Five-year mortality disparities across urban and rural areas in patients treated with coronary artery bypass grafting

 CC BY 4.0
CC BY 4.0
Five-year mortality disparities across urban and rural areas in patients treated with coronary artery bypass grafting
Introduction
Coronary artery disease (CAD) remains one of the major causes of morbidity. An evaluation of genetic and lifetime factors can be important for public health improvement initiatives. Multivessel coronary disease can be effectively treated with surgical or percutaneous interventions. Compared with medical therapy, coronary revascularization is associated with long‑term reduction in the number of recurrent events and superior long‑term survival. However, the former is crucial to procedural outcomes. Long‑term results following surgical intervention have been related to preoperative factors, such as diabetes, hyperlipidemia, and smoking.1 Clinical attention cannot achieve optimal results without personalized therapy for comorbidities, including arterial hypertension, diabetes mellitus, and dyslipidemia.
Currently, it is believed that environmental factors represent a group of nontraditional risk factors for morbidity and premature mortality. It has been recently postulated that air pollution has an impact on human health, including the risk of CAD.2
In their review, Miller et al3 underlined the significance of the influence of inhaled particle matter (PM) on the cardiovascular system. The relationship between traffic air pollution in metropolitan areas and the prevalence of CAD has already been presented, just as the incidence of myocardial infarction. Mena et al4 noted geographical differences and disparities in the incidence of cardiovascular events related to the living environment (urban vs rural). It is emphasized that in order to improve cardiovascular health, multiple strategies of tackling air pollution should be addressed. However, though it has been postulated that air pollution has a negative impact on cardiovascular morbidity and mortality, its significance in patients who have already undergone surgical coronary artery revascularization is less known.
The aim of the study was to evaluate the value of clinical and environmental factors, in terms of the place of habitation and related air pollution exposure, for long‑term mortality in patients treated with surgical coronary artery revascularization.
Patients and methods
Our single‑center retrospective analysis included 427 patients (369 [86%] men and 58 [14%] women) with a median (interquartile range [IQR]) age of 64 (59–70) years, who underwent CAD surgery with the use of off‑pump revascularization technique at our Cardiac Surgery Department in 2014 and 2016, and were followed up to September 30, 2020 (Supplementary material, Figure S1) for a median (IQR) period of 5.5 (4.8–6) years. The study group comprised 303 patients (71%) with multivessel CAD and 124 individuals (29%) with left main CAD, all of whom were qualified for surgical revascularization based on the decision of the heart team.
We analyzed the clinical characteristics and air pollution exposure of patients from western and central parts of Poland. These regions have similar population density and socioeconomic status. Main sources of air pollution include road traffic, industry, heating, and agriculture. Urban areas were classified as cities with over 50 000 citizens, and rural areas were defined as open country settlements with fewer than 5000 residents. None of the participants reported having in‑home air conditioning. The individual analysis included the time between surgery and the established follow‑up point (September 30, 2020) or time of death.
Demographic and clinical factors were collected. Blood samples were obtained for complete blood count and biochemical and lipid profiles. Dyslipidemia was diagnosed based on the current guidelines5 or a history of lipid‑modifying therapy.
In all patients, echocardiography was performed on admission, postoperatively, and at discharge by the same team of experienced cardiologists following the same protocol.
Mortality during follow‑up was evaluated based on the national health care database and direct contact with patients or their families, including ambulatory clinic visits and phone calls.
Air pollutant exposure
Three health‑relevant air pollutants were considered for our study: PM with a diameter of 10 microns or less (PM10), PM with a diameter of 2.5 microns or less (PM2.5) and nitrogen dioxide (NO2). The exposure analysis was personalized for each patient and presented as median (IQR) values through the entire follow‑up period.
Exposure level of individual patients was assessed using spatial distributions of air concentration fields across Poland, as provided by the Chief Inspectorate of Environmental Protection. Maps of PM10, PM2.5, and NO2 were derived from the National Air Quality Modelling (NAQM) system, elaborated by the Institute of Environmental Protection – National Research Institute in Poland, in line with the Polish Environmental Protection Act (article 66, paragraph 6). The NAQM database contains 2 kinds of maps: 1) high‑resolution bottom‑up emission inventory maps of air pollutants, stored in the Central Emission Database,6 and 2) air concentration maps elaborated using the Global Environmental Multiscale with Air Quality processes (GEM‑AQ) model, which operates in the Copernicus Atmosphere Monitoring Service–Regional Production.7
High‑resolution annual emission maps were created based on Standard Nomenclature for Air Pollution categories. The GEM‑AQ is a semi‑Lagrangian chemical weather model developed at the Environment Canada, which implements air quality processes and tropospheric chemistry into the analysis. The weather prediction model was based on the Global Environmental Multiscale.8 The final air quality maps were created using a 0.025‑degree resolution grid, with higher resolution in densely populated areas (eg, cities and agglomerations).
All air pollutant concentrations in residential areas (approximately 250 m buffer zones) were estimated using downscaling statistical methods. These methods relied on land use variables and the Expert‑in‑the‑loop Stepwise Regression procedure developed in the Neurosmog project.9 The personalized ambient air exposure was also evaluated for real‑life data from air quality monitoring stations operating in the State Environmental Monitoring program.10 The air pollutant exposure was estimated on the basis of mean values estimated for the place of residence (based on the distance from measurement stations).
Statistical analysis
The normality of distribution of variables was tested with the Shapiro–Wilk test. The t test, Cox regression test or Mann–Whitney test, or the Fisher exact test were used where applicable to compare the variables between the 2 groups. Finally, backward logistic regression analysis based on demographic, clinical, and intraoperative factors combined with air pollution exposure was performed to identify predictors of long‑term mortality within a 5‑year observation period. Statistical analysis was performed using Statistica 13 by TIBCO (Statsoft, Kraków, Poland). P value below 0.05 was considered significant.
Ethics statement
Informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Poznan University of Medical Sciences (55/20) for human studies.
Results
During the median (IQR) 5.5 (4.8–6)-year follow‑up period, 56 patients (13%) died, none perioperatively. The comorbidities included arterial hypertension (n = 336; 79%), dyslipidemia (n = 238; 56%), and diabetes mellitus (n = 148; 35%). The median (IQR) body mass index was 28.4 kg/m2 (26.2–30.8 kg/m2). As many as 139 patients (33%) were diagnosed as overweight.
The median (IQR) number of anastomoses was 2 (2–3). All procedures were performed through median sternotomy using the off‑pump technique (off‑pump coronary artery bypass grafting). Arterial revascularization was conducted in 19 patients (4%). None of them required intraoperative conversion to cardiopulmonary bypass. No low‑cardiac output syndrome or perioperative myocardial infarction was observed. The median (IQR) hospitalization time was 10 (8–12) days. In the perioperative period, all patients were treated with β-blockers, antiplatelets, statins, and angiotensin‑converting enzyme inhibitor / angiotensin II receptor blockers, with continued optimal medical pharmacotherapy recommended after discharge.
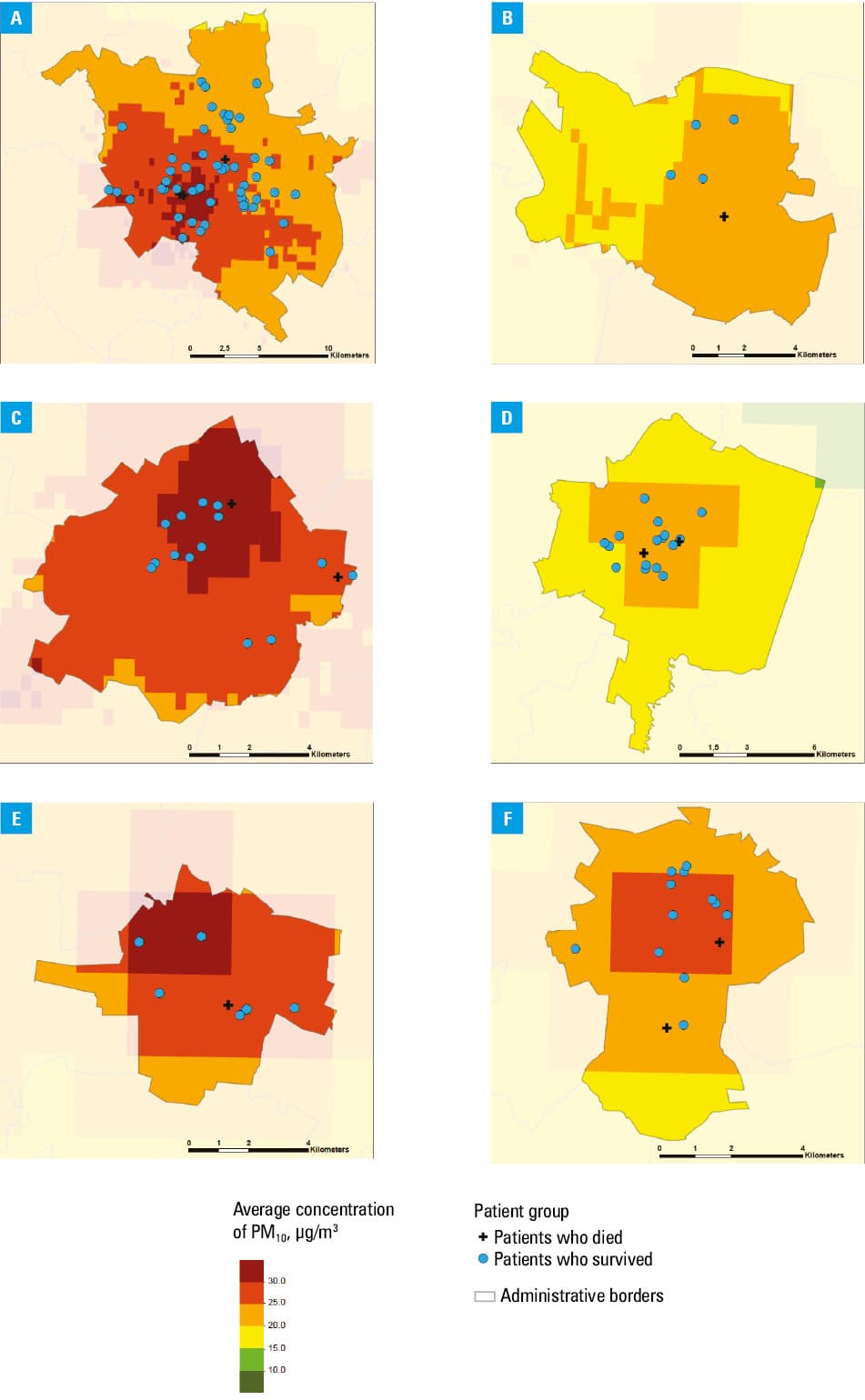
The patients were divided according to a prediction of long‑term mortality risk factors based on their place of residence (Figure 1). They were classified as urban residents (city over 50 000 inhabitants), representing a group of 130 patients (30%), and rural residents (297 patients; 70%).
No significant differences were observed regarding demographic and clinical profiles of the groups (Supplementary material, Table S1).
Subsequently, uni- and multivariable analyses based on demographic, clinical, and intraoperative factors combined with air pollution exposure were performed to establish the predictors of 5‑year mortality in both subgroups.
In the urban group (group 1), the multivariable analysis showed a predictive value of left ventricular ejection fraction (LVEF) of less than 50% (hazard ratio [HR], 4.4; 95% CI, 1.41–13.85; P = 0.01) and PM10 exposure (HR, 1.15; 95% CI, 1–1.32; P = 0.04). Disparities between mortality and ambient PM10 exposure of the urban patients are depicted in Supplementary material, Figure S1 and Table S2.
The multivariable analysis of the rural group (group 2) showed a predictive value of LVEF of less than 50% (HR, 3.59; 95% CI, 1.79–7.23; P <0.001) and dyslipidemia (HR, 2.08; 95% CI, 1.04–2.83; P = 0.03; see Supplementary material, Table S3).
Discussion
The presented analysis highlights the urban / rural disparities in all‑cause long‑term mortality rates related to air pollution exposure. After adjusting for clinical and intraoperative factors, PM10 exposure was shown to be a strong predictor in urban environments, distinct from its influence in the rural ones. We analyzed the median values of air pollutant exposure. Our study presents the median values of NO2, PM2.5, and PM10 within a 5‑year period, indicating a 14% risk increase per each PM10 unit growth that also distinguished urban and rural areas.
Our analysis identified possible risk factors for all‑cause mortality in 5‑year follow‑up after surgical coronary artery revascularization. Among clinical characteristics, reduced LVEF and dyslipidemia are strong predictors of fatal events. Urban citizens living in a city environment are exposed to air pollutants, which can be considered a mortality indicator. Our retrospective analysis pointed out the ominous influence of PM10 exposure on late mortality.
Separate analyses for urban and rural locations showed reduced LVEF as the most significant factor for both subgroups. The relation between LV dysfunction and increased risk of hospitalization and mortality is well documented.11 Despite advances in pharmacotherapy, patients with low LVEF are at a higher mortality risk due to arrhythmias and heart failure deterioration.12 Therefore, Shen et al13 offered a novel approach to medical therapy, emphasizing accelerated up‑titration schedule and optimized ordering of treatment. Moreover, dyslipidemia is a well‑known morbidity and mortality predictor, which our study confirmed. Still, there is a place for other factors to explain some of the residual morbidity and mortality risks. Our study confirms the negative consequences of air pollution for human health. Chronic exposure to PM10 was harmful for patients with coronary artery disease in the analysis by Occelli et al14. Proximity to high‑traffic roads increases exposure to heavy metals, pollutants such as NO2, PM10, and PM2.5, and the risk of cardiovascular complications.
The novelty of our analysis comes from the differences in possible mortality risk after coronary revascularization in the patients living in urban and rural environments. According to our analysis, showing the 5‑year all‑cause mortality risk, PM10 can be regarded as a significant risk factor in urban settings. Our previous report15 showed the progression of atherosclerotic changes in patients with CAD in response to greater air pollution exposure.
Chronic exposure to ambient air pollutants exerts complex pathophysiological effects on human organisms. These phenomena include endothelial or autonomic dysfunction and systemic reactions, such as inflammatory activation, generation of oxidative stress, impaired vegetative nervous system functioning, and increased activity of the hemostatic system.16
Choi et al17 presented the complement system activation and inflammatory reaction regulation by urban PM. They showed possible mechanisms behind the relationship between cardiovascular diseases and air pollution through the interaction between endothelial cells and dysregulation of the complement system. Importantly, there are differences in various geographic areas concerning air pollution compounds.18 Konduracka et al19 reported an increased daily number of hospital admissions related to short‑term increases in PM2.5 levels in a large city in southern Poland, while the effect of PM10 was significant during a simultaneous decrease in temperature. Kuzma et al18,20 showed a higher incidence of hospitalizations due to acute coronary syndrome associated with air pollution in the eastern part of Poland, especially in younger individuals, women, residents of rural areas, and those with lower income. Air pollution may also aggravate the episodes of chronic obstructive pulmonary disease and increase the risk of hospital admission.21 Short- and long‑term exposure to air pollution may affect cardiovascular survival.22,23
Strengths and limitations
The presented analysis is based on data collected from 427 patients followed for 5 years. We demonstrated the utility of joined clinical and environmental analysis to reveal factors influencing long‑term outcomes that are not routinely pointed out in daily practice. A limitation of the study is the fact that we analyzed all‑cause mortality without differentiating it from cardiovascular or pulmonary causes of death.
Conclusions
Chronic exposure to PM10 can be regarded as a significant long‑term mortality risk factor for the urban citizens, following surgical revascularization. Reduced LVEF is a strong clinical indicator of all‑cause mortality. These findings suggest that air pollution exposure increases the risk of mortality despite optimal surgical treatment of CAD. Modern pharmacotherapy, advanced percutaneous and surgical procedures, and lifestyle changes are not enough to improve survival if environmental problems are not addressed. Therefore, national health management policies need to address these issues to reduce mortality rate and improve medical outcomes.
- Leviner DB, Zafrir B, Jaffe R, et al. Impact of modifiable risk factors on long‑term outcomes after coronary artery bypass surgery. Thorac Cardiovasc Surg. 2021; 69: 592‑598. | Crossref
- Urbanowicz T, Lesiak M, Skotak K, et al. Coronary artery culprit lesions progression and temperature exposure ‑ personalized analysis. Adv in Interventional Cardiol. 2024; 20: 139‑147. | Crossref
- Miller MR, Newby DE. Air pollution and cardiovascular disease: car sick. Cardiovasc Res. 2020; 116: 279‑294. | Crossref
- Mena C, Sepúlveda C, Fuentes E, et al. Spatial analysis for the epidemiological study of cardiovascular diseases: a systematic literature search. Geospat Health. 2018; 13: 587‑598. | Crossref
- Mach F, Baigent C, Catapano AL, et al; ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020; 41: 111‑188.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION