Immunoglobulin A vasculitis with Koebner phenomenon and renal involvement induced by antitumor necrosis factor α therapy in the treatment of rheumatoid arthritis

 CC BY 4.0
CC BY 4.0
Immunoglobulin A vasculitis with Koebner phenomenon and renal involvement induced by antitumor necrosis factor α therapy in the treatment of rheumatoid arthritis
Tumor necrosis factor α (TNF-α) inhibitors have shown excellent therapeutic results in the treatment of inflammatory bowel disease and rheumatoid arthritis (RA). However, due to their immunogenicity and potential role in inducing autoantibody formation, they may be associated with adverse effects, such as allergic reactions, thromboembolic events, or autoimmune responses (lupus‑like syndrome or vasculitis). Immunoglobulin (Ig) A vasculitis is an extremely rare complication of TNF-α inhibitor therapy, described in only a few cases of ulcerative colitis, Crohn disease, and RA.1-4
We present a case of a 31‑year‑old woman with RA and a history of TNF-α inhibitor therapy (certolizumab‑pegol) complicated by development of IgA vasculitis.
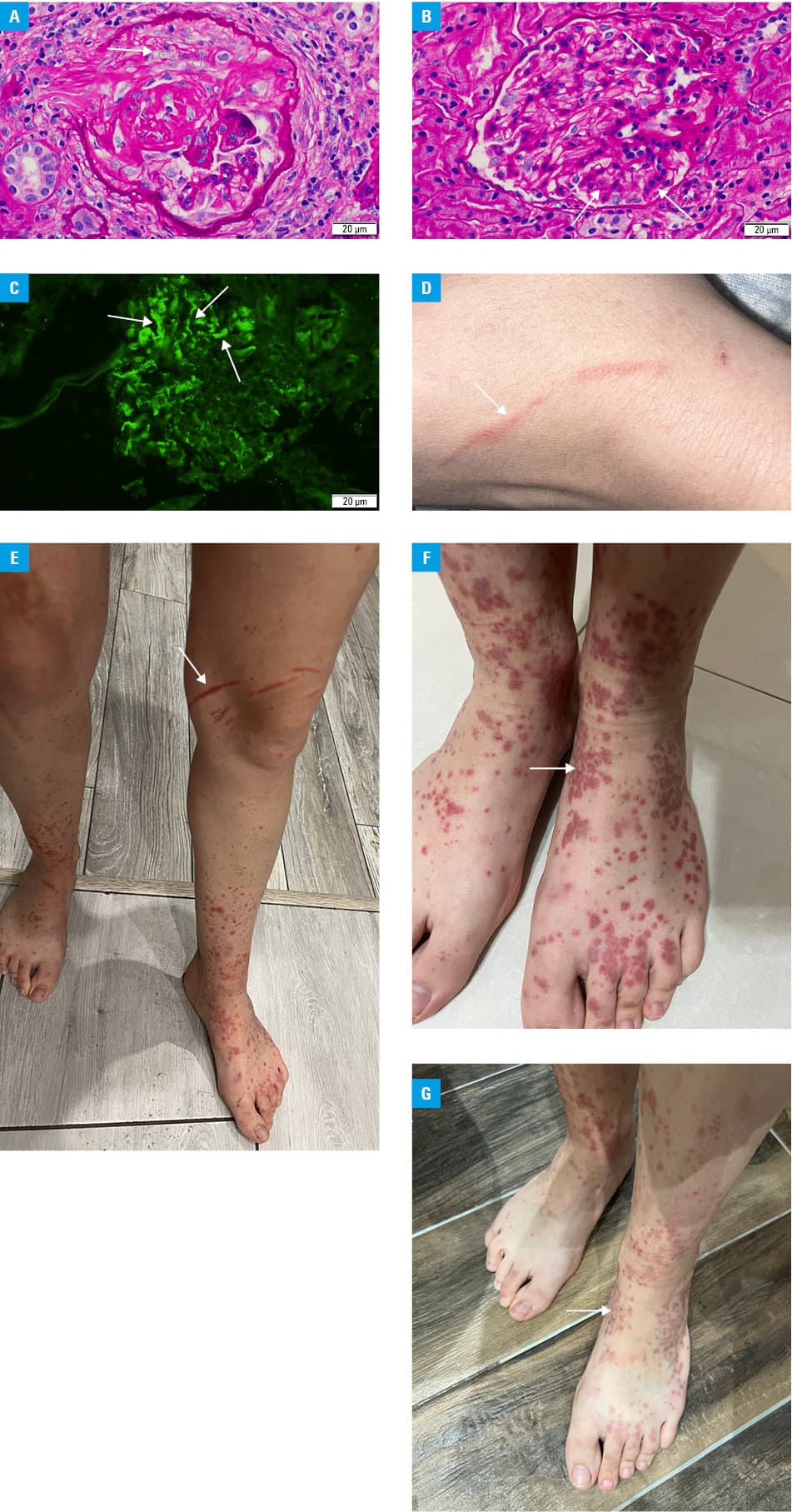
The patient was admitted to our nephrology department due to the presence of erythrocyturia (50–70 cells/µl; reference range [RR] <13.6 cells/µl) and proteinuria (300 mg/dl; RR <15 mg/dl) with preserved renal function. The patient had elevated plasma IgA (429 mg/dl; RR, 70–400 mg/dl) and anticyclic citrullinated peptide (361 U/ml; RR <7 U/ml). Renal biopsy showed mesangial proliferative glomerulonephritis with the presence of crescents and immunofluorescent deposits of IgA, IgG, IgM, fibrinogen, and C1q (Figure 1A–1C). Based on the biopsy results and clinical picture, IgA vasculitis was diagnosed. In addition, increased pain was observed in the left shoulder, hand and foot joints, accompanied by stiffness and limited range of motion. The patient was previously treated for RA with methotrexate and steroids for 1 year. The therapy was discontinued during pregnancy, then the patient was treated with certolizumab and prednisone for 2 years, until another pregnancy, when treatment was terminated. Again, certolizumab treatment was resumed 3 months after the end of the second pregnancy and then therapy was discontinued after 4 months due to the onset of purpura involving the skin of the lower and upper extremities with the presence of Koebner phenomenon (Figure 1D–1G). The skin lesions resolved after discontinuation of certolizumab‑pegol.
Mycophenolate mofetil (2 × 1000 mg) and prednisolone were used for glomerulonephritis. After 3 months of therapy, it was decided to switch to rituximab due to a lack of response and increased joint pain according to the European Alliance of Associations for Rheumatology recommendations. Methotrexate was also added to the RA treatment regimen.5 The patient received 2 doses of rituximab (1000 mg by infusion) at 2‑week intervals with methotrexate (10 mg subcutaneously once a week) along with maintenance prednisone therapy at a reduced dose. The proposed treatment provided a favorable outcome in terms of effective pain relief and improvement in the patient’s well‑being. After 1 month, remission of both RA symptoms and IgA vasculitis was observed. The aforementioned therapeutic option could be considered as the treatment of choice for RA coexisting with TNF-α inhibitor–induced IgA vasculitis.
To the best of our knowledge, this is the first case of a patient with mesangial proliferative glomerulonephritis with the presence of crescents suffering from RA and IgA vasculitis who was successfully treated with rituximab and methotrexate. Careful consideration of the patient’s overall clinical picture and awareness of current guidelines are essential to optimize therapy and reduce adverse drug reactions.
- Jani M, Dixon WG, Chinoy H. Drug safety and immunogenicity of tumour necrosis factor inhibitors: the story so far. Rheumatology (Oxford). 2018; 57: 1896‑1907. | Crossref
- Sokumbi O, Wetter DA, Makol A, et al. Vasculitis associated with tumor necrosis factor-α inhibitors. Mayo Clin Proc. 2012; 87: 739‑745. | Crossref
- Hokama A, Sonosaki T, Zamami R, et al. Crohn disease complicated by IgA vasculitis during therapy with tumor necrosis factor-α inhibitor. Pol Arch Intern Med. 2019; 129: 283‑284. | Crossref
- Karasawa K, Iwabuchi Y, Kyoda M, et al. Primary IgA vasculitis with nephritis in a patient with rheumatoid arthritis diagnosed by anti‑galactose‑deficient IgA1 Immunostaining. Intern Med. 2019; 58: 2551‑2554. | Crossref
- Smolen JS, Landewé RBM, Bergstra SA, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease‑modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023; 82: 3‑18. | Crossref
ARTICLE INFORMATION