embolism Severity Index score, revised Geneva score, Wells criteria
Key words: age-adjusted D-dimer, pulmonary embolism response team, Pulmonary Embolism Severity Index score, revised Geneva score, Wells criteria



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Current practices in diagnosing acute pulmonary embolism: a comprehensive analysis of adherence to contemporary practice guidelines
Introduction: Acute pulmonary embolism (APE) poses significant diagnostic challenges, with potentially fatal outcomes if not promptly identified and treated. Despite the availability of clinical guidelines, adherence to diagnostic strategies varies globally, impacting patient outcomes.
Objectives: Our aim was to investigate current practices for PE diagnosis among Polish physicians and their adherence to the contemporary 2019 European Society of Cardiology (ESC) guidelines.
Patients and methods: This cross‑sectional study, utilizing a web‑based survey developed with the Delphi methodology, included hospital‑based physicians of various specialties from Poland. The survey focused on diagnostic practices, risk stratification, and adherence to the ESC 2019 guidelines for PE.
Results: The study showed a limited use of guideline‑recommended clinical prediction rules, with predominant reliance on D‑dimer assessment and computed tomography pulmonary angiography. Risk stratification practices varied, and were often based on individual experience rather than evidence‑based strategies. The vast majority of physicians (80.5%) had never contacted a PE response team, but 88% stated that they would if it were available. Cardiologists were more likely to employ guideline‑recommended methods than other specialists.
Conclusions: There is a need for increased adherence to guideline‑recommended diagnostic and risk stratification strategies in APE among physicians in Poland. Enhancing the availability of PE response teams and promoting guideline‑directed practices could improve diagnostic accuracy and patient outcomes.
What's new?
Adherence to guideline‑recommended clinical prediction rules in diagnosing acute pulmonary embolism is limited among physicians in Poland. Reliance on D‑dimers appears to be the most common strategy for assessing probability of the disease. Risk stratification is largely based on individual experience and clinical judgement rather than evidence‑based strategies. The use of diagnostic algorithms and risk assessment models is heterogenous across different medical specialties, with cardiologists most frequently employing guideline‑recommended methods. The use of pulmonary embolism response team–based strategy in making therapeutic decisions is low.
Introduction
Acute pulmonary embolism (APE) is a common and potentially life‑threatening condition that continues to challenge clinicians worldwide.1 Rapid and accurate diagnosis is crucial for optimizing patient outcomes, as delayed or missed diagnoses can lead to significant morbidity and mortality. Over the years, the possibilities of PE diagnosis have evolved significantly, with new diagnostic strategies regularly revised by experts in scientific practice guidelines.1 Nevertheless, following the scientific recommendations, routine practice varies among physicians across the world.2-6 A few studies showed that the adherence to guidelines may improve the accuracy of diagnosis and, most importantly, the outcomes of PE patients.7 Therefore, it is of great clinical importance to encourage and promote guideline‑directed approach to the diagnosis and treatment of PE among physicians of different specialties. However, there is limited evidence on the current use of guideline‑recommended diagnostic strategies in everyday clinical routine. Hence, our study aimed to assess current practices in PE diagnosis and risk stratification among physicians in Poland and to evaluate their adherence to the current European Society of Cardiology (ESC) guidelines.1 We also intended to explore the awareness and attitudes of the physicians toward the concept of PE response teams (PERTs), that is, multidisciplinary teams of specialists dedicated, as recommended by the ESC guidelines, to support the care of PE patients.
Patients and methods
Questionnaire
As the first step of our study, we prepared a web‑based survey using the Delphi methodology.8 First, 3 authors (JS, ŁW, GK) suggested 65 questions, encompassing the following aspects: characteristics of a respondent and the respondent’s workplace, availability of diagnostic and therapeutic modalities, real‑life use of diagnostic, risk stratification, and therapeutic strategies, and in‑hospital and post‑PE care. This set of questions was sent to each author of this document for evaluation from 1 (irrelevant) to 10 (especially relevant). Questions with an average score above 7 were arbitrarily accepted, and those with an average score of 3 or below were rejected. The remaining questions were reassessed by the authors, and either dismissed or modified according to the reviewer’s suggestions. After the second round of the Delphi process, 65 questions were accepted, including 3 additional ones proposed during the first round and accepted in the second.
In this article, we analyze responses to 17 questions relating to current practices in diagnosis and risk stratification of PE.
Data collection
We used a commercially available web‑based survey tool (www.webankieta.pl) to collect the data. We aimed to obtain responses from hospital‑based physicians. All hospital departments of Małopolska, Podkarpacie, and Świętokrzyskie regions were identified using the Polish National Health Fund registries (www.nfz.gov.pl). First, an invitation letter including a link to the survey was emailed to the heads of 647 departments, asking all employed physicians to respond to the questionnaire. Next, a copy of the invitation letter was sent by regular mail to each department. Physicians working in pediatric and psychiatric wards were excluded. The responses were collected between June 20, 2022 and April 30, 2023.
Our analysis is based on responses to 17 questions described in the Supplementary material, Table S1.
Statistical analysis
Categorical variables were described as counts and percentages. Percentages were calculated for a nonmissing sample. To assess differences in selected diagnostic and risk stratification strategies between the groups we used the χ2 test. The Bonferroni correction was applied when several diagnostic and risk stratification parameters were compared between the subgroups. The significance level was set at a P value below 0.01. Statistical analyses were performed with Statistica PL software (StatSoft, Inc., 2017, STATISTICA, version 13.3, Kraków, Poland).
We hypothesized that cardiologists from larger cities, working in hospitals with emergency departments (EDs) have more guideline‑directed clinical practices. Accordingly, the analyses were performed within prespecified subgroups, based on the type of specialization of a responding physician (cardiologists vs noncardiologists), years of clinical experience (up to or over 5), size of the city (up to or above 100 000 inhabitants), presence of an ED in the hospital, and formally approved procedure for diagnosing and treating PE in place.
Results
A total of 376 physicians responded to our invitation to participate in the survey. Response rates to the questions used in this analysis ranged from 77% (288 responses) to 53% (198 responses).
Characteristics of the respondents
All respondents declared to be hospital‑based physicians, primarily working in departments such as cardiology, internal medicine, and ED, with a majority being specialists (Table 1). More than half reported to have a formally approved procedure for diagnosing and treating patients with APE or a dedicated unit for this purpose in their hospitals.
Variable | Characteristics | N, %a |
a Percentages are calculated for nonmissing values. | ||
City population, n | <50 000 | 77 (27) |
50 000–100 000 | 55 (19) | |
100 000–500 000 | 66 (23) | |
>500 000 | 90 (31) | |
Primary workplace | Department of cardiology | 79 (27.4) |
Department of internal medicine | 38 (13.2) | |
Emergency department | 34 (11.8) | |
Department of anesthesiology and intensive care | 28 (9.6) | |
Other | 109 (38) | |
Specialist title | Yes | 196 (74.5) |
No | 67 (25.5) | |
Medical specialty | Cardiology | 73 (27.8) |
Internal medicine | 56 (21.3) | |
Emergency room | 12 (4.6) | |
Anesthesiology and intensive care | 28 (10.6) | |
Other | 94 (35.7) | |
Professional experience, y | <5 | 45 (17.1) |
5–14 | 76 (28.9) | |
>15 | 142 (54) | |
Availability of an admission or emergency department in the hospital | Yes | 270 (93.7) |
No | 18 (6.3) | |
Formal procedure for pulmonary embolism diagnosis and treatment | Yes | 113 (39.2) |
No | 175 (60.8) | |
Dedicated department for the treatment of pulmonary embolism patients | Yes, department of cardiology | 132 (45.8) |
Yes, department of internal medicine | 28 (9.7) | |
Yes, anesthesiology and intensive care unit | 21 (7.3) | |
Yes, department of pulmonology | 6 (2.1) | |
Yes, department of angiology | 2 (0.7) | |
Yes, other | 0 | |
No | 99 (34.4) | |
Use of diagnostic tests and assessment of pulmonary embolism probability
Less than half of the physicians (88; 40%) admitted to routinely using the revised Geneva or Wells clinical prediction rules for assessing the clinical probability of PE, as recommended by the 2019 ESC guidelines (Table 2). A majority of the respondents use them either occasionally (79; 36%) or never (52; 24%), preferring a clinical judgment. In contrast, D‑dimer levels are routinely assessed when diagnosing PE by nearly all respondents (198; 97.5%), but the age‑adjustment of the cutoff values is performed by only two‑thirds of the physicians (131; 65%). Computed tomography pulmonary angiography (CTPA) was reported to be the most commonly used diagnostic modality (189; 93%), whereas the use of echocardiography for diagnosis or risk stratification was reported by 148 physicians (73%).
Variable | N, %a | |
a Percentages are calculated for nonmissing values. | ||
Revised Geneva or Wells clinical prediction rules | Routine use | 88 (40) |
Occasional use | 79 (36) | |
No use, only clinical judgement | 52 (24) | |
D‑Dimers | Routine use | 198 (97.5) |
No use | 5 (2.5) | |
Age‑adjusted D‑dimer | Routine use | 131 (64.5) |
No use | 72 (35.5) | |
Computed tomography pulmonary angiography | Routine use | 189 (93) |
No use | 14 (7) | |
Echocardiography | Routine use | 148 (73) |
No use | 55 (27) | |
Subgroup analyses on the use of diagnostic tests and assessment of pulmonary embolism probability
Cardiologists use echocardiography and D‑dimer age‑adjustment more commonly in their routine practice than noncardiologists (Figure 1, Supplementary material, Table S2). The presence of an ED is associated with the most frequent application of CTPA and D‑dimers for the PE diagnosis.
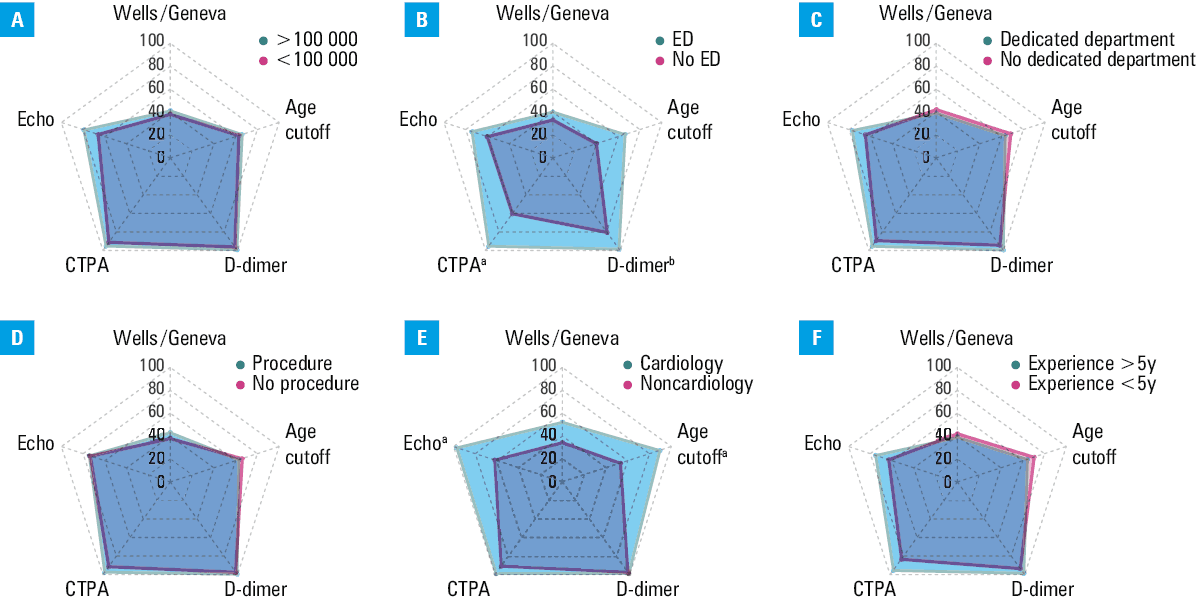
a Significant difference for P <0.001
b Significant difference for P <0.01
Risk assessment in acute pulmonary embolism patients
As presented in Figure 2, the most frequently used markers of prognosis in acute PE, reported by over 90% of the respondents, are blood pressure, oxygen saturation, and severity of symptoms, followed by heart rate, presence of a saddle thrombus on CTPA, blood troponin levels, right ventricular function on echocardiography, presence of central clots, and levels of N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP). An expression “massive PE” on CTPA is considered a prognostic marker by 167 respondents (78.8%). The least commonly used risk predictors are the Bova scale, right‑to‑left ventricular ratio (RV/LV) on CTPA, and Pulmonary Embolism Score Index (PESI) or simplified PESI (sPESI) score.
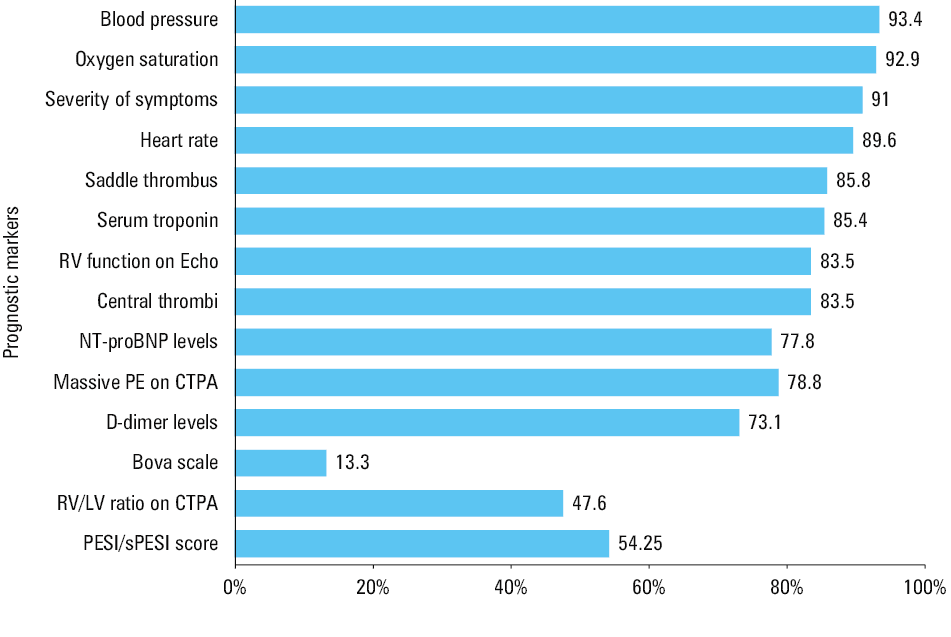
Abbreviations: CTPA, computed tomography pulmonary angiography; Echo, echocardiography; LV, left ventricle; NT‑proBNP, N‑terminal pro–B‑type natriuretic peptide; PE, pulmonary embolism; sPESI, simplified Pulmonary Embolism Severity Index; RV, right ventricle
Subgroup analyses of risk assessment in acute pulmonary embolism patients
Cardiologists are more likely than noncardiologists to use cardiac troponin levels, RV function on echocardiography, RV/LV ratio on CTPA, PESI/sPESI scores and NT‑proBNP levels for risk assessment (Figure 3, Supplementary material, Table S3). In hospitals with an ED, the echocardiography‑assessed RV function is used more often for prognosis than in hospitals without an ED.
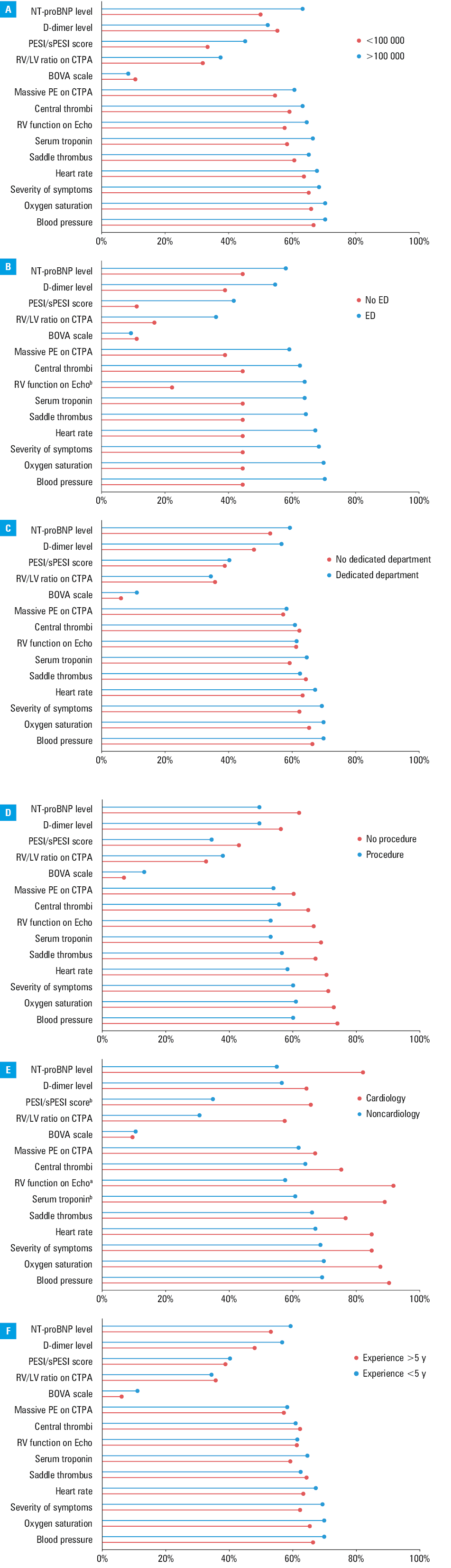
a Significant difference for P <0.001
b Significant difference for P <0.01
Abbreviations: see Figure 2
Contacting pulmonary embolism response team for consultation
As many as 203 physicians (80.5%) have never consulted their acute PE patients with a PERT, despite the fact that 221 (88%) reported that they would if the PERT was available (Figure 4). In general, the responding physicians would seek PERT’s advice on patients without shock but with severe symptoms despite initial anticoagulation, on patients with shock and contraindications to systemic fibrinolysis, and on patients without shock or signs of RV dysfunction but with a diagnosis of massive PE on CTPA. As many as 74 respondents (29.4%) declared that they would consult a PERT on any PE patient with shock.
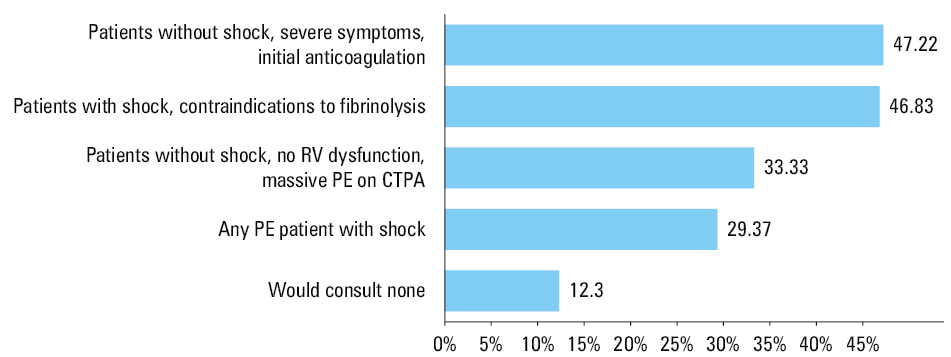
Abbreviations: see Figure 2
Subgroup analyses on seeking pulmonary embolism response team advice
The cardiologists and physicians with over 5 years of clinical experience would more often consult patients with shock and coexisting contraindications to systemic thrombolysis than the noncardiologists or physicians with a shorter experience (Supplementary material, Table S4), whereas the noncardiologists would more often consult patients without shock or signs of RV disfunction but with massive PE on CTPA (11 [15%] vs 72 [38%]; P = 0.002). Interestingly, doctors who once contacted PERT, would seek its advice again for every PE patient.
Discussion
In this cross‑sectional study we present a comprehensive view on current clinical practices in the diagnosis and risk stratification of PE among hospital‑based physicians from Poland. We received answers from physicians representing a majority of hospital‑based medical specialties and a wide spectrum of clinical expertise. There was a well‑balanced distribution of responders originating from cities of all sizes and representing hospitals of different levels of reference. Eventually, there was a proportional ratio of respondents working in medical centers with and without dedicated procedures or departments for diagnosing and treating patients with PE.
We found that the use of clinical prediction rules for assessing the clinical probability of PE, such as the revised Geneva score or the Wells criteria, as recommended by the guidelines, is low. This is in line with previous observations from across the world, reporting that in up to 80% of patients, clinicians do not use them or use them incorrectly.2,3 We also learned from our study that utilization of the rules was low independently of the medical specialty, clinical experience, or availability of a formal PE diagnostic procedure. In contrast, the use of D‑dimers as a routine diagnostic strategy was reported by nearly all respondents, and only among clinicians from hospitals with no ED its frequency was slightly lower. Additionally, we found that many physicians have not adopted the age‑adjustment of D‑dimer cutoffs in their practice despite supporting evidence and the guidelines.1,9 The reluctance toward recommended probability assessment strategies among the respondents may preserve the pursue for excessive use of imaging, which is widely observed around the world.10,11 On the other hand, these findings may as well reflect the fact that for some physicians the use of prediction rules or D‑dimer age‑adjustment may feel impractical in everyday practice, as compared with experience‑based approach. Their decision to order imaging may be influenced by fear of missing PE, potentially overriding clear advantages of adhering to evidence‑based algorithms, which represents the so‑called defensive rather than evidence‑based medicine. The use of CTPA was very common among the respondents in our study, showing that, similarly to other regions worldwide, it is a modality of choice for PE diagnosis in Poland.12-15
Although not mandatory for establishing the diagnosis of APE, echocardiography may provide a range of valuable diagnostic and prognostic clues and, in some cases, justify immediate initiation of reperfusion treatment. Despite this, early use of echocardiography has been identified in less than half of cases in recent studies.16-19 As many as 73% of the respondents in our study declared the use of echocardiography as a standard‑of‑care, but this number was lower among noncardiologists (62%). It is therefore of a great potential clinical benefit to increase availability of echocardiography and encourage training, especially among this group of health care providers.
Identifying patients at the greatest risk of early death is another critical step in the diagnostic and therapeutic PE pathway. Risk stratification should begin already upon initiation of the diagnostic workup and should apply to every patient. Cardiac arrest, hypotension, and end‑organ hypoperfusion define the highest‑risk group, whereas the presence of clinical, imaging, and laboratory markers of RV dysfunction but without concomitant arterial hypotension identifies patients at intermediate‑high risk. Accordingly, our study showed that blood pressure, oxygen saturation, and heart rate were the most commonly used markers of the worst outcome among the respondents. This indicates that in an immediate life‑threatening APE scenario, physicians correctly rely on fundamental signs of cardiopulmonary compromise. On the other hand, in patients who present without hemodynamic instability, individual baseline findings alone may be insufficient to determine PE severity and early PE‑related risk. The vast majority of respondents declared to base their risk stratification on such parameters as the severity of symptoms, the presence of a saddle thrombus or the massive PE finding on CTPA. Despite how easy‑to‑use these parameters may seem, there exist limited or, at best, conflicting scientific evidence of their actual utility for this purpose.20,21 Instead, the guidelines recommend to apply validated scores combining clinical, imaging, and laboratory PE‑related prognostic factors, such as the PESI/sPESI score, the RV/LV ratio, cardiac troponin levels, or the BOVA scale. We have learned from our study that such guideline‑directed approach has been poorly adopted by Polish physicians so far. Barely half of them reported the use of these parameters in their daily practice. The cardiologists were found to be the most familiar with the contemporary risk stratification modalities. Also, the respondents from the medical centers with the ED on site, and those who had ever consulted a PE patient with a PERT, were more commonly using the guideline‑recommended strategies. This highlights the need for wider distribution of knowledge on modern risk assessment strategies. It may also reflect the positive impact that a PERT can have on disseminating up‑to‑date knowledge on best practices in the PE care. In general, the primary role of a PERT is to consult, advise, and execute reperfusion treatment if needed. The PERT concept has recently gained rapid recognition around the world, but its usefulness has yet to be proven.22-24 Nonetheless, the exchange of knowledge and experience takes place at any step of a PERT consultation, and therefore often has a positive effect on all stakeholders. Not surprisingly, most of the respondents declared that they would contact a PERT for consultation, if only it were available. Unfortunately, as found in our recent publication, only 8.3% of physicians declared having a 24‑hour access to PERT consultations in their workplace, and only 28.4% in another hospital.25 The respondents would most frequently consult patients with shock and concomitant contraindications to fibrinolysis and patients with signs of RV disfunction who do not improve on anticoagulation. This is in line with previously published data showing that high‑risk and intermediate‑high risk PE patients are the most common PE patient groups consulted by PERTs.26 These are by far the most complicated and not so infrequent PE patients, who are often diagnosed and initially treated in non‑PERT medical centers. Our study found that the need for widely available PERT consultations is even greater, as one‑third of the respondents declared that they would consult any patient with shock, and another 30% would consult any patient with massive PE on CTPA, irrespective of the clinical presentation. Therefore, raising awareness of PERTs and novel PE therapies, and building networks of PERTs with regional medical centers could reduce disparities in the access to the state‑of‑the‑art diagnostic strategies and modern therapies, ultimately improving outcomes for patients.
Limitations
A few limitations of our study should be mentioned. The focus on Polish medical practices may limit the generalizability of the findings to other health care systems; however, some similarities to previously published data2-6 have been identified, such as limited use of prediction rules and potential overuse of CT imaging. A lack of a direct correlation between diagnostic strategies and patient outcomes may be regarded as a limitation of the study, as it could provide more conclusive evidence. The aim of the study, though, was to understand the current practices in the diagnosis of PE to identify potential areas of improvement to be addressed in the future. The study utilized a web‑based survey, which might introduce selection bias, as it relied on voluntary participation, potentially skewing results toward more engaged or technologically adept respondents. Limited rate of responses may also be regarded as a study drawback. On the other hand, the number of gathered responses may reflect only those physicians who have actual experience or a dedicated interest in PE care. If this were the case, then the actual awareness and knowledge of PE management would be even more limited.
Despite limitations, we believe that the study provided a valuable examination of current clinical practices in the diagnosis and risk stratification of PE, giving insights into the adherence to clinical practice guidelines almost 5 years after their publication. The originality of the study is the inclusion of various medical specialties from different hospital across the southern Poland. Its novelty lies in the fact that it assessed the actual use of risk assessment strategies, as such data have been limited so far. Also, capturing the respondent views on the most recent development in the management of PE patients, the PERTs, is a unique advantage of this study.
Conclusions
Adherence to guideline‑recommended clinical prediction rules in the diagnosis of acute PE is limited among physicians in Poland, and the reliance on D‑dimer appears to be the most common strategy. Risk stratification is largely based on individual experience and clinical judgement rather than evidence‑based strategies. The use of diagnostic algorithms and risk assessment models is heterogenous across different medical centers and medical specialties, with cardiologists from larger hospitals most frequently employing guideline‑recommended methods. By incorporating their expertise early in the PE management process, but also by broadening the knowledge and improving the skills of noncardiologists, general improvement in diagnostic precision could be expected. There is a high demand for the assistance of PERTs in the management of PE patients. Increasing the availability of PERTs and their cooperation with regional medical centers should become a nationwide number one initiative to reduce disparities in access to modern therapies and to improve patient care.
- Konstantinides SV, Meyer G, Becattini C, et al. The 2019 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2019; 40: 3453‑3455. | Crossref
- Hsu N, Soo Hoo GW. Underuse of clinical decision rules and D‑dimer in suspected pulmonary embolism: a nationwide survey of the Veterans Administration healthcare system. J Am Coll Radiol. 2020; 17: 405‑411. | Crossref
- Elias A, Schmidt J, Bellou A, et al. Opinion and practice survey about the use of prognostic models in acute pulmonary embolism. Thromb Res. 2021; 198: 40‑48. | Crossref
- Almarshad F, Alaklabi A, Raizah AA, et al. Diagnostic approach and use of CTPA in patients with suspected pulmonary embolism in an emergency department in Saudi Arabia. Blood Res. 2023; 58: 51‑60. | Crossref
- Al Dandan O, Hassan A, Alnasr A, et al. The use of clinical decision rules for pulmonary embolism in the emergency department: a retrospective study. Int J Emerg Med. 2020; 13: 23. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION